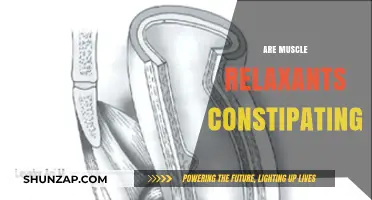
Muscle relaxants and analgesics are two distinct classes of medications often used in pain management, but their mechanisms of action and intended purposes differ significantly. While analgesics, such as nonsteroidal anti-inflammatory drugs (NSAIDs) or opioids, primarily target pain perception by acting on the central nervous system or reducing inflammation, muscle relaxants work by alleviating muscle spasms and tension through their effects on the nervous system or directly on muscle fibers. Although both types of medications can provide relief in certain pain conditions, muscle relaxants are not classified as analgesics because they do not directly address pain pathways. Instead, they are often prescribed alongside analgesics to manage musculoskeletal pain by reducing muscle stiffness and improving mobility. Understanding the differences between these medications is crucial for effective pain management and avoiding potential misuse or confusion in treatment approaches.
| Characteristics | Values |
|---|---|
| Definition | Muscle relaxants are medications that relieve muscle spasms and stiffness. |
| Analgesic Classification | Muscle relaxants are not classified as analgesics (pain relievers). |
| Mechanism of Action | Act on the central nervous system or directly on muscles to reduce spasms. |
| Primary Use | Treatment of musculoskeletal conditions (e.g., back pain, sprains). |
| Pain Relief | May indirectly reduce pain by alleviating muscle tension, but not primary analgesics. |
| Examples | Cyclobenzaprine, Baclofen, Tizanidine, Methocarbamol. |
| Side Effects | Drowsiness, dizziness, dry mouth, fatigue. |
| Analgesic Comparison | Analgesics (e.g., NSAIDs, opioids) directly target pain pathways. |
| Medical Consensus | Muscle relaxants are distinct from analgesics but may complement pain management. |
Explore related products






What You'll Learn
- Definition and Classification: Differentiating muscle relaxants and analgesics based on their primary mechanisms and uses
- Mechanism of Action: How muscle relaxants and analgesics work in the body to relieve pain
- Indications and Uses: Conditions treated by muscle relaxants versus those managed by analgesics
- Side Effects and Risks: Comparing potential adverse effects of muscle relaxants and analgesics
- Combination Therapy: Exploring the use of muscle relaxants and analgesics together for pain management
![]()
Definition and Classification: Differentiating muscle relaxants and analgesics based on their primary mechanisms and uses
Muscle relaxants and analgesics, though often prescribed together, serve distinct purposes in managing pain and discomfort. Muscle relaxants primarily target the central nervous system or neuromuscular junction to reduce muscle spasms and tension, while analgesics focus on alleviating pain by acting on the peripheral or central nervous system. Understanding their mechanisms is crucial for effective treatment, as misclassification can lead to inappropriate use and potential side effects.
Consider the example of cyclobenzaprine (a muscle relaxant) and acetaminophen (an analgesic). Cyclobenzaprine works by inhibiting nerve impulses in the brain that cause muscle contractions, often prescribed for acute musculoskeletal conditions like lower back pain. In contrast, acetaminophen reduces pain perception by blocking prostaglandin production in the brain and spinal cord. While both may be used in similar scenarios, their actions are fundamentally different. For instance, a patient with muscle spasms might receive 10 mg of cyclobenzaprine thrice daily, whereas acetaminophen is typically dosed at 650–1000 mg every 4–6 hours for pain relief, with a maximum daily limit of 4000 mg to avoid liver toxicity.
Analyzing their classification further, muscle relaxants are often categorized into two groups: antispastics (e.g., baclofen) and antispasmodics (e.g., tizanidine). Antispastics act on the spinal cord to reduce muscle stiffness, commonly used in conditions like multiple sclerosis or spinal cord injuries. Antispasmodics, on the other hand, depress the central nervous system to relieve muscle spasms, often prescribed for acute injuries. Analgesics are classified into non-opioids (e.g., ibuprofen), opioids (e.g., morphine), and adjuvant analgesics (e.g., antidepressants). Each class has specific indications, dosages, and risks, emphasizing the need for precise differentiation.
From a practical standpoint, patients and healthcare providers must recognize that muscle relaxants are not analgesics, despite their occasional concurrent use. For instance, combining tizanidine (4–8 mg every 6–8 hours) with ibuprofen (400–800 mg every 6–8 hours) can effectively manage both muscle spasms and pain in a patient with a strained neck. However, relying solely on a muscle relaxant for pain relief or an analgesic for muscle spasms can lead to suboptimal outcomes. Age-specific considerations are also vital; muscle relaxants like cyclobenzaprine are generally avoided in elderly patients due to increased risk of sedation and falls, while analgesics like NSAIDs require dose adjustments in renal impairment.
In conclusion, differentiating muscle relaxants and analgesics based on their mechanisms and uses is essential for safe and effective treatment. While muscle relaxants target muscle spasms through central or neuromuscular action, analgesics address pain perception via peripheral or central pathways. Practical application requires understanding their classifications, dosages, and contraindications to ensure optimal patient outcomes. Always consult a healthcare provider for tailored advice, as individual responses to these medications can vary significantly.
Top Muscle Relaxer Creams for Quick Pain Relief and Relaxation
You may want to see also
Explore related products






![]()
Mechanism of Action: How muscle relaxants and analgesics work in the body to relieve pain
Muscle relaxants and analgesics, though often used interchangeably in pain management, operate through distinct mechanisms to alleviate discomfort. Muscle relaxants primarily target the central nervous system (CNS) or neuromuscular junction to reduce muscle spasms and tension. For instance, baclofen, a common muscle relaxant, acts as a GABA-B receptor agonist, inhibiting neuronal activity in the spinal cord and decreasing muscle tone. In contrast, analgesics, such as acetaminophen or NSAIDs, work by blocking pain signals at the peripheral or central level. NSAIDs, for example, inhibit cyclooxygenase (COX) enzymes, reducing prostaglandin production and subsequently diminishing inflammation and pain perception.
Consider the scenario of a patient with acute lower back pain due to muscle spasms. A physician might prescribe cyclobenzaprine, a muscle relaxant that acts on the CNS to disrupt nerve impulses causing muscle contractions. The typical dosage is 5–10 mg three times daily, with caution advised for elderly patients due to increased risk of drowsiness and dizziness. Simultaneously, an analgesic like ibuprofen (400–800 mg every 6–8 hours) could be recommended to address the inflammatory component of pain. This combination targets both the source of muscle tension and the pain signal transmission, providing comprehensive relief.
From a comparative perspective, the mechanisms of muscle relaxants and analgesics highlight their complementary roles in pain management. While muscle relaxants address the root cause of pain by reducing muscle spasms, analgesics focus on symptom relief by modulating pain perception. For chronic conditions like fibromyalgia, where muscle stiffness and widespread pain coexist, a dual approach is often necessary. Tizanidine, a muscle relaxant with alpha-2 adrenergic agonist properties, can be paired with tramadol, an opioid analgesic, to manage both muscle tension and neuropathic pain. However, such combinations require careful monitoring due to potential side effects like sedation and respiratory depression.
A practical takeaway for patients and practitioners is the importance of tailoring treatment to the underlying cause of pain. For instance, in cases of musculoskeletal injury, a muscle relaxant like methocarbamol (1,500 mg 4 times daily) may be sufficient to relieve spasms, while an analgesic like naproxen (500 mg twice daily) could address inflammation. Conversely, for pain primarily driven by nerve compression, a muscle relaxant might offer limited benefit, and a targeted analgesic like pregabalin could be more effective. Understanding these mechanisms ensures that treatment is both precise and effective, minimizing reliance on broad-spectrum medications.
Finally, it’s crucial to acknowledge the limitations and risks associated with these mechanisms. Prolonged use of muscle relaxants can lead to tolerance, dependence, or impaired motor function, particularly in older adults. Analgesics, especially NSAIDs, carry risks of gastrointestinal bleeding or renal impairment, particularly at high doses or with long-term use. Patients should be educated on proper dosing, potential interactions, and the importance of reporting side effects promptly. By leveraging the unique mechanisms of muscle relaxants and analgesics while remaining vigilant about their risks, healthcare providers can optimize pain management strategies for diverse patient populations.
Why Muscles Twitch When Relaxing: Unraveling the Fascinating Phenomenon
You may want to see also
Explore related products






![]()
Indications and Uses: Conditions treated by muscle relaxants versus those managed by analgesics
Muscle relaxants and analgesics serve distinct purposes in managing pain and discomfort, though their roles often intersect in clinical practice. Muscle relaxants primarily target skeletal muscle spasms, stiffness, and associated pain, often arising from conditions like acute lower back pain, neck pain, or musculoskeletal injuries. For instance, cyclobenzaprine (Flexeril) is commonly prescribed at doses of 5–10 mg three times daily for adults, with caution advised in elderly patients due to increased risk of dizziness and falls. In contrast, analgesics—ranging from acetaminophen (Tylenol) to opioids like oxycodone—focus on alleviating pain by acting on the central nervous system or peripheral sites, regardless of its muscular origin.
Consider a patient with chronic osteoarthritis: an analgesic like ibuprofen (400–800 mg every 6–8 hours) might be prescribed to manage joint pain, while a muscle relaxant would be unnecessary unless muscle spasms develop as a secondary complication. This distinction highlights the importance of diagnosing the root cause of pain. Analgesics are broadly applicable across age groups, though dosages adjust for children and the elderly, whereas muscle relaxants are typically reserved for short-term use (2–3 weeks) due to risks of sedation and dependence.
From a persuasive standpoint, clinicians should prioritize analgesics for primary pain management unless muscle spasms are explicitly present. For example, postoperative pain is often better managed with a combination of acetaminophen and NSAIDs rather than adding a muscle relaxant, which may introduce unnecessary side effects. However, in cases like multiple sclerosis or cerebral palsy, where spasticity is a dominant symptom, muscle relaxants like baclofen (10–20 mg three times daily) become essential, often used alongside analgesics for comprehensive relief.
Comparatively, the two classes differ in mechanism and scope. Analgesics modulate pain perception directly, while muscle relaxants reduce muscle tone and spasm, indirectly alleviating pain. A descriptive example is a patient with fibromyalgia, where analgesics like duloxetine (60 mg daily) address widespread pain, but muscle relaxants like tizanidine (2–4 mg at bedtime) might be added for nocturnal muscle stiffness. This layered approach underscores the complementary, yet distinct, roles of these medications.
In practice, understanding these differences ensures targeted therapy. For acute injuries, a combination of an NSAID and a short course of a muscle relaxant like methocarbamol (500–1500 mg four times daily) can provide synergistic relief. However, long-term use of muscle relaxants should be avoided due to tolerance and cognitive impairment risks. Conversely, analgesics remain the cornerstone for chronic pain management, with opioids reserved for severe cases due to their addiction potential. Tailoring treatment to the specific condition—whether muscular spasm or nociceptive pain—maximizes efficacy while minimizing adverse effects.
Pregabalin's Muscle Relaxation Effects: Benefits, Uses, and Considerations
You may want to see also
Explore related products






![]()
Side Effects and Risks: Comparing potential adverse effects of muscle relaxants and analgesics
Muscle relaxants and analgesics, though often used interchangeably for pain management, differ significantly in their mechanisms and side effect profiles. Muscle relaxants primarily target muscle spasms by acting on the central nervous system, while analgesics focus on pain relief through various pathways. This distinction is crucial when considering their potential adverse effects, which can range from mild discomfort to severe health risks.
Analyzing Common Side Effects:
Muscle relaxants, such as cyclobenzaprine and tizanidine, frequently cause drowsiness, dizziness, and dry mouth. For instance, cyclobenzaprine can impair cognitive function, making it unsafe to operate machinery or drive, especially within the first few hours of a 10 mg dose. Analgesics, on the other hand, vary widely. Nonsteroidal anti-inflammatory drugs (NSAIDs) like ibuprofen often lead to gastrointestinal issues, including stomach ulcers, particularly when taken at high doses (e.g., 2400 mg/day). Opioid analgesics, such as oxycodone, carry risks of constipation, respiratory depression, and addiction, even at prescribed dosages (e.g., 5–10 mg every 4–6 hours).
High-Risk Populations and Interactions:
Elderly patients are particularly vulnerable to the side effects of both drug classes. Muscle relaxants can exacerbate balance issues, increasing fall risks, while analgesics like acetaminophen (up to 3000 mg/day) may strain liver function in this age group. Combining these medications amplifies dangers; for example, mixing tizanidine with opioid analgesics can cause severe sedation or hypotension. Always consult a pharmacist or physician before combining these drugs, especially in patients over 65 or those with pre-existing conditions like liver or kidney disease.
Practical Tips for Minimizing Risks:
To mitigate side effects, start with the lowest effective dose and gradually increase as needed. For muscle relaxants, take them at bedtime to reduce daytime drowsiness. With analgesics, pair NSAIDs with food to protect the stomach lining, and limit acetaminophen use to avoid liver toxicity. Patients should monitor for unusual symptoms, such as persistent headaches or difficulty breathing, and report them immediately. For chronic conditions, consider physical therapy or alternative therapies to reduce reliance on these medications.
While muscle relaxants and analgesics offer valuable pain management options, their side effects require careful consideration. Understanding their unique risks and tailoring usage to individual needs can optimize benefits while minimizing harm. Always prioritize informed decision-making and professional guidance when navigating these treatments.
Effective Techniques to Relax Tense Muscles and Ease Stress
You may want to see also
Explore related products






![]()
Combination Therapy: Exploring the use of muscle relaxants and analgesics together for pain management
Muscle relaxants and analgesics serve distinct purposes in pain management, yet their combined use is increasingly explored for synergistic effects. Muscle relaxants, such as cyclobenzaprine and tizanidine, target muscle spasms by acting on the central nervous system, while analgesics like acetaminophen or NSAIDs (e.g., ibuprofen) primarily alleviate pain by reducing inflammation or blocking pain signals. When used together, these medications can address both the nociceptive and spastic components of musculoskeletal pain, offering more comprehensive relief than either alone. For instance, a patient with acute lower back pain might benefit from 10 mg of cyclobenzaprine twice daily paired with 650 mg of acetaminophen every 6 hours, as this combination targets both muscle tension and pain perception.
The rationale for combination therapy lies in its ability to tackle multifaceted pain conditions. Muscle relaxants reduce muscle rigidity, which can exacerbate pain, while analgesics directly mitigate discomfort. However, this approach requires careful consideration of potential side effects, such as drowsiness or dizziness, which are common with muscle relaxants. For older adults or individuals with hepatic impairment, dosage adjustments are critical; for example, tizanidine doses should not exceed 4 mg in patients over 65 due to increased sensitivity. Combining these medications also necessitates monitoring for drug interactions, particularly with NSAIDs, which can elevate the risk of gastrointestinal bleeding when paired with certain muscle relaxants.
A comparative analysis of combination therapy versus monotherapy reveals its advantages in specific scenarios. A study published in *Pain Medicine* found that patients with chronic neck pain experienced greater improvement in pain scores and functional outcomes when treated with a combination of 4 mg tizanidine and 400 mg ibuprofen compared to ibuprofen alone. However, this approach is not universally superior; for mild, acute injuries, a single analgesic may suffice, avoiding unnecessary polypharmacy. Clinicians must weigh the benefits of enhanced pain relief against the risks of side effects and drug interactions, tailoring treatment to individual patient needs.
Practical implementation of combination therapy involves clear patient education and monitoring. Patients should be instructed to take muscle relaxants at bedtime to minimize daytime sedation, particularly with agents like cyclobenzaprine, which has a longer half-life. Analgesics should be dosed according to pain severity, with NSAIDs limited to short-term use to avoid renal or gastrointestinal complications. For example, a regimen of 2 mg tizanidine at night paired with 200 mg ibuprofen as needed can effectively manage moderate musculoskeletal pain. Regular follow-ups are essential to assess efficacy and adjust dosages, ensuring optimal outcomes while minimizing risks.
In conclusion, combination therapy with muscle relaxants and analgesics offers a promising approach for managing complex pain conditions, particularly when pain stems from both muscle spasms and inflammation. While this strategy can enhance relief, it demands careful planning, patient education, and monitoring to balance benefits and risks. By addressing pain from multiple angles, this approach exemplifies the evolving sophistication of pain management, providing clinicians with a powerful tool to improve patient outcomes.
Effective Techniques to Relieve Tight Foot Muscles and Promote Relaxation
You may want to see also
Frequently asked questions
No, muscle relaxants and analgesics are different types of medications. Muscle relaxants work by reducing muscle spasms and tension, while analgesics (pain relievers) target pain signals in the body.
Muscle relaxants are not primarily designed to relieve pain. While they may indirectly reduce pain by easing muscle spasms, they are not classified as analgesics and should not be used as a substitute for pain medication.
Some muscle relaxants may have mild analgesic effects due to their ability to reduce muscle-related pain, but they do not function as traditional analgesics. Their primary action is to relax muscles, not to directly alleviate pain.