Acute intermittent porphyria (AIP) is a rare genetic disorder affecting the body's ability to produce heme, leading to potentially severe neurological symptoms during acute attacks. When managing these symptoms, muscle relaxants are sometimes considered to alleviate muscle pain and stiffness. However, the use of muscle relaxants in AIP patients is a topic of concern due to the risk of triggering or exacerbating porphyria attacks. Certain muscle relaxants, particularly those metabolized by the liver, can induce the activity of hepatic enzymes involved in heme synthesis, potentially worsening the condition. Therefore, careful consideration and consultation with a specialist are essential before administering muscle relaxants to individuals with AIP, as the benefits must be weighed against the potential risks of disease exacerbation.
| Characteristics | Values |
|---|---|
| Condition | Acute Intermittent Porphyria (AIP) |
| Muscle Relaxants Risk | Generally contraindicated due to potential to trigger acute attacks |
| Mechanism of Risk | Some muscle relaxants can induce hepatic cytochrome P450 enzymes, increasing porphyrin precursor production |
| Specific Muscle Relaxants to Avoid | Succinylcholine, Suxamethonium, Vecuronium, Pancuronium, Atracurium (use with extreme caution) |
| Safer Alternatives | Benzodiazepines (e.g., Diazepam, Lorazepam) in low doses, Gabapentin, Pregabalin (though still use cautiously) |
| Symptoms of Acute Attack | Abdominal pain, nausea, vomiting, neuropathy, seizures, hypertension, tachycardia |
| Management of Acute Attacks | Avoid triggering medications, administer glucose, hematin, or heme arginate, supportive care |
| Precautionary Measures | Consult porphyria specialists, monitor closely if muscle relaxants are absolutely necessary |
| Latest Research (as of 2023) | Limited data; case reports suggest increased risk, but individual responses may vary |
| Recommendation | Avoid muscle relaxants unless absolutely necessary and under expert supervision |
Explore related products






What You'll Learn
![]()
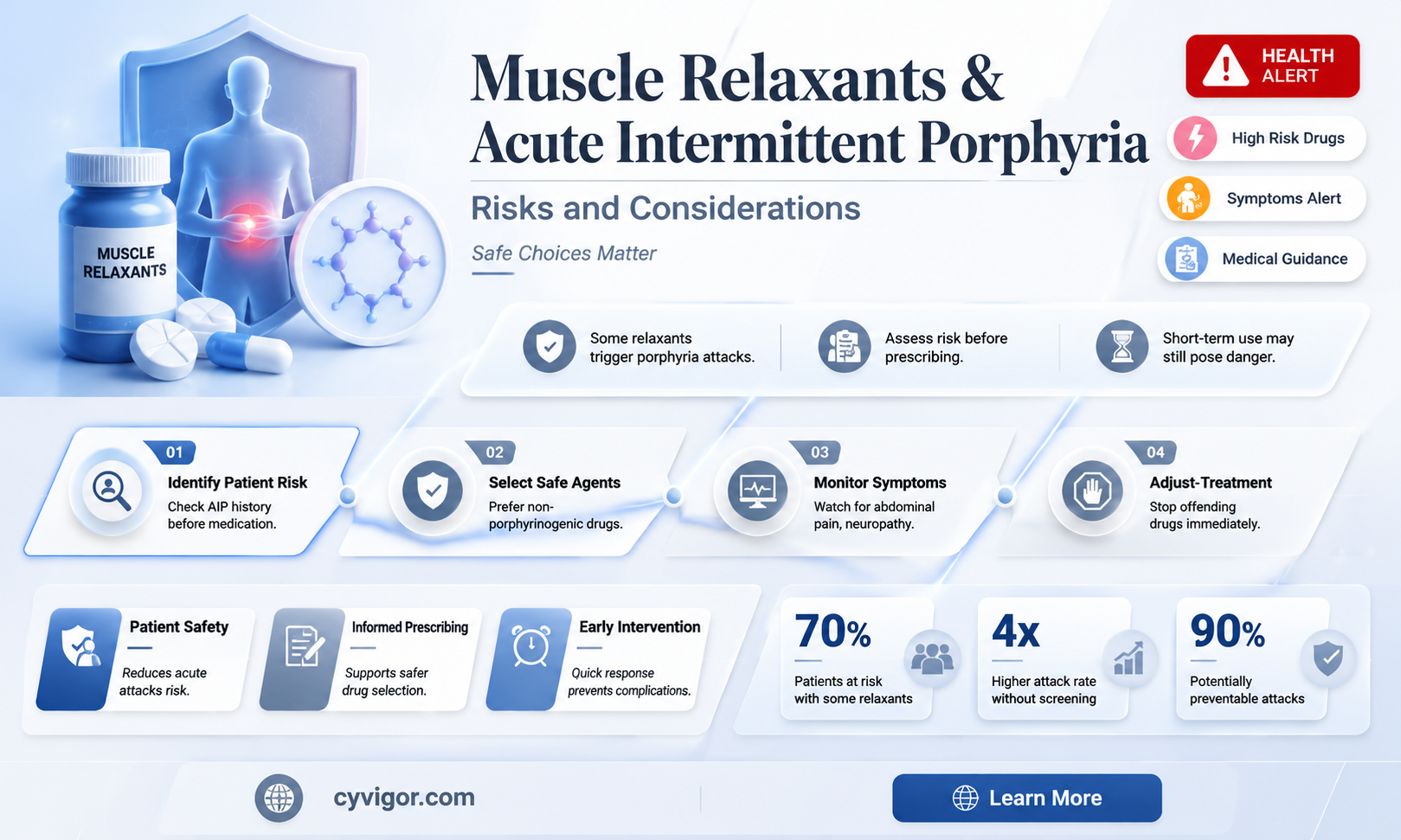
Potential Trigger for Attacks
Muscle relaxants, particularly those in the benzodiazepine and barbiturate classes, can act as potential triggers for acute intermittent porphyria (AIP) attacks. These medications are known to induce the activity of hepatic delta-aminolevulinic acid synthase (ALAS1), the rate-limiting enzyme in heme synthesis. This induction leads to the overproduction of porphyrin precursors, which accumulate and precipitate an AIP crisis. For instance, diazepam, a commonly prescribed benzodiazepine, has been documented to exacerbate symptoms in AIP patients, even at standard therapeutic doses (5–10 mg). Clinicians must exercise caution when prescribing these agents to individuals with AIP or those at risk, opting for alternative therapies whenever possible.
A comparative analysis of muscle relaxants reveals that non-benzodiazepine, non-barbiturate options may pose a lower risk for AIP patients. For example, tizanidine, a central alpha-2 agonist, and cyclobenzaprine, a tricyclic antidepressant derivative, have not been directly linked to porphyria attacks in clinical literature. However, their safety profiles are not definitively established, and individual variability in patient response necessitates careful monitoring. Dosage adjustments, such as starting tizanidine at 2 mg every 6–8 hours and titrating slowly, can minimize potential risks. Patients should be educated to report early symptoms of an AIP attack, such as abdominal pain or neurological changes, promptly.
From a persuasive standpoint, the avoidance of muscle relaxants in AIP patients is not merely precautionary but essential. The consequences of triggering an AIP attack can be severe, including acute neurological dysfunction, respiratory compromise, and even death. Given the availability of alternative pain management and muscle spasm treatments—such as physical therapy, lidocaine patches, or acetaminophen—the risk-benefit ratio of muscle relaxants in this population is unfavorable. Healthcare providers should prioritize patient history screening for porphyria and consult porphyria specialists when in doubt, ensuring that treatment decisions are evidence-based and individualized.
Descriptively, an AIP attack triggered by muscle relaxants unfolds rapidly, often within hours to days of medication initiation. Patients may experience acute abdominal pain, nausea, and vomiting, followed by neurological symptoms like muscle weakness, seizures, or peripheral neuropathy. Laboratory findings typically show elevated urine porphobilinogen (PBG) levels, confirming the diagnosis. Immediate management involves discontinuing the offending medication, administering intravenous glucose to suppress ALAS1 activity, and providing symptomatic care. This scenario underscores the critical need for awareness among prescribers and patients alike, as early recognition and intervention can prevent life-threatening complications.
Discover Effective Natural Muscle Relaxants for Pain Relief and Relaxation
You may want to see also
Explore related products





![]()
Drug Interactions and Risks
Muscle relaxants, while effective for managing muscle spasms and pain, pose significant risks for individuals with acute intermittent porphyria (AIP). AIP is a rare genetic disorder affecting heme production, and certain medications can trigger acute attacks characterized by severe abdominal pain, neurological symptoms, and potential organ damage. The interaction between muscle relaxants and AIP lies in their potential to induce cytochrome P450 enzyme activity, which can exacerbate porphyrin accumulation and precipitate an acute porphyria crisis.
Consider the case of baclofen, a commonly prescribed muscle relaxant. While it acts centrally to reduce muscle tone, its metabolism involves hepatic enzymes that may interfere with heme synthesis pathways. For AIP patients, even standard doses (10–80 mg/day) could theoretically increase the risk of an acute attack. Similarly, tizanidine, another muscle relaxant, carries a black box warning for hepatotoxicity, a concern for AIP patients already at risk of liver dysfunction during acute episodes. These examples underscore the need for cautious prescribing and individualized risk assessment.
When evaluating muscle relaxants for AIP patients, clinicians must prioritize alternatives with minimal hepatic metabolism and enzyme induction. For instance, cyclobenzaprine, often used for short-term muscle spasms, has a lower risk profile compared to baclofen or tizanidine. However, its dosage should be carefully titrated (starting at 5 mg/day) and monitored for signs of porphyria exacerbation. Non-pharmacological interventions, such as physical therapy or heat therapy, should be explored as first-line options to minimize drug-related risks.
Patients with AIP must actively participate in their care by disclosing their diagnosis to all healthcare providers and pharmacists. Carrying a medical alert card or wearing a bracelet can prevent accidental exposure to harmful medications. Additionally, maintaining a low-dose approach and avoiding polypharmacy are critical strategies to reduce cumulative risks. For acute muscle symptoms, short-acting agents with rapid elimination profiles may be preferable, but only under strict medical supervision.
In conclusion, the interplay between muscle relaxants and AIP demands a meticulous, patient-centered approach. While not all muscle relaxants are contraindicated, their use requires careful selection, dosing, and monitoring. By balancing therapeutic benefits against potential risks, clinicians and patients can navigate this complex landscape to ensure safe and effective management of muscle-related symptoms in AIP.
Relax Your Neck Muscles: Tips for a Comfortable Sleep
You may want to see also
Explore related products




![]()
Alternative Pain Management Options
Muscle relaxants, while effective for many, pose significant risks for individuals with acute intermittent porphyria (AIP). These medications can exacerbate symptoms, including abdominal pain, neurological issues, and even trigger acute attacks. Given this, exploring alternative pain management options becomes essential for AIP patients seeking relief without compromising their health.
Physical Therapy and Exercise: A Foundation for Relief
Regular, low-impact exercise tailored to individual tolerance can reduce muscle tension and improve overall function. Physical therapy, particularly modalities like gentle stretching, heat therapy, and guided strengthening exercises, helps alleviate pain by enhancing flexibility and circulation. For AIP patients, starting with 10–15 minutes of daily activity, such as walking or yoga, and gradually increasing intensity under professional guidance, can yield significant benefits. Avoid overexertion, as it may trigger symptoms.
Pharmacological Alternatives: Safer Medication Choices
Certain medications are less likely to provoke AIP attacks. For instance, acetaminophen (up to 4 grams daily for adults) is generally considered safer than NSAIDs or opioids for pain management. Low-dose tricyclic antidepressants, such as amitriptyline (10–25 mg at bedtime), can also help by modulating pain perception without the risks associated with muscle relaxants. Always consult a healthcare provider to ensure compatibility with AIP and other medications.
Mind-Body Techniques: Harnessing the Power of the Mind
Techniques like mindfulness meditation, biofeedback, and cognitive-behavioral therapy (CBT) offer non-pharmacological ways to manage pain. For example, practicing deep breathing exercises for 5–10 minutes daily can reduce stress and muscle tension. CBT, delivered in 8–12 sessions, teaches patients to reframe pain perceptions and develop coping strategies. These methods empower individuals to take control of their pain without relying on potentially harmful medications.
Lifestyle Adjustments: Small Changes, Big Impact
Dietary modifications, such as avoiding alcohol and fasting, are crucial for AIP management. Incorporating magnesium-rich foods (e.g., spinach, almonds) or supplements (300–400 mg daily, under medical supervision) can help reduce muscle cramps. Adequate sleep (7–9 hours nightly) and stress management through hobbies or social support further contribute to pain reduction. These holistic approaches address underlying triggers while promoting overall well-being.
In conclusion, while muscle relaxants are ill-suited for AIP patients, a multifaceted approach combining physical therapy, safer medications, mind-body techniques, and lifestyle adjustments offers effective pain management. Tailoring these strategies to individual needs ensures relief without exacerbating porphyria symptoms. Always collaborate with healthcare professionals to create a personalized plan.
Effective Techniques to Relieve Tight Hamstring Muscles and Improve Flexibility
You may want to see also
![]()
Symptom Exacerbation Concerns
Muscle relaxants, while beneficial for managing muscle spasms and pain, pose significant risks for individuals with acute intermittent porphyria (AIP). The primary concern lies in their potential to exacerbate symptoms of this rare metabolic disorder. AIP is characterized by the deficient activity of porphobilinogen deaminase, an enzyme crucial for heme synthesis. Certain medications, including muscle relaxants, can trigger the accumulation of porphyrin precursors, leading to acute attacks marked by severe abdominal pain, neurological symptoms, and psychiatric disturbances.
Analyzing the mechanism, muscle relaxants often belong to classes such as benzodiazepines or antispasmodics, which can induce cytochrome P450 enzyme activity in the liver. This increased metabolic demand may disrupt heme synthesis, particularly in AIP patients whose enzyme function is already compromised. For instance, tizanidine, a commonly prescribed muscle relaxant, has been associated with cases of porphyria exacerbation due to its hepatic metabolism. Similarly, baclofen, while less hepatically metabolized, can still pose risks in high doses or prolonged use, especially in individuals with pre-existing liver dysfunction, a common comorbidity in AIP.
To mitigate risks, healthcare providers must exercise caution when prescribing muscle relaxants to AIP patients. Dosage adjustments are critical; for example, starting tizanidine at 2 mg every 6–8 hours and titrating slowly can minimize metabolic stress. Alternatively, non-pharmacological interventions, such as physical therapy or heat therapy, should be prioritized. If pharmacotherapy is unavoidable, medications with minimal hepatic metabolism, like cyclobenzaprine (used cautiously at 5–10 mg/day), may be considered. However, even these options require vigilant monitoring for early signs of porphyria exacerbation, such as dark urine or sudden abdominal pain.
Comparatively, the risks of muscle relaxants in AIP patients outweigh their benefits in many cases. While these drugs provide short-term relief, their potential to trigger acute attacks—which may require hospitalization and intravenous hemin therapy—cannot be overlooked. A persuasive argument emerges for adopting a conservative approach, emphasizing lifestyle modifications and alternative therapies. Patients should be educated on avoiding triggers, such as fasting or excessive alcohol consumption, which compound the risks associated with muscle relaxants. Ultimately, the decision to prescribe these medications must be individualized, balancing symptom management with the avoidance of symptom exacerbation.
In practical terms, AIP patients experiencing muscle spasms should maintain a symptom diary to track medication use and potential triggers. Regular follow-ups with a porphyria specialist are essential to monitor disease activity and adjust treatment plans accordingly. For acute muscle issues, non-drug strategies like gentle stretching or transcutaneous electrical nerve stimulation (TENS) can offer relief without metabolic risks. When muscle relaxants are deemed necessary, patients should be advised to report any new symptoms immediately, as early intervention can prevent severe complications. This proactive, patient-centered approach ensures safer management of both AIP and its associated symptoms.
Opioids and Muscle Relaxation: Unraveling the Effects and Risks
You may want to see also
![]()
Safe Medication Alternatives for AIP
Muscle relaxants, particularly those in the benzodiazepine and barbiturate classes, are known to exacerbate acute intermittent porphyria (AIP) by inducing hepatic cytochrome P450 enzymes, which increase porphyrin precursor production. For AIP patients experiencing muscle pain or spasticity, safer alternatives are critical to avoid triggering acute attacks. Non-pharmacological interventions, such as physical therapy, heat application, and gentle stretching, should be the first line of defense. When medication is necessary, gabapentin or pregabalin can be considered, as they are not metabolized through the cytochrome P450 pathway and have a lower risk of inducing porphyria symptoms. Always consult a porphyria specialist to tailor treatment to individual needs.
For acute pain management in AIP, acetaminophen (paracetamol) is generally safe at standard doses (up to 4 grams per day for adults), but nonsteroidal anti-inflammatory drugs (NSAIDs) like ibuprofen or naproxen should be avoided due to their potential to worsen renal function, a common complication in AIP. Opioids, while effective for severe pain, must be used cautiously and at the lowest effective dose, as they can cause constipation, which may increase abdominal pressure and exacerbate symptoms. A balanced approach, combining medication with hydration and dietary adjustments (e.g., high-carbohydrate intake), can help manage pain without triggering an AIP crisis.
In cases of muscle spasticity, botulinum toxin injections offer a localized, non-systemic alternative to oral muscle relaxants. This treatment directly targets affected muscles, bypassing hepatic metabolism and reducing the risk of systemic porphyria activation. Dosage varies by muscle group and severity, typically ranging from 50 to 200 units per injection site, administered by a trained neurologist or physiatrist. Patients should monitor for injection site reactions and report any unusual symptoms promptly.
Finally, preventive strategies play a pivotal role in reducing the need for acute medications. Regular carbohydrate intake, stress management, and avoiding known triggers (e.g., alcohol, hormonal contraceptives) can minimize the frequency and severity of AIP attacks. For those with recurrent symptoms, hematin or heme arginate infusions may be prescribed to rapidly control acute episodes, though these require close medical supervision due to potential side effects like thrombophlebitis. By prioritizing safe alternatives and proactive management, AIP patients can maintain better symptom control while minimizing risks.
Muscle Relaxers and Drowsiness: Understanding Side Effects and Safety
You may want to see also
Frequently asked questions
Many muscle relaxants, especially those metabolized by the liver, can trigger acute attacks in AIP patients. It’s crucial to consult a healthcare provider for safer alternatives.
Muscle relaxants like succinylcholine, baclofen, and certain benzodiazepines (e.g., diazepam) may exacerbate AIP symptoms and should be avoided unless absolutely necessary.
Yes, some muscle relaxants can induce porphyria attacks by increasing porphyrin production or stressing the liver, leading to symptoms like abdominal pain, neuropathy, or seizures.
Some muscle relaxants, such as dantrolene or tizanidine, may be safer, but their use should still be carefully monitored by a physician familiar with porphyria.
AIP patients should inform their doctor about their condition, avoid known triggers, and opt for non-pharmacological treatments (e.g., physical therapy) whenever possible. Regular monitoring is essential.