Muscle relaxers and antidepressants are two distinct classes of medications often prescribed for different medical conditions, yet there is growing interest in their potential overlap in treating both physical and mental health symptoms. Muscle relaxers, such as cyclobenzaprine and tizanidine, are primarily used to alleviate muscle spasms and pain, while antidepressants, including SSRIs and SNRIs, target mood disorders like depression and anxiety. However, some muscle relaxers, particularly those with central nervous system effects, may also influence mood and have been explored as adjunctive treatments for depression or anxiety. Conversely, certain antidepressants can inadvertently relax muscles due to their sedative properties. This intersection raises questions about whether muscle relaxers can function as antidepressants or vice versa, prompting further research into their mechanisms, efficacy, and potential dual roles in managing both physical discomfort and mental health challenges.
| Characteristics | Values |
|---|---|
| Primary Purpose | Muscle relaxers are primarily used to alleviate muscle spasms and pain. |
| Antidepressant Properties | Some muscle relaxers (e.g., cyclobenzaprine, tizanidine) have mild serotonergic effects but are not classified as antidepressants. |
| Mechanism of Action | Muscle relaxers act on the central nervous system to reduce muscle tension, while antidepressants target neurotransmitters like serotonin, norepinephrine, or dopamine. |
| Medical Use | Muscle relaxers are prescribed for musculoskeletal conditions, whereas antidepressants are used to treat depression, anxiety, and other mood disorders. |
| Side Effects | Muscle relaxers may cause drowsiness, dizziness, and dry mouth. Antidepressants can cause nausea, weight gain, and sexual dysfunction. |
| Addiction Potential | Some muscle relaxers (e.g., carisoprodol) have abuse potential, while antidepressants generally do not. |
| Examples | Muscle relaxers: Cyclobenzaprine, Baclofen, Tizanidine. Antidepressants: Fluoxetine, Sertraline, Escitalopram. |
| Cross-Use | Certain muscle relaxers may be used off-label for mild anxiety or sleep issues, but they are not substitutes for antidepressants. |
| Pharmacological Class | Muscle relaxers are typically classified as centrally acting agents, while antidepressants belong to classes like SSRIs, SNRIs, or TCAs. |
| Long-Term Use | Muscle relaxers are generally recommended for short-term use, while antidepressants may be prescribed long-term for chronic conditions. |
| Interaction with Other Medications | Both can interact with other drugs, but the specific interactions differ based on their mechanisms. |
Explore related products

$8.49 $11.99





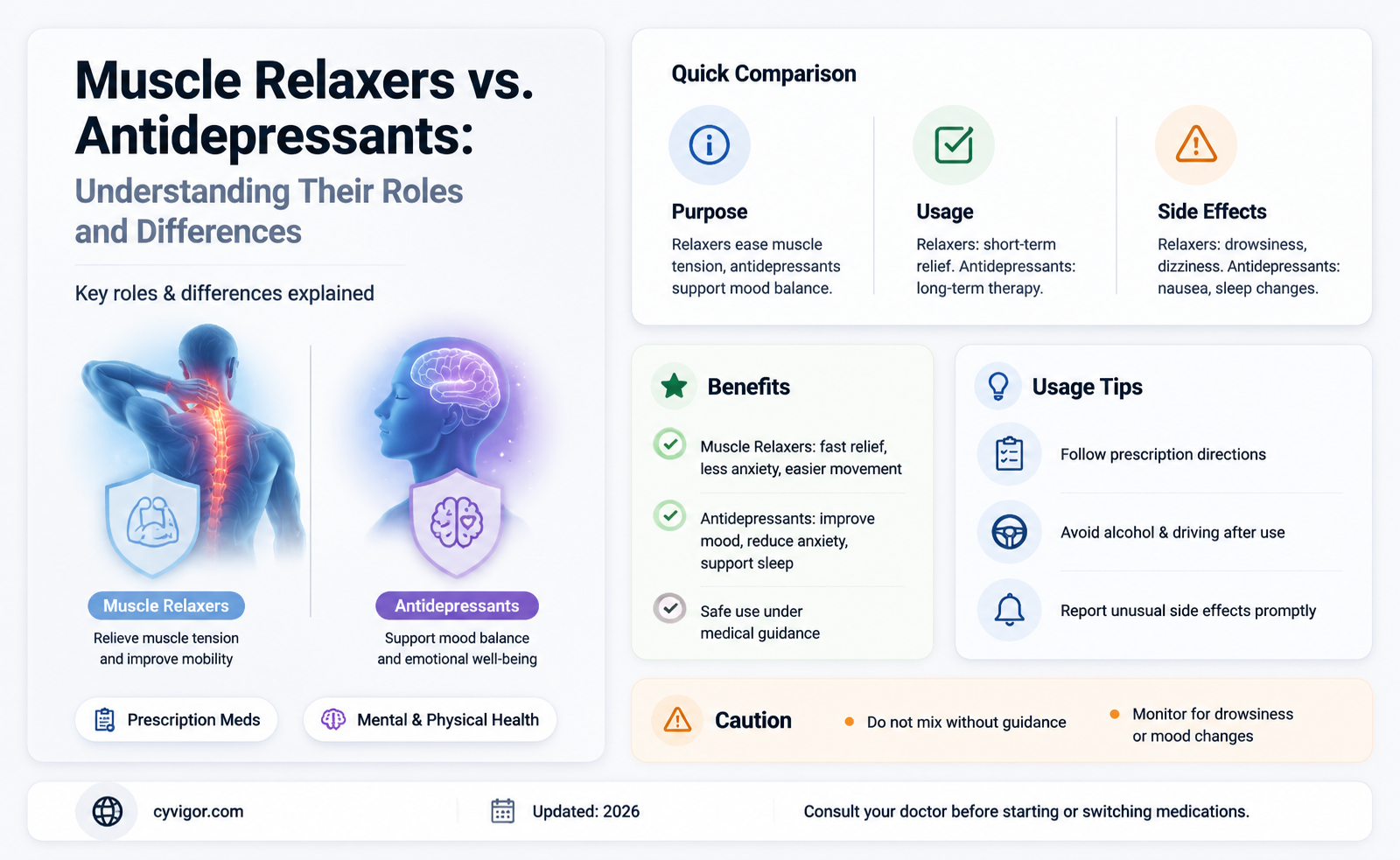
What You'll Learn
- Mechanism Differences: Muscle relaxers target muscles; antidepressants affect brain chemicals like serotonin and norepinephrine
- Off-Label Use: Some muscle relaxers may have mild antidepressant effects but aren’t primary treatments
- Side Effects: Both can cause drowsiness, dizziness, and fatigue, but differ in long-term impacts
- Treatment Goals: Muscle relaxers relieve pain/spasms; antidepressants address mood disorders and emotional symptoms
- Combination Therapy: Doctors may prescribe both for conditions like chronic pain with depression
![]()
Mechanism Differences: Muscle relaxers target muscles; antidepressants affect brain chemicals like serotonin and norepinephrine
Muscle relaxers and antidepressants, though sometimes prescribed together, operate through fundamentally different mechanisms. Muscle relaxers, such as cyclobenzaprine (Flexeril) or tizanidine (Zanaflex), primarily target skeletal muscles to alleviate spasms, stiffness, and pain. They achieve this by acting on the central nervous system to reduce muscle tone, often through GABA receptors or by inhibiting nerve impulses. In contrast, antidepressants like selective serotonin reuptake inhibitors (SSRIs) or serotonin-norepinephrine reuptake inhibitors (SNRIs) focus on altering brain chemistry. These medications increase the availability of neurotransmitters such as serotonin and norepinephrine, which regulate mood, anxiety, and emotional responses. This distinction highlights why muscle relaxers are not considered antidepressants—their actions are localized to muscles, not brain chemistry.
Consider the practical implications of these differences. For instance, a patient with chronic back pain and comorbid depression might be prescribed both a muscle relaxer and an antidepressant. The muscle relaxer, typically taken at a dose of 5–10 mg up to three times daily for cyclobenzaprine, addresses the physical symptoms of muscle tension. Meanwhile, an SSRI like fluoxetine (Prozac), starting at 20 mg daily and adjusted up to 80 mg, targets the underlying mood disorder. While both medications may improve quality of life, their effects are complementary rather than interchangeable. Misusing a muscle relaxer as an antidepressant would be ineffective, as it lacks the ability to modulate serotonin or norepinephrine levels.
From a persuasive standpoint, understanding these mechanisms underscores the importance of precise prescribing. Patients and providers alike must recognize that muscle relaxers are not a substitute for antidepressants, nor vice versa. For example, tizanidine’s short half-life (2–4 hours) and potential for sedation make it unsuitable for long-term mood management, while SSRIs’ delayed onset of action (2–4 weeks) renders them impractical for acute muscle spasms. This clarity prevents misuse and ensures that treatments are tailored to the root cause of symptoms, whether musculoskeletal or neurochemical.
A comparative analysis further illustrates the divergence. Muscle relaxers often carry risks such as drowsiness, dizziness, and impaired coordination, necessitating caution in older adults or those with hepatic impairment. Antidepressants, on the other hand, may cause side effects like nausea, weight changes, or sexual dysfunction, with SNRIs posing additional risks in patients with hypertension. These profiles reflect their distinct mechanisms and underscore why one cannot replace the other. For instance, while cyclobenzaprine’s anticholinergic properties might exacerbate cognitive fog in elderly patients, SSRIs’ impact on serotonin is unrelated to muscle function.
In conclusion, the mechanism differences between muscle relaxers and antidepressants are not merely academic—they have tangible implications for treatment efficacy and safety. Muscle relaxers act on muscles to relieve spasms, while antidepressants modulate brain chemicals to stabilize mood. This knowledge empowers patients and providers to make informed decisions, ensuring that each medication is used appropriately to address its intended target. By respecting these distinctions, healthcare professionals can optimize outcomes and avoid the pitfalls of misapplication.
Heat vs. Ice: Which Therapy Best Relaxes Sore Muscles?
You may want to see also
Explore related products






![]()
Off-Label Use: Some muscle relaxers may have mild antidepressant effects but aren’t primary treatments
Muscle relaxers, primarily prescribed for musculoskeletal conditions, occasionally exhibit mild antidepressant effects, though they are not classified as primary treatments for depression. This off-label use has sparked interest among clinicians and patients seeking alternative or adjunctive therapies. For instance, cyclobenzaprine, a commonly prescribed muscle relaxer, has been noted to improve mood in some patients, possibly due to its sedative properties reducing anxiety and promoting sleep. However, its efficacy in treating depression is limited and inconsistent, making it unsuitable as a standalone antidepressant.
Analyzing the mechanism, muscle relaxers like tizanidine and baclofen act on the central nervous system to alleviate muscle spasms, but their impact on neurotransmitters like serotonin and norepinephrine is minimal compared to dedicated antidepressants. Studies suggest that cyclobenzaprine, at doses of 10–30 mg/day, may offer modest mood benefits, particularly in patients with comorbid pain and depression. However, these effects are often secondary to pain relief rather than direct antidepressant action. It’s crucial to note that such use should only occur under medical supervision, as muscle relaxers carry risks like drowsiness, dizziness, and potential dependence.
From a practical standpoint, patients and providers must weigh the risks and benefits of off-label use. For example, older adults or individuals with hepatic impairment may face heightened risks due to slower drug metabolism. Combining muscle relaxers with antidepressants like SSRIs or SNRIs requires caution, as interactions can exacerbate side effects. A stepwise approach is advisable: start with the lowest effective dose, monitor for mood changes, and reassess after 4–6 weeks. If no significant improvement is observed, transitioning to evidence-based antidepressants is recommended.
Comparatively, while muscle relaxers may offer temporary relief, they lack the robust clinical data supporting traditional antidepressants like fluoxetine or sertraline. Their off-label use is more of a stopgap than a solution, particularly for moderate to severe depression. For mild cases or patients intolerant to standard antidepressants, they might serve as a supplementary option, but expectations should be managed. Always consult a healthcare provider to explore tailored treatment plans, ensuring safety and efficacy.
In conclusion, while some muscle relaxers may incidentally improve mood, they are not substitutes for primary antidepressant therapies. Their off-label use should be approached with caution, focusing on specific patient profiles and closely monitored outcomes. As research evolves, clearer guidelines may emerge, but for now, their role remains adjunctive at best.
Alcohol and Muscle Relaxation: Fact or Fiction? Unveiling the Truth
You may want to see also
Explore related products

$14.63 $21.99





![]()
Side Effects: Both can cause drowsiness, dizziness, and fatigue, but differ in long-term impacts
Muscle relaxers and antidepressants, though distinct in purpose, share a common side effect profile that includes drowsiness, dizziness, and fatigue. These symptoms often emerge within the first few hours of taking the medication, particularly with muscle relaxers like cyclobenzaprine, which can cause pronounced sedation at doses as low as 10 mg. Antidepressants, such as amitriptyline (a tricyclic antidepressant with muscle relaxant properties), may also induce these effects, especially during initial weeks of treatment or at higher doses exceeding 25 mg daily. While both drug classes can impair alertness, their mechanisms differ: muscle relaxers act directly on the central nervous system to reduce muscle spasms, whereas antidepressants modulate neurotransmitter levels over time.
The immediate risks of drowsiness and dizziness are manageable with practical adjustments. Patients prescribed muscle relaxers are often advised to take the medication at bedtime to minimize daytime impairment, particularly for short-term use (e.g., 2–3 weeks). Antidepressants, however, require a more gradual approach. Starting with a low dose (e.g., 10 mg of amitriptyline) and titrating upward under medical supervision can reduce initial side effects. For older adults (aged 65+), caution is critical, as both drug types increase fall risk due to orthostatic hypotension and cognitive fog. Pairing these medications with alcohol or benzodiazepines amplifies sedation, making it essential to avoid such combinations.
Long-term impacts diverge sharply between the two. Muscle relaxers, when used chronically, carry risks of dependence, cognitive decline, and liver toxicity, particularly with drugs like carisoprodol. Prolonged use beyond 3 weeks is generally discouraged unless medically necessary. Antidepressants, in contrast, may cause weight gain, sexual dysfunction, or emotional blunting over months to years, but these effects are often outweighed by their therapeutic benefits in managing mood disorders. Notably, abrupt discontinuation of antidepressants can lead to withdrawal symptoms, whereas muscle relaxers typically do not require tapering unless dependence has developed.
For patients navigating these medications, monitoring and communication are key. Keep a symptom journal to track side effects and their severity, noting when they occur relative to dosing. Report persistent or worsening symptoms to a healthcare provider, who may adjust the dosage or switch medications. Lifestyle modifications, such as maintaining a consistent sleep schedule and avoiding heavy machinery until tolerance develops, can mitigate short-term risks. Ultimately, while both drug classes share acute side effects, their long-term profiles demand tailored management strategies to balance efficacy and safety.
Heat Therapy: Unlocking Muscle Relaxation and Pain Relief Benefits
You may want to see also
Explore related products






![]()
Treatment Goals: Muscle relaxers relieve pain/spasms; antidepressants address mood disorders and emotional symptoms
Muscle relaxers and antidepressants serve distinct therapeutic purposes, each targeting specific physiological and psychological conditions. Muscle relaxers, such as cyclobenzaprine (Flexeril) or tizanidine (Zanaflex), are primarily prescribed to alleviate muscle pain and spasms caused by injuries, strains, or chronic conditions like fibromyalgia. These medications work by depressing the central nervous system, reducing muscle tension and promoting relaxation. For instance, a typical dose of cyclobenzaprine is 5–10 mg taken 3 times daily, with caution advised for elderly patients due to increased sensitivity to side effects like drowsiness or dizziness. In contrast, antidepressants like selective serotonin reuptake inhibitors (SSRIs) or serotonin-norepinephrine reuptake inhibitors (SNRIs) are designed to address mood disorders, including depression and anxiety. They function by altering neurotransmitter levels in the brain to stabilize mood and reduce emotional symptoms. For example, fluoxetine (Prozac) is often started at 20 mg daily, with dosage adjustments based on individual response and tolerance.
While both classes of drugs can induce sedation as a side effect, their mechanisms and treatment goals differ fundamentally. Muscle relaxers focus on physical symptoms, providing short-term relief from acute or chronic musculoskeletal issues. Antidepressants, however, target long-term emotional and psychological well-being, often requiring weeks to months of consistent use to achieve therapeutic effects. This distinction is critical for patients and healthcare providers to understand, as misusing one for the other’s purpose can lead to ineffective treatment or adverse outcomes. For example, using a muscle relaxer to treat depression would not address the underlying neurochemical imbalances, while prescribing an antidepressant for muscle spasms might delay appropriate pain management.
A comparative analysis reveals that while there is some overlap in side effects—such as fatigue or dizziness—the intended outcomes of these medications are non-interchangeable. Muscle relaxers are typically prescribed for short durations (e.g., 2–3 weeks) to avoid dependency, whereas antidepressants are often used long-term, sometimes indefinitely, to manage chronic mood disorders. Additionally, certain antidepressants, like amitriptyline, have dual applications, as they can also alleviate neuropathic pain due to their anticholinergic properties. However, this does not equate to muscle relaxers being antidepressants; rather, it highlights the complexity of pharmacological actions and the importance of precise prescribing practices.
For patients navigating these treatments, practical tips can enhance efficacy and safety. Muscle relaxers should be taken as directed, avoiding alcohol or other central nervous system depressants to minimize risks like respiratory depression. Antidepressants require patience, as their full effects may not manifest for 4–6 weeks. Combining these medications under medical supervision may be appropriate in some cases, such as when a patient experiences both chronic pain and depression, but this requires careful monitoring to balance benefits and risks. Ultimately, understanding the unique treatment goals of muscle relaxers and antidepressants empowers individuals to advocate for tailored, effective care.
Magnesium's Role in Muscle Relaxation: Unlocking Tension Relief Naturally
You may want to see also
Explore related products






![]()
Combination Therapy: Doctors may prescribe both for conditions like chronic pain with depression
Muscle relaxers and antidepressants, though distinct in their primary functions, often intersect in the treatment of complex conditions like chronic pain with comorbid depression. This combination therapy is not merely a coincidence but a strategic approach rooted in neurobiology. Both chronic pain and depression share overlapping pathways in the central nervous system, particularly involving serotonin and norepinephrine. Antidepressants like duloxetine and amitriptyline, which modulate these neurotransmitters, are frequently prescribed for chronic pain syndromes such as fibromyalgia or neuropathic pain. Simultaneously, muscle relaxers like cyclobenzaprine or tizanidine are used to alleviate muscle spasms and tension, often exacerbating pain. When used together, these medications can address both the physical and emotional dimensions of chronic pain, offering a more holistic treatment.
Consider a 45-year-old patient with chronic lower back pain and concurrent major depressive disorder. A physician might prescribe 30 mg of duloxetine daily to manage both pain and depression, alongside 4 mg of tizanidine at bedtime to reduce muscle spasms. The dosage and timing are critical: tizanidine’s sedative effects are minimized when taken at night, while duloxetine’s once-daily regimen improves adherence. This combination not only targets the nociceptive and neuropathic components of pain but also addresses the psychological burden, often improving overall quality of life. However, patients must be monitored for side effects, such as drowsiness or dizziness, which can occur when these medications interact.
The rationale for this approach lies in the shared mechanisms of action and the synergistic effects of these drugs. For instance, cyclobenzaprine, a muscle relaxer, has structural similarities to tricyclic antidepressants and can exert mild antidepressant effects at higher doses. Similarly, certain SSRIs and SNRIs have been shown to reduce pain sensitivity by modulating descending inhibitory pathways in the spinal cord. This dual action makes combination therapy particularly effective for patients whose conditions are intertwined, such as those with fibromyalgia or post-surgical pain with depressive symptoms. However, this strategy is not one-size-fits-all; individual factors like age, comorbidities, and medication tolerance must guide prescribing decisions.
Practical considerations are paramount when implementing combination therapy. Patients over 65, for example, may require lower doses due to age-related changes in metabolism and increased sensitivity to side effects. Additionally, lifestyle modifications, such as physical therapy and cognitive-behavioral therapy, should complement pharmacological treatment to maximize outcomes. Patients should be educated about potential drug interactions—for instance, the risk of serotonin syndrome when combining SSRIs with certain muscle relaxers—and advised to avoid alcohol, which can exacerbate sedation. Regular follow-ups are essential to assess efficacy and adjust dosages as needed, ensuring that the combination remains both safe and effective.
In conclusion, combination therapy with muscle relaxers and antidepressants represents a nuanced approach to treating chronic pain with depression. By leveraging the overlapping mechanisms of these medications, clinicians can address both the physical and emotional aspects of these conditions. However, success hinges on careful patient selection, precise dosing, and vigilant monitoring. When executed thoughtfully, this strategy can significantly improve outcomes, offering relief to patients burdened by the dual challenges of pain and depression.
Soothe Your Burning Eye Muscles: Quick and Effective Relaxation Tips
You may want to see also
Frequently asked questions
No, muscle relaxers and antidepressants are different types of medications with distinct purposes. Muscle relaxers are used to alleviate muscle spasms and pain, while antidepressants are primarily prescribed to treat depression and other mood disorders.
Muscle relaxers are not typically used to treat depression. While some muscle relaxers may have mild sedative effects, they do not address the underlying chemical imbalances associated with depression, which is the primary target of antidepressant medications.
Some antidepressants, particularly those in the tricyclic antidepressant (TCA) class, may have muscle relaxant properties as a secondary effect. However, this is not their primary function, and they are not typically prescribed solely for muscle relaxation.
In some cases, muscle relaxers and antidepressants may be prescribed together, but this should only be done under the supervision of a healthcare provider. Combining these medications can increase the risk of side effects, such as drowsiness and impaired coordination, and may require dosage adjustments.