Muscle relaxers and tricyclic antidepressants (TCAs) are distinct classes of medications, but there is some overlap in their mechanisms and uses. While muscle relaxers are primarily prescribed to alleviate muscle spasms and pain, tricyclic antidepressants are designed to treat depression and anxiety disorders. However, certain TCAs, such as amitriptyline and cyclobenzaprine, also possess muscle relaxant properties and are sometimes used off-label to manage musculoskeletal conditions. This dual functionality raises questions about whether muscle relaxers can be classified as tricyclic antidepressants, highlighting the complexity of pharmacological categorization and the multifaceted nature of these drugs.
| Characteristics | Values |
|---|---|
| Are muscle relaxers tricyclic antidepressants? | No, muscle relaxers and tricyclic antidepressants (TCAs) are distinct classes of drugs. However, some TCAs (e.g., amitriptyline, cyclobenzaprine) have muscle relaxant properties and are sometimes prescribed for musculoskeletal pain. |
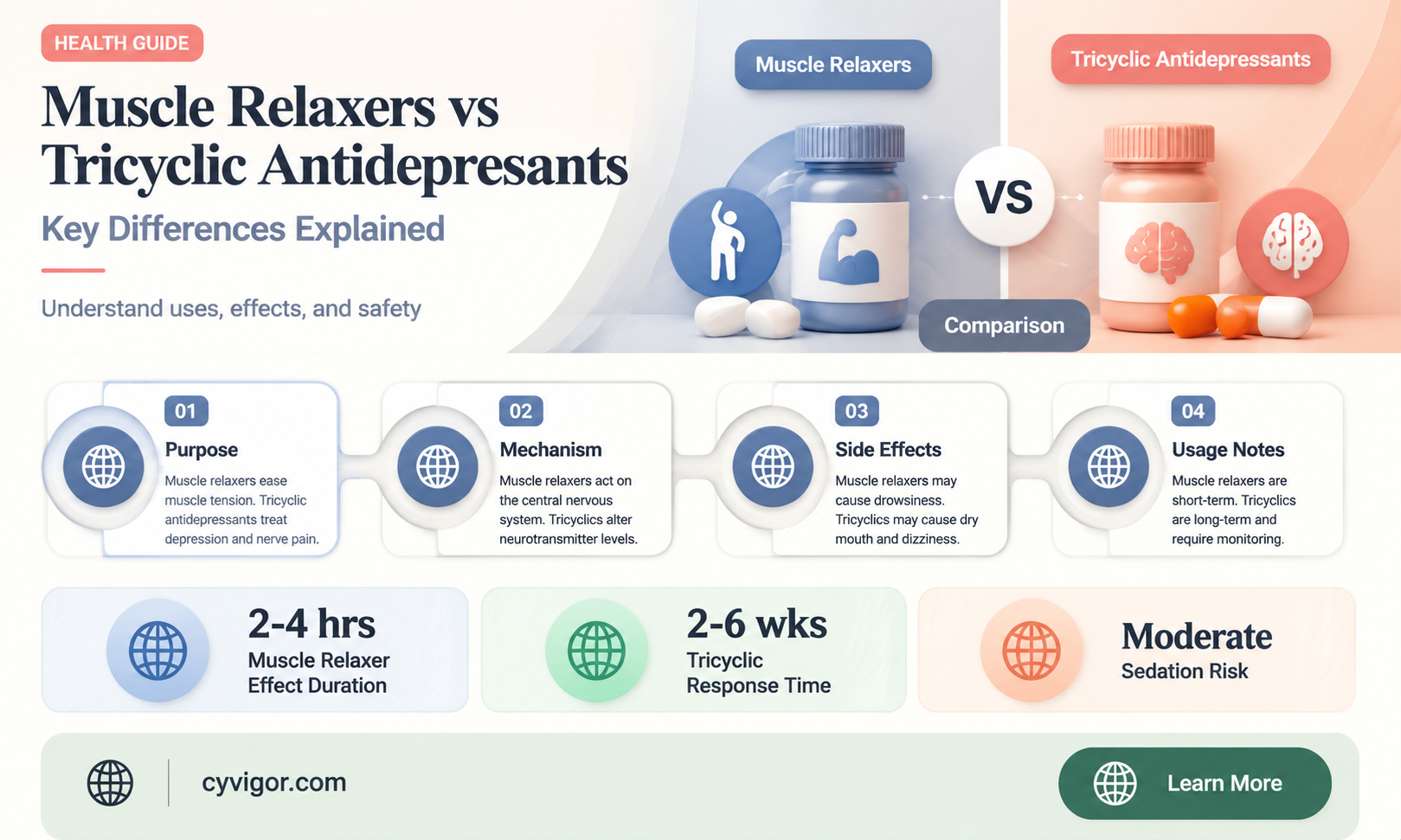
| Primary Use of Muscle Relaxers | Treat muscle spasms, pain, and stiffness (e.g., baclofen, tizanidine). |
| Primary Use of TCAs | Treat depression, anxiety, and neuropathic pain (e.g., amitriptyline, nortriptyline). |
| Mechanism of Action (Muscle Relaxers) | Act on the central nervous system or directly on muscles to reduce spasms. |
| Mechanism of Action (TCAs) | Inhibit reuptake of neurotransmitters (e.g., serotonin, norepinephrine) in the brain. |
| Side Effects (Muscle Relaxers) | Drowsiness, dizziness, weakness, dry mouth. |
| Side Effects (TCAs) | Drowsiness, dry mouth, blurred vision, weight gain, cardiac effects. |
| Examples of Muscle Relaxers | Baclofen, tizanidine, cyclobenzaprine (note: cyclobenzaprine is structurally similar to TCAs but not classified as one). |
| Examples of TCAs | Amitriptyline, nortriptyline, imipramine. |
| Overlap in Use | Some TCAs (e.g., amitriptyline) are used off-label for muscle pain due to their sedative and analgesic effects. |
| Pharmacological Classification | Muscle relaxers are not classified as antidepressants; TCAs are a subclass of antidepressants. |
Explore related products






What You'll Learn
- Mechanism of Action: How muscle relaxers and tricyclic antidepressants affect the nervous system differently
- Common Uses: Conditions treated by muscle relaxers vs. tricyclic antidepressants
- Side Effects: Comparison of side effects between the two drug classes
- Drug Interactions: Potential risks when combining muscle relaxers and tricyclic antidepressants
- Pharmacological Classification: Why muscle relaxers are not classified as tricyclic antidepressants
![]()
Mechanism of Action: How muscle relaxers and tricyclic antidepressants affect the nervous system differently
Muscle relaxers and tricyclic antidepressants (TCAs) are distinct classes of medications with overlapping uses but fundamentally different mechanisms of action within the nervous system. Muscle relaxers, such as cyclobenzaprine and tizanidine, primarily target the central nervous system (CNS) to reduce muscle spasms and pain. They achieve this by acting on the brainstem and spinal cord, inhibiting motor neuron activity and decreasing muscle tone. For instance, cyclobenzaprine mimics the effects of neurotransmitters like serotonin, while tizanidine acts as an α2-adrenergic agonist, reducing nerve signal transmission. These drugs are typically prescribed for acute musculoskeletal conditions, with dosages ranging from 5 to 30 mg daily, depending on the specific medication and patient tolerance.
In contrast, TCAs, such as amitriptyline and nortriptyline, exert their effects by modulating neurotransmitter levels in the brain. They primarily inhibit the reuptake of serotonin and norepinephrine, increasing their availability in the synaptic cleft. This mechanism is crucial for their antidepressant action but also explains their efficacy in treating chronic pain conditions, such as neuropathic pain. Unlike muscle relaxers, TCAs do not directly target muscle activity; instead, they alter pain perception by influencing the CNS’s processing of pain signals. Dosages for TCAs are often lower when used for pain management (e.g., 10–50 mg daily) compared to their antidepressant doses (75–150 mg daily), reflecting their dual therapeutic roles.
A key distinction lies in their side effect profiles, which stem from their mechanisms. Muscle relaxers commonly cause drowsiness, dizziness, and dry mouth due to their direct CNS suppression. TCAs, however, are associated with anticholinergic effects (e.g., blurred vision, constipation) and cardiovascular risks (e.g., orthostatic hypotension) due to their broader impact on neurotransmitter systems. For older adults or patients with comorbidities, these differences are critical: muscle relaxers may be preferred for short-term muscle spasm relief, while TCAs are reserved for chronic pain or depression, often requiring careful monitoring.
Practically, understanding these mechanisms helps clinicians tailor treatments. For acute back pain, a 10 mg dose of cyclobenzaprine at bedtime may suffice, while a patient with fibromyalgia might benefit from 25 mg of amitriptyline nightly. Patients should be advised to avoid alcohol and sedatives when taking either class, as both can potentiate CNS depression. Ultimately, while muscle relaxers and TCAs may appear interchangeable in certain conditions, their distinct actions on the nervous system dictate their appropriate use, highlighting the importance of mechanism-based prescribing.
Cymbalta and Muscle Relaxation: Understanding Its Effects on Tension Relief
You may want to see also
Explore related products






![]()
Common Uses: Conditions treated by muscle relaxers vs. tricyclic antidepressants
Muscle relaxers and tricyclic antidepressants (TCAs) are distinct classes of medications with overlapping yet fundamentally different therapeutic applications. Muscle relaxers, such as cyclobenzaprine and tizanidine, are primarily prescribed for acute musculoskeletal conditions like lower back pain or muscle spasms. These drugs act directly on the central nervous system to reduce muscle tension, often providing short-term relief. For instance, cyclobenzaprine is typically dosed at 5–10 mg three times daily for up to 2–3 weeks, with caution advised for elderly patients due to increased sensitivity to side effects like drowsiness and dizziness.
In contrast, TCAs, exemplified by amitriptyline and nortriptyline, are primarily used to treat depression, anxiety disorders, and neuropathic pain. Their mechanism involves increasing neurotransmitter levels in the brain, but they also have anticholinergic properties that can cause side effects like dry mouth and blurred vision. Notably, TCAs are often prescribed at lower doses for pain management than for depression. For neuropathic pain, amitriptyline may start at 10–25 mg daily, gradually increasing to 75–150 mg as tolerated, with careful monitoring for cardiovascular risks, especially in patients over 65.
While both classes can alleviate pain, their use cases diverge significantly. Muscle relaxers are typically reserved for acute, short-term conditions, whereas TCAs are employed for chronic pain syndromes and mental health disorders. For example, a patient with fibromyalgia might benefit from a TCA like nortriptyline, while someone with a strained back muscle would more likely receive a muscle relaxer like tizanidine. This distinction highlights the importance of tailoring treatment to the specific condition and patient profile.
A critical consideration is the potential for misuse or dependency. Muscle relaxers carry a risk of sedation and impaired coordination, making them unsuitable for long-term use. TCAs, while effective, require careful titration and monitoring due to their side effect profile and potential for drug interactions. For instance, combining TCAs with monoamine oxidase inhibitors (MAOIs) can lead to serotonin syndrome, a life-threatening condition. Patients should always follow their healthcare provider’s instructions and report any adverse effects promptly.
In summary, while muscle relaxers and TCAs may share some pharmacological properties, their clinical applications are distinct. Muscle relaxers address acute musculoskeletal issues with short-term use, while TCAs are versatile tools for chronic pain and mental health disorders, requiring long-term management. Understanding these differences ensures appropriate prescribing practices and better patient outcomes. Always consult a healthcare professional to determine the most suitable treatment for your specific condition.
Magnesium Sulfate's Muscle Relaxing Benefits: How It Works and Why
You may want to see also
Explore related products






![]()
Side Effects: Comparison of side effects between the two drug classes
Muscle relaxers and tricyclic antidepressants (TCAs) serve distinct purposes but share some pharmacological similarities, leading to overlapping side effects. While muscle relaxers like cyclobenzaprine and tizanidine are primarily used to alleviate muscle spasms, TCAs such as amitriptyline and nortriptyline are prescribed for depression and chronic pain. Both classes can cause drowsiness, dizziness, and dry mouth, but the severity and context of these effects differ significantly. For instance, cyclobenzaprine’s sedative properties are often intentional, aiding in pain relief by promoting rest, whereas TCAs’ drowsiness may be an unwanted side effect for patients managing depression.
Consider the cardiovascular implications, a critical area of divergence. TCAs are known to lower blood pressure and heart rate, particularly at higher doses (e.g., amitriptyline 75–150 mg/day), posing risks for elderly patients or those with pre-existing heart conditions. Muscle relaxers, while generally safer in this regard, can still cause mild hypotension, especially when combined with alcohol or other central nervous system depressants. For example, tizanidine’s dosage (2–8 mg every 6–8 hours) must be carefully titrated to avoid sudden drops in blood pressure. Patients on either medication should monitor symptoms like lightheadedness and report them promptly.
Cognitive and neurological side effects further highlight the differences. TCAs frequently cause confusion and memory impairment, particularly in older adults, due to their anticholinergic properties. This can be problematic for elderly patients already at risk for cognitive decline. Muscle relaxers, while less likely to impair memory, can induce weakness or clumsiness, increasing fall risks. A practical tip: patients on cyclobenzaprine (10–30 mg/day) should avoid activities requiring alertness until they understand how the drug affects them. Both drug classes may also exacerbate symptoms in individuals with a history of seizures, necessitating cautious prescribing.
Gastrointestinal side effects provide another point of comparison. TCAs often lead to constipation due to their anticholinergic effects, requiring patients to increase fiber intake or use stool softeners. Muscle relaxers, in contrast, are less likely to cause constipation but may induce nausea or upset stomach, particularly when taken without food. For instance, taking tizanidine with a meal can reduce gastrointestinal discomfort. Both medications can interact with other drugs metabolized by the liver, such as CYP1A2 inhibitors, increasing side effect risks—a reminder to disclose all medications to healthcare providers.
Finally, withdrawal symptoms underscore the importance of tapering these medications. Abruptly stopping TCAs can lead to flu-like symptoms, insomnia, and mood swings, necessitating a gradual reduction over weeks. Muscle relaxers, particularly tizanidine, can cause rebound hypertension and increased muscle spasms if discontinued suddenly. Patients should follow a tapering schedule (e.g., reducing tizanidine by 2–4 mg every 7 days) to minimize risks. This comparison highlights the need for individualized treatment plans, balancing therapeutic benefits against the unique side effect profiles of each drug class.
Is Percogesic a Muscle Relaxer? Understanding Its Uses and Effects
You may want to see also
Explore related products






![]()
Drug Interactions: Potential risks when combining muscle relaxers and tricyclic antidepressants
Muscle relaxers and tricyclic antidepressants (TCAs) are distinct classes of medications, but their overlapping mechanisms of action can lead to significant drug interactions when combined. Muscle relaxers, such as cyclobenzaprine and tizanidine, often act on the central nervous system to alleviate muscle spasms and pain. TCAs, like amitriptyline and nortriptyline, are primarily used to treat depression but also have analgesic properties. Both classes can enhance the effects of neurotransmitters like serotonin and norepinephrine, increasing the risk of serotonin syndrome—a potentially life-threatening condition characterized by agitation, confusion, rapid heart rate, and muscle rigidity.
Consider a scenario where a 45-year-old patient with chronic back pain is prescribed cyclobenzaprine (10 mg, three times daily) and is already taking amitriptyline (25 mg at bedtime) for depression. The combined use of these medications elevates the risk of serotonin syndrome, particularly if dosages are increased or if the patient has renal impairment, which slows drug metabolism. Additionally, both drugs can cause drowsiness and dizziness, impairing cognitive and motor functions. For instance, operating heavy machinery or driving could become hazardous, especially within the first few hours after taking either medication.
To mitigate these risks, healthcare providers should conduct a thorough medication review before prescribing muscle relaxers to patients on TCAs. If combination therapy is unavoidable, starting with the lowest effective doses of both medications is critical. For cyclobenzaprine, a reduced dose of 5 mg three times daily may be considered, while amitriptyline could be titrated down to 10 mg nightly. Patients should be monitored closely for signs of serotonin syndrome, particularly during the first week of combined therapy. Practical tips include avoiding alcohol, which can exacerbate drowsiness, and maintaining hydration to support renal function.
Comparatively, newer antidepressants like selective serotonin reuptake inhibitors (SSRIs) may pose fewer interaction risks with muscle relaxers, but they are not without their own complications. For example, combining tizanidine with fluoxetine can increase tizanidine’s blood levels, leading to severe hypotension. However, the TCA-muscle relaxer combination remains particularly concerning due to their shared pharmacological pathways. In contrast, non-pharmacological interventions, such as physical therapy or heat therapy, should be prioritized for muscle pain management in patients already on TCAs, reducing the need for additional medications.
In conclusion, while muscle relaxers and TCAs are not the same class of drugs, their interaction potential demands caution. Patients and providers must be aware of the risks, including serotonin syndrome and central nervous system depression. Tailored dosing, vigilant monitoring, and exploring alternative treatments are essential strategies to ensure safe and effective pain management in this population. Always consult a healthcare professional before combining these medications to avoid adverse outcomes.
Hot Showers for Muscle Relaxation: Fact or Fiction?
You may want to see also
Explore related products






![]()
Pharmacological Classification: Why muscle relaxers are not classified as tricyclic antidepressants
Muscle relaxers and tricyclic antidepressants (TCAs) are distinct pharmacological classes with unique mechanisms, indications, and side effect profiles. While both may be prescribed for conditions involving pain or neurological symptoms, their classification differences stem from their primary actions and chemical structures. Muscle relaxers, such as cyclobenzaprine and tizanidine, primarily target muscle spasticity or musculoskeletal pain by acting on the central nervous system to reduce nerve impulses. In contrast, TCAs like amitriptyline and nortriptyline exert their effects by inhibiting the reuptake of serotonin and norepinephrine, primarily treating depression and neuropathic pain. This fundamental difference in mechanism underscores why muscle relaxers are not classified as TCAs.
Consider the structural basis for classification. TCAs are characterized by a three-ring chemical structure, which gives them their name and influences their binding affinity to neurotransmitter transporters. Muscle relaxers lack this tricyclic structure, instead belonging to diverse chemical classes such as benzothiazepines (e.g., dantrolene) or non-benzodiazepines (e.g., metaxalone). This structural disparity is a critical factor in pharmacological classification, as it dictates how the drug interacts with biological targets. For instance, cyclobenzaprine’s chemical structure resembles that of a TCA, but its primary action as a muscle relaxer and lack of significant antidepressant efficacy at standard doses (10–30 mg/day) further distinguish it from TCAs, which are typically dosed at 25–150 mg/day for depression.
Clinically, the distinction between muscle relaxers and TCAs is reinforced by their indications and usage guidelines. Muscle relaxers are short-term treatments for acute musculoskeletal conditions, often prescribed for 2–3 weeks due to risks of tolerance and sedation. TCAs, however, are used long-term for chronic conditions like major depressive disorder or fibromyalgia. Additionally, TCAs carry a higher risk of anticholinergic side effects (e.g., dry mouth, blurred vision) and cardiovascular complications (e.g., arrhythmias), whereas muscle relaxers are more likely to cause drowsiness and dizziness. These differences in safety profiles and therapeutic windows further justify their separate classifications.
A comparative analysis highlights the overlap and divergence between these classes. While both may be used off-label for pain management—TCAs for neuropathic pain and muscle relaxers for tension headaches—their primary roles remain distinct. For example, amitriptyline’s efficacy in treating migraines does not reclassify it as a muscle relaxer, nor does cyclobenzaprine’s mild serotonergic activity make it a TCA. Pharmacological classification prioritizes a drug’s primary mechanism and intended use, ensuring clarity in prescribing practices. Misclassification could lead to inappropriate dosing or expectations, such as using a muscle relaxer as a first-line antidepressant or a TCA for acute back pain.
In practice, understanding these classifications aids clinicians in selecting the right medication for the right patient. For instance, a 45-year-old with chronic depression and comorbid fibromyalgia might benefit from a TCA like duloxetine, whereas a 30-year-old with acute lower back strain would be better served by a short course of tizanidine. Patients should also be educated on these differences to manage expectations and adhere to treatment plans. While there may be superficial similarities, the pharmacological classification of muscle relaxers and TCAs as separate entities is rooted in science, ensuring safe and effective therapeutic outcomes.
Sauna Therapy: Unwinding Muscles and Easing Tension Naturally
You may want to see also
Frequently asked questions
No, muscle relaxers and tricyclic antidepressants are different classes of medications, although some tricyclic antidepressants may have muscle relaxant properties as a secondary effect.
Yes, certain tricyclic antidepressants like amitriptyline and cyclobenzaprine are sometimes prescribed off-label to treat muscle pain and spasms due to their muscle relaxant effects, but they are primarily used to treat depression.
Muscle relaxers are primarily used to alleviate muscle spasms, pain, and stiffness, while tricyclic antidepressants are mainly prescribed to treat depression, anxiety, and other mood disorders, with muscle relaxation being a potential side benefit.































