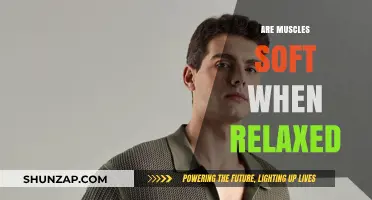
Breathing is an essential physiological process that involves the coordinated contraction and relaxation of various muscles, primarily the diaphragm and intercostal muscles. The diaphragm, a dome-shaped muscle located at the base of the lungs, plays a central role in inhalation by contracting and flattening, which increases the volume of the thoracic cavity and draws air into the lungs. During exhalation, the diaphragm relaxes and returns to its dome shape, while the intercostal muscles between the ribs may assist in forcing air out. Understanding whether these muscles are contracted or relaxed during different phases of breathing is crucial for comprehending respiratory mechanics and addressing conditions related to breathing difficulties.
| Characteristics | Values |
|---|---|
| Primary Muscles Involved | Diaphragm, External Intercostal Muscles |
| State During Inhalation | Contracted (Diaphragm moves downward, intercostals expand the chest) |
| State During Exhalation (Rest) | Relaxed (Passive return to resting position due to elastic recoil) |
| State During Forced Exhalation | Contracted (Abdominal muscles and internal intercostals assist) |
| Role of Diaphragm | Main muscle for inhalation; contracts to increase thoracic volume |
| Role of Intercostal Muscles | Assist in elevating and expanding the rib cage during inhalation |
| Energy Requirement | Inhalation is active (requires energy); resting exhalation is passive |
| Impact of Relaxation | Relaxed muscles during exhalation allow lungs to recoil naturally |
| Clinical Relevance | Weakness or fatigue in these muscles can impair breathing efficiency |
| Adaptations in Exercise | Increased use of accessory muscles (e.g., scalene, sternocleidomastoid) during heavy breathing |
Explore related products






What You'll Learn
![]()
Diaphragm Function During Inhalation
During inhalation, the diaphragm contracts and flattens, creating a vacuum in the chest cavity. This dome-shaped muscle, located at the base of the lungs, is the primary driver of breathing. As it descends, it increases the volume of the thoracic cavity, reducing air pressure inside the lungs relative to the atmosphere. This pressure gradient forces air to rush in through the airways, filling the lungs with oxygen-rich air. Without this critical action, the lungs would lack the necessary expansion to facilitate gas exchange efficiently.
Consider the mechanics of this process: the diaphragm’s contraction is not isolated but coordinated with other respiratory muscles, such as the intercostal muscles between the ribs. However, the diaphragm does the bulk of the work, accounting for about 75% of inhaled air volume during quiet breathing. This efficiency is particularly vital during rest, when the body’s oxygen demands are lower, and the diaphragm operates with minimal effort. For instance, in a healthy adult at rest, the diaphragm contracts approximately 16 to 20 times per minute, ensuring a steady supply of oxygen to tissues.
To optimize diaphragm function, certain practices can be beneficial. Deep breathing exercises, such as diaphragmatic breathing, strengthen the muscle and improve lung capacity. Lie on your back with one hand on your chest and the other on your abdomen. Inhale slowly through your nose, letting your abdomen rise while keeping your chest still. Exhale through pursed lips, engaging your abdominal muscles to push air out. Repeat this for 5–10 minutes daily to enhance diaphragm efficiency, particularly useful for individuals with respiratory conditions like COPD or asthma.
A cautionary note: prolonged shallow breathing, often seen in stressed individuals, can weaken the diaphragm over time. This reduces its ability to contract effectively, leading to decreased oxygen intake and potential fatigue. To counteract this, incorporate posture awareness into your routine. Sitting or standing upright minimizes pressure on the diaphragm, allowing it to move freely. Avoid slouching, especially during prolonged desk work, as it restricts diaphragm movement and compromises breathing efficiency.
In summary, the diaphragm’s contraction during inhalation is a cornerstone of respiratory function, ensuring adequate oxygen supply to the body. By understanding its mechanics and adopting practices that support its strength and mobility, individuals can maintain optimal breathing health. Whether through targeted exercises or mindful posture adjustments, nurturing diaphragm function is a practical step toward overall well-being.
Are All Muscle Relaxers Prescription? Exploring Over-the-Counter Options
You may want to see also
Explore related products






![]()
Intercostal Muscles Role in Breathing
The intercostal muscles, nestled between the ribs, play a pivotal role in the mechanics of breathing. These muscles are not merely passive structures but active participants in both inhalation and exhalation. During inhalation, the external intercostal muscles contract, lifting the ribs upward and outward, which expands the chest cavity and creates a vacuum that draws air into the lungs. Conversely, during quiet exhalation, these muscles relax, allowing the ribs to return to their resting position and the lungs to passively deflate. This rhythmic contraction and relaxation are essential for maintaining efficient respiratory function.
To understand the intercostal muscles’ role more deeply, consider their coordination with the diaphragm, the primary muscle of respiration. While the diaphragm descends during inhalation to increase lung volume, the external intercostal muscles simultaneously expand the rib cage, maximizing air intake. This dual action is particularly crucial during deep breathing or physical exertion when greater oxygen demand requires a more forceful inhalation. For example, athletes often focus on diaphragmatic breathing but overlook the importance of intercostal muscle engagement, which can limit their respiratory efficiency.
A practical tip for enhancing intercostal muscle function is to practice rib-expanding exercises. Lie on your back with your hands placed on your ribs, then inhale deeply while consciously expanding your rib cage outward. Exhale slowly, allowing your ribs to fall naturally. Repeat this exercise 5–10 times daily to improve intercostal muscle strength and flexibility. This technique is especially beneficial for individuals with respiratory conditions like asthma or chronic obstructive pulmonary disease (COPD), where weakened intercostal muscles can exacerbate breathing difficulties.
It’s important to note that the internal intercostal muscles, unlike their external counterparts, play a more significant role during forced exhalation, such as during coughing or singing. These muscles contract to lower the ribs and decrease chest volume, aiding in the expulsion of air. However, in normal breathing, their involvement is minimal. This distinction highlights the specialized functions of the intercostal muscles and their adaptability to different respiratory demands.
In conclusion, the intercostal muscles are indispensable for breathing, with their contraction and relaxation driving the expansion and contraction of the rib cage. By understanding their role and incorporating targeted exercises, individuals can optimize respiratory function and address specific breathing challenges. Whether for athletic performance or managing respiratory conditions, recognizing the intercostal muscles’ contribution to breathing is key to harnessing their full potential.
Does Tramadol Relax Muscles? Exploring Its Effects and Uses
You may want to see also
Explore related products






![]()
Exhalation: Passive or Active Process?
Exhalation, the process of breathing out, is often misunderstood as a purely passive event. However, the reality is more nuanced. During quiet breathing, exhalation is primarily passive, relying on the elastic recoil of the lungs and chest wall. When you inhale, the diaphragm contracts and the rib muscles expand the chest, increasing lung volume. Upon relaxation, these muscles return to their resting state, and the elastic tissues of the lungs recoil, pushing air out without active muscular effort. This passive mechanism is energy-efficient and sufficient for resting conditions.
Contrastingly, forced exhalation, such as during exercise or when blowing out candles, is an active process. Muscles like the internal intercostals and abdominal muscles contract to increase abdominal pressure, actively pushing air out of the lungs. For instance, athletes engaging in high-intensity activities use these muscles to expel air quickly, optimizing oxygen intake during the subsequent inhalation. Understanding this distinction is crucial for respiratory therapy, as patients with conditions like COPD may require training to strengthen these muscles for more effective breathing.
From a physiological standpoint, the transition from passive to active exhalation is governed by the body’s demand for oxygen and carbon dioxide clearance. During rest, the partial pressure of carbon dioxide in the blood triggers inhalation, but exhalation remains passive unless metabolic needs escalate. For children or elderly individuals with weaker respiratory muscles, even mild exertion can shift exhalation from passive to active, highlighting the adaptability of this process.
Practically, knowing whether exhalation is passive or active can guide breathing exercises. For example, pursed-lip breathing—a technique where exhalation is prolonged through a small mouth opening—leverages both passive recoil and active control to improve lung function in asthma or COPD patients. Similarly, diaphragmatic breathing emphasizes active engagement of the diaphragm during both inhalation and exhalation, enhancing lung capacity and reducing breathlessness.
In summary, exhalation is passive during rest but can become active under increased demand. Recognizing this duality allows for targeted interventions, whether through therapeutic exercises or lifestyle adjustments. By understanding the mechanics of exhalation, individuals can optimize their breathing patterns for better health and performance.
Can Panadol Ease Muscle Tension? Exploring Its Relaxation Effects
You may want to see also
Explore related products






![]()
Accessory Muscles in Forced Respiration
During forced respiration, accessory muscles spring into action, supplementing the primary muscles of inhalation and exhalation. These secondary muscles, including the scalene muscles in the neck and the pectoralis major in the chest, are typically inactive during quiet breathing but become essential during intense physical activity, emotional distress, or respiratory disorders. Their recruitment ensures that the body meets heightened oxygen demands or expels excess carbon dioxide efficiently. However, their prolonged use can signal underlying issues, such as asthma or chronic obstructive pulmonary disease (COPD), where the primary muscles alone cannot sustain adequate ventilation.
Consider the mechanics: when you sprint or lift heavy weights, your diaphragm and intercostal muscles work overtime but may still fall short. This is where accessory muscles intervene. The scalene muscles lift the upper ribs, expanding the chest cavity further, while the pectoralis major assists in elevating the chest wall. Even the sternocleidomastoid muscles in the neck can contract to aid inhalation. These muscles are not designed for continuous use, though; their activation during rest or mild activity often indicates respiratory distress. For instance, in a COPD patient, accessory muscle use during quiet breathing is a red flag, warranting immediate medical attention.
To optimize accessory muscle function during forced respiration, focus on strengthening the core and improving overall respiratory efficiency. Diaphragmatic breathing exercises, practiced for 5–10 minutes daily, can enhance primary muscle performance, reducing reliance on accessory muscles. For athletes, incorporating interval training with controlled breathing techniques can train the body to use these muscles effectively without fatigue. Caution: avoid overexertion, as excessive accessory muscle use can lead to neck and shoulder strain. If you notice persistent use of these muscles during rest, consult a healthcare provider to rule out respiratory conditions.
A comparative analysis reveals that while primary respiratory muscles are fine-tuned for endurance, accessory muscles are powerful but inefficient for prolonged use. For example, the diaphragm contracts rhythmically up to 20,000 times daily with minimal fatigue, whereas the scalene muscles, when overused, can lead to tension headaches or thoracic outlet syndrome. This highlights the importance of maintaining a balance between primary and accessory muscle engagement. Practical tip: during high-intensity workouts, exhale actively through pursed lips to engage the abdominal muscles, reducing the burden on accessory muscles.
In conclusion, accessory muscles are the unsung heroes of forced respiration, stepping in when primary muscles reach their limits. Their role is critical but temporary, and their misuse can signal health issues. By understanding their function and incorporating targeted exercises, individuals can enhance respiratory performance while safeguarding against strain. Whether you’re an athlete or someone managing a respiratory condition, recognizing when and how these muscles activate is key to maintaining optimal breathing efficiency.
Chamomile Tea's Muscle Relaxing Benefits: Fact or Fiction?
You may want to see also
Explore related products






![]()
Muscle State During Resting Breathing
During resting breathing, the diaphragm, the primary muscle of respiration, maintains a state of gentle contraction, known as tonic activity. This low-level contraction positions the diaphragm optimally for efficient inhalation without requiring maximal effort. Unlike skeletal muscles that fully relax at rest, the diaphragm’s tonic contraction ensures a baseline dome shape, allowing it to descend smoothly during inspiration. This subtle tension is essential for spontaneous breathing, as it prevents the diaphragm from collapsing into the chest cavity and obstructing airflow. Without this resting tone, the transition from exhalation to inhalation would be less fluid, requiring greater energy expenditure to initiate each breath.
Consider the mechanics of this process: at rest, the diaphragm’s tonic contraction creates a subatmospheric pressure in the pleural cavity, facilitating passive exhalation. When inhalation begins, the diaphragm contracts further, but this additional effort builds upon the existing resting tone rather than starting from a fully relaxed state. This principle is analogous to a stretched rubber band—it requires less force to extend further when already under tension. For individuals practicing diaphragmatic breathing exercises, understanding this resting tone is crucial. By consciously engaging the diaphragm from its tonically contracted state, one can enhance lung capacity and reduce the work of breathing, particularly in conditions like chronic obstructive pulmonary disease (COPD) or asthma.
Contrast this with accessory muscles of respiration, such as the scalene and sternocleidomastoid muscles, which remain relaxed during resting breathing. These muscles are recruited only during increased ventilatory demand, such as exercise or respiratory distress. Their relaxed state at rest conserves energy and prevents unnecessary tension in the neck and shoulder regions. However, in cases of diaphragmatic fatigue or dysfunction, these accessory muscles may become chronically engaged, leading to postural strain and reduced breathing efficiency. This highlights the importance of maintaining diaphragmatic health through targeted exercises, such as pursed-lip breathing or abdominal breathing techniques, to ensure optimal resting muscle states.
A practical takeaway for improving resting breathing efficiency involves mindful breathing practices. Start by lying supine with one hand on the chest and the other on the abdomen. Focus on deepening abdominal movement while keeping chest motion minimal. This engages the diaphragm from its resting tone, promoting fuller oxygen exchange. Incorporate this practice for 5–10 minutes daily, particularly before bed, to enhance relaxation and reduce nocturnal breathing disruptions. For older adults or individuals with respiratory conditions, gradual progression is key—begin with shorter sessions and increase duration as tolerance improves. By optimizing the diaphragm’s resting state, one can achieve more effortless breathing, even at rest.
Timing Muscle Relaxers Discontinuation: Pre-Surgery Guidelines for Safe Recovery
You may want to see also
Frequently asked questions
During inhalation, the primary muscle for breathing, the diaphragm, contracts and moves downward, creating more space in the chest cavity and allowing air to enter the lungs.
During exhalation, the diaphragm and other respiratory muscles relax, returning to their original position and reducing the volume of the chest cavity, which forces air out of the lungs.
During quiet breathing, the external intercostal muscles contract slightly to assist the diaphragm in expanding the rib cage during inhalation, while they relax during exhalation to allow the rib cage to return to its resting position.