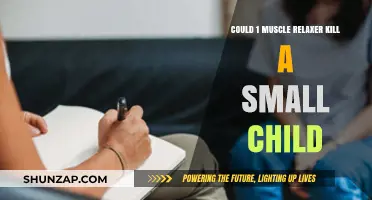
Skeletal muscle relaxants, primarily used to alleviate muscle spasms and pain, are not typically considered a standard treatment for Parkinson's disease (PD), a neurodegenerative disorder characterized by motor symptoms such as tremors, rigidity, and bradykinesia. While PD involves muscle stiffness and rigidity due to dopamine deficiency, these symptoms are distinct from the conditions skeletal muscle relaxants are designed to address, such as acute muscle spasms or spasticity. However, in some cases, patients with PD may experience secondary muscle tension or dystonia, leading clinicians to explore the use of muscle relaxants as adjunctive therapy. Despite this, their efficacy and safety in PD remain limited, and they are generally not recommended as a primary treatment, as they do not address the underlying dopaminergic deficit. Instead, PD management primarily relies on dopaminergic medications, deep brain stimulation, and physical therapy to improve motor function and quality of life.
| Characteristics | Values |
|---|---|
| Primary Use of Skeletal Muscle Relaxants | Treatment of muscle spasms, stiffness, and pain associated with conditions like sprains, strains, or back pain. |
| Use in Parkinson's Disease | Not typically a first-line treatment for Parkinson's disease (PD). |
| Relevance to PD Symptoms | May be considered in PD patients with secondary muscle rigidity or dystonia, but not for primary PD motor symptoms. |
| Commonly Used Relaxants in PD Context | Baclofen, tizanidine, or benzodiazepines (e.g., diazepam) in specific cases. |
| Effectiveness in PD | Limited; primarily used for symptom management, not disease modification. |
| Side Effects in PD Patients | Increased risk of sedation, dizziness, and worsening of PD-related balance issues. |
| Alternative Treatments for PD | Dopamine agonists, levodopa, MAO-B inhibitors, and physical therapy. |
| Medical Recommendation | Use only under specialist supervision for specific PD-related muscle issues. |
| Research Status | Limited evidence supporting widespread use in PD; more research needed. |
| Patient Considerations | Individualized approach based on symptom severity and comorbidities. |
Explore related products






What You'll Learn
![]()
Effectiveness of Muscle Relaxants in Parkinson's Disease
Skeletal muscle relaxants are occasionally considered in Parkinson's disease (PD) management, primarily to address secondary muscle rigidity and dystonia, which can exacerbate motor symptoms and reduce quality of life. While not first-line treatments, drugs like baclofen, tizanidine, and cyclobenzaprine are sometimes prescribed off-label to alleviate these complications. Their effectiveness, however, is limited and varies widely among patients, often requiring careful titration to balance benefits against side effects such as sedation and dizziness.
Baclofen, a GABA-B agonist, is one of the most studied muscle relaxants in PD. It acts on the spinal cord to reduce muscle spasticity and can be administered orally or via intrathecal pump for severe cases. Dosages typically start at 5 mg three times daily, gradually increasing to 20–80 mg/day as tolerated. While it may improve rigidity, its efficacy is often modest, and side effects like fatigue and confusion can limit its use, particularly in older adults or those with cognitive impairment.
Tizanidine, an α2-adrenergic agonist, offers another option, though its use in PD is less common. It is generally dosed at 2–4 mg every 6–8 hours, with a maximum daily dose of 36 mg. Tizanidine’s short duration of action and potential for hypotension make it less ideal for long-term management. However, it may be preferable for patients experiencing localized dystonia or those intolerant to baclofen.
Cyclobenzaprine, a centrally acting muscle relaxant, is rarely used in PD due to its strong sedative effects and limited evidence of efficacy. Its anticholinergic properties can worsen PD symptoms like cognitive decline or urinary retention, making it a less attractive option. When used, dosages are typically kept low (5–10 mg/day) to minimize risks.
In practice, the decision to use muscle relaxants in PD hinges on a careful assessment of risks versus benefits. These medications are not disease-modifying and do not address the core dopaminergic deficit of PD. Instead, they target secondary symptoms that may arise from prolonged muscle tension or abnormal postures. Physical therapy, botulinum toxin injections, and adjustments to dopaminergic therapy often provide more effective and safer alternatives. For patients where muscle relaxants are deemed necessary, close monitoring and individualized dosing are critical to optimize outcomes.
Alcohol vs. Anesthesia: Which Relaxes Smooth Muscles More Effectively?
You may want to see also
Explore related products






![]()
Commonly Used Skeletal Muscle Relaxants for Parkinson's
Skeletal muscle relaxants are not typically first-line treatments for Parkinson's disease (PD), but they can play a role in managing specific symptoms, particularly muscle rigidity and dystonia. These medications work by reducing muscle tension and spasms, which can improve mobility and comfort in PD patients. While they are not a cure for the disease, they can be a valuable adjunct therapy when other treatments fall short.
One commonly prescribed skeletal muscle relaxant for PD is baclofen. This medication acts as a GABA-B receptor agonist, inhibiting the release of excitatory neurotransmitters and reducing muscle tone. Baclofen is often used to treat generalized rigidity and can be particularly helpful for patients experiencing painful muscle spasms. The typical starting dose is 5 mg three times daily, gradually increasing to a maximum of 80 mg/day based on response and tolerance. It’s important to monitor for side effects such as drowsiness, dizziness, and weakness, especially in older adults. Baclofen should be tapered slowly when discontinuing to avoid withdrawal symptoms.
Another option is tizanidine, which acts as an alpha-2 adrenergic agonist, reducing muscle tone by suppressing spinal cord reflexes. Tizanidine is often preferred for its shorter duration of action, making it suitable for intermittent use during periods of heightened rigidity or dystonia. The usual dose ranges from 2 to 8 mg every 6 to 8 hours, with a maximum daily dose of 36 mg. Patients should avoid grapefruit juice while taking tizanidine, as it can increase blood levels and the risk of side effects like hypotension and sedation. This medication is particularly useful for younger patients or those who require flexibility in their treatment regimen.
Dantrolene is a less commonly used muscle relaxant but can be effective for severe, refractory muscle rigidity in PD. It works by directly inhibiting calcium release in muscle fibers, reducing contraction. However, its use is limited by potential hepatotoxicity, requiring regular liver function monitoring. The starting dose is typically 25 mg daily, increasing gradually to a maximum of 100 mg four times daily. Due to its side effect profile, dantrolene is reserved for cases where other treatments have failed.
When considering skeletal muscle relaxants for PD, it’s crucial to balance their benefits against potential risks. These medications can interact with dopaminergic therapies and other PD medications, so careful titration and monitoring are essential. Additionally, they are not a substitute for primary PD treatments like levodopa or deep brain stimulation but can provide symptomatic relief when rigidity or dystonia significantly impacts quality of life. Always consult a neurologist or movement disorder specialist to determine the most appropriate treatment plan.
Are Muscle Relaxers Safe? Exploring Risks, Benefits, and Alternatives
You may want to see also
Explore related products





![]()
Side Effects of Muscle Relaxants in Parkinson's Patients
Skeletal muscle relaxants, while not a primary treatment for Parkinson's disease, are sometimes prescribed to manage secondary symptoms like muscle stiffness and rigidity. However, their use in Parkinson's patients requires careful consideration due to potential side effects that can exacerbate existing challenges. One of the most common side effects is increased sedation, which can worsen the fatigue and cognitive impairment often experienced by Parkinson's patients. For instance, medications like cyclobenzaprine or tizanidine, typically prescribed at doses of 5–20 mg, can cause drowsiness, making it difficult for patients to maintain alertness during daily activities.
Another significant concern is the risk of falls. Muscle relaxants can impair coordination and balance, which are already compromised in Parkinson's patients due to motor symptoms. A study published in the *Journal of Neurology* found that patients over 65 taking muscle relaxants had a 30% higher risk of falls compared to those not on these medications. To mitigate this, caregivers should ensure a safe home environment, removing trip hazards and installing handrails, especially if a patient is prescribed higher doses of these drugs.
Drug interactions are also a critical issue. Parkinson's patients often take dopaminergic medications like levodopa, and muscle relaxants can interfere with their efficacy or increase side effects. For example, combining tizanidine with levodopa may lead to heightened dizziness or low blood pressure. Pharmacists and physicians must carefully review a patient’s medication regimen to avoid such interactions, particularly in older adults who may metabolize drugs more slowly.
Finally, long-term use of muscle relaxants in Parkinson's patients raises concerns about dependency and tolerance. Prolonged use of medications like baclofen, often prescribed at 10–80 mg daily, can lead to withdrawal symptoms if abruptly discontinued. Patients and caregivers should be educated on the importance of adhering to prescribed dosages and the need for gradual tapering under medical supervision. While muscle relaxants can provide symptomatic relief, their side effects demand a tailored, cautious approach in Parkinson's management.
Atrial Muscle's Role in Isovolumetric Relaxation: A Cardiac Connection
You may want to see also
Explore related products





![]()
Alternatives to Skeletal Muscle Relaxants for Parkinson's
Skeletal muscle relaxants are not typically the first-line treatment for Parkinson's disease (PD) due to their potential side effects, such as drowsiness and impaired motor function, which can exacerbate PD symptoms. Instead, patients and caregivers often seek alternatives that address rigidity, tremors, and muscle stiffness without compromising mobility or cognitive function. Below are targeted alternatives, structured as a practical guide for managing PD-related muscle issues.
Physical Therapy and Exercise: A Foundation for Mobility
Structured physical therapy is a cornerstone for PD patients, focusing on stretching, strength training, and balance exercises. Techniques like the LSVT BIG program, which uses amplified movements to recalibrate motor control, have shown significant improvements in rigidity and gait. For home routines, low-impact activities such as tai chi, yoga, or aquatic therapy are recommended. Aim for 30 minutes of moderate exercise daily, tailored to the patient’s fitness level. Caution: Avoid overexertion, especially in advanced stages, and consult a therapist to design a safe regimen.
Pharmacological Alternatives: Dopaminergic Agents and Beyond
While skeletal muscle relaxants are rarely used, dopaminergic medications like levodopa remain the gold standard for PD. However, adjunctive therapies such as amantadine (100–300 mg/day) can reduce dyskinesia and stiffness, particularly in early stages. For localized muscle tension, botulinum toxin injections (e.g., 50–200 units per muscle group) offer targeted relief without systemic side effects. Always monitor for interactions, especially in patients over 65, as polypharmacy risks increase with age.
Non-Invasive Neuromodulation: A Technological Edge
Transcranial magnetic stimulation (TMS) and deep brain stimulation (DBS) are emerging as alternatives for refractory motor symptoms. DBS, though invasive, provides sustained relief from rigidity and tremors in advanced cases. For milder symptoms, wearable devices like portable TENS units (transcutaneous electrical nerve stimulation) can temporarily alleviate muscle stiffness when applied at 30–50 Hz for 20–30 minutes. These methods require professional oversight but offer promising results without sedative effects.
Lifestyle and Complementary Approaches: Holistic Support
Dietary adjustments, such as increasing magnesium-rich foods (spinach, almonds) or considering supplements (400–600 mg/day magnesium glycinate), may reduce muscle cramps. Heat therapy (warm baths or heating pads) and massage can provide immediate, drug-free relief. Mindfulness practices, including meditation and guided relaxation, help manage stress-induced muscle tension. While not replacements for medical treatment, these strategies enhance overall symptom management and quality of life.
Takeaway: Personalized Care is Key
Alternatives to skeletal muscle relaxants in PD require a multifaceted approach, blending medical, physical, and lifestyle interventions. Patients should work closely with neurologists, physiotherapists, and occupational therapists to tailor a plan addressing their unique needs. Regular reassessment ensures treatments remain effective as the disease progresses, prioritizing safety and functional independence.
Does CityMD Prescribe Muscle Relaxants? Facts and Guidelines
You may want to see also
Explore related products





![]()
Research on Muscle Relaxants and Parkinson's Symptoms
Skeletal muscle relaxants, traditionally used to alleviate muscle spasms and pain, have emerged as a subject of interest in Parkinson’s disease (PD) research due to their potential to address secondary motor symptoms. While PD is primarily characterized by dopaminergic deficits, patients often experience rigidity, dystonia, and muscle stiffness that dopamine replacement therapies alone cannot fully resolve. This has prompted investigations into whether muscle relaxants, such as baclofen, tizanidine, or cyclobenzaprine, could provide symptomatic relief. However, their use in PD is not without challenges, as these medications can exacerbate fatigue, cognitive impairment, or postural instability—common concerns in this population.
One notable area of research focuses on baclofen, a GABA-B agonist, which has shown promise in reducing levodopa-induced dyskinesias and dystonia in PD patients. A 2018 study published in *Movement Disorders* demonstrated that low-dose baclofen (10–20 mg/day) improved dystonic symptoms in 60% of participants without significantly worsening bradykinesia or balance. However, higher doses were associated with sedation and confusion, particularly in patients over 65 years old. This highlights the need for individualized dosing and careful monitoring, especially in older adults or those with renal impairment, as baclofen is primarily renally excreted.
In contrast, tizanidine, an α2-adrenergic agonist, has been explored for its spasmolytic and analgesic properties in PD. A randomized controlled trial in *Neurology* (2020) found that tizanidine (2–6 mg/day) reduced muscle rigidity in PD patients, but its short half-life necessitated frequent dosing, leading to non-adherence in some cases. Additionally, tizanidine’s potential to lower blood pressure and cause liver enzyme elevations requires cautious use, particularly in patients with cardiovascular comorbidities or those on polypharmacy regimens.
Cyclobenzaprine, a centrally acting muscle relaxant, has been less studied in PD but offers a unique advantage due to its longer duration of action. A case series in *Journal of Neurology* (2019) reported that low-dose cyclobenzaprine (5 mg at bedtime) improved nocturnal muscle stiffness in PD patients without daytime sedation. However, its anticholinergic properties may worsen cognitive symptoms or urinary retention, making it less suitable for patients with dementia or prostate issues.
Despite these findings, the integration of muscle relaxants into PD management remains experimental. Clinicians must weigh the benefits of symptom relief against the risks of adverse effects, particularly in a population already vulnerable to polypharmacy complications. Future research should focus on long-term safety, optimal dosing strategies, and combination therapies to maximize efficacy while minimizing side effects. For now, muscle relaxants may serve as a valuable adjunctive option for select PD patients with refractory motor symptoms, but their use should be guided by careful patient selection and close monitoring.
Sauna Benefits: How Heat Therapy Relaxes and Soothes Muscles
You may want to see also
Frequently asked questions
Skeletal muscle relaxants are not typically used as a primary treatment for Parkinson's disease. They may be prescribed to manage secondary symptoms like muscle stiffness or pain but are not a standard therapy for the disease itself.
While skeletal muscle relaxants can alleviate muscle rigidity, they are not the first-line treatment for Parkinson's-related rigidity. Medications like levodopa or dopamine agonists are preferred for addressing rigidity caused by Parkinson's.
Yes, skeletal muscle relaxants can cause side effects such as drowsiness, dizziness, or weakness, which may worsen balance issues or mobility problems already present in Parkinson's patients. Use should be carefully monitored by a healthcare provider.
Some skeletal muscle relaxants may interact with Parkinson's medications, potentially increasing side effects like sedation or impairing motor function. Always consult a doctor before combining these treatments.
Long-term use of skeletal muscle relaxants in Parkinson's patients is generally not recommended due to the risk of side effects and dependency. They are typically used short-term or as needed for specific symptoms.