Asthma is a chronic inflammatory disease that affects the airways of the lungs. It is characterized by symptoms such as shortness of breath, coughing, and wheezing, which can cause respiratory and sleep disturbances. While asthma is a manageable condition, it can lead to fatigue and exhaustion due to uncontrolled symptoms, nocturnal asthma, and asthma flare-ups. Additionally, asthma has been associated with musculoskeletal dysfunction and chronic pain in adults, potentially impacting their quality of life. In severe cases requiring mechanical ventilation, asthma patients may experience diffuse muscle weakness due to acute myopathy and the use of certain medications, such as corticosteroids and neuromuscular blocking agents. This raises questions about the role of these treatments in muscle weakness and the need for further research to optimize endurance training programs for asthmatic individuals.
| Characteristics | Values |
|---|---|
| Asthma classification | Mild, severe, nocturnal, persistent |
| Musculoskeletal effects | Dysfunction, pain, postural alterations, muscle shortening, decreased chest wall expansion, decreased shoulder internal rotation, decreased thoracic spine flexibility |
| Fatigue causes | Uncontrolled asthma, nocturnal asthma, asthma flare-ups, asthma attacks, asthma triggers, sleep disturbance, obesity |
| Muscle weakness causes | Reduced motor neuron activity, decreased percentage of type I fibers, increased percentage of type IIb fibers, reduced activity of enzymes involved in oxidative energy conversion, respiratory failure, cardiac failure, corticosteroid therapy, neuromuscular paralysis, acute myopathy |
| Functional capacity | Impaired, diminished activity patterns, lower limb fatigue, limited endurance, limited exercise tolerance |
Explore related products






What You'll Learn
![]()
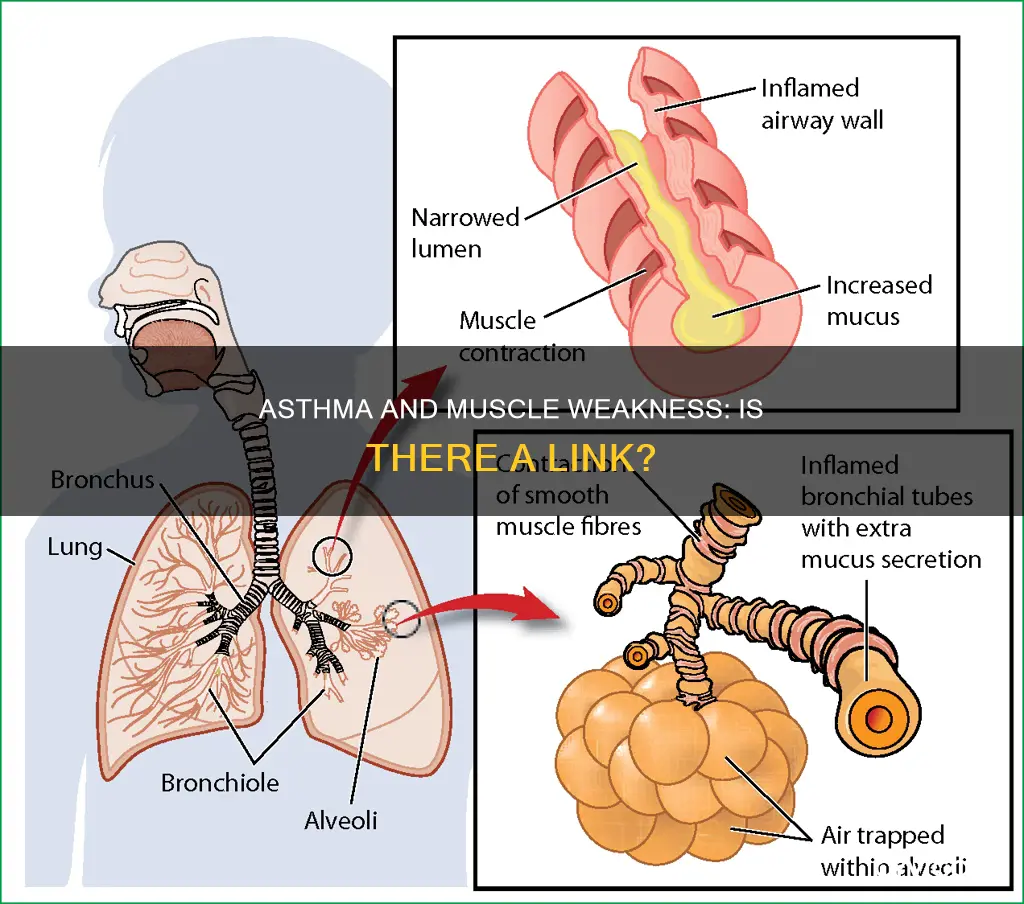
Asthma and muscle weakness: the role of mechanical ventilation
Asthma is an inflammatory disease that affects the airways of the lungs. It is a chronic condition that can be managed and controlled but not cured. Asthma can cause fatigue due to uncontrolled symptoms, nocturnal asthma, asthma flare-ups, and asthma attacks. Obesity can also exacerbate asthma symptoms, leading to chronic coughing, disrupted sleep, and increased fatigue.
Asthma patients often experience diminished activity patterns, which can lead to impaired functional capacity. While asthma itself does not directly cause muscle weakness, the use of corticosteroids as a common treatment for asthma has been associated with an increased risk of muscle weakness and even myopathy. Mechanical ventilation for severe asthma, combined with prolonged neuromuscular paralysis induced by specific drugs, further elevates the risk of developing diffuse muscle weakness.
Mechanical ventilation is a life-saving intervention for patients with severe asthma who require respiratory support. However, the immobilization and drug-induced paralysis associated with mechanical ventilation can contribute to muscle weakness. In a retrospective cohort study, researchers evaluated the incidence of muscle weakness in mechanically ventilated asthma patients treated with corticosteroids alone or in combination with neuromuscular paralysis.
The study found a significantly higher incidence of muscle weakness in patients receiving both corticosteroids and neuromuscular blocking agents compared to those receiving only corticosteroids. Additionally, the duration of paralysis was longer in the group that experienced muscle weakness. This indicates a correlation between prolonged paralysis and the development of muscle weakness.
The exact mechanisms underlying the development of muscle weakness in mechanically ventilated asthma patients are not fully understood. Further research is needed to elucidate the complex interactions between corticosteroids and neuromuscular blocking agents, and their potential synergistic effects on muscle function. Optimizing endurance training programs and physical therapy protocols can help mitigate the negative impact of muscle weakness on asthma patients' functional capacity.
Low Glucose and Muscle Weakness: What's the Link?
You may want to see also
Explore related products






![]()
Corticosteroids and muscle weakness in asthma patients
Asthma is a chronic inflammatory disease that affects the airways of the lungs. It is a condition that can be managed and controlled but not cured. Asthma patients often experience fatigue and tiredness, which may be due to several factors, including respiratory muscle weakness.
The use of corticosteroids in the treatment of asthma has been linked to muscle weakness in patients. Corticosteroids are a common treatment for asthma, and while they can help manage the condition, they also carry the risk of steroid-induced myopathy, a well-known side effect. This risk is particularly evident in patients who have been using corticosteroids for an extended period, with one source suggesting that muscle weakness can occur after at least a year of daily treatment.
Several studies have investigated the link between corticosteroid use and muscle weakness in asthma patients. One study found that 65% of patients using corticosteroids daily for a year or longer reported weakness in the legs, and 20% of these patients showed objective signs of muscle weakness. Another study compared asthma patients treated with corticosteroids alone versus those treated with corticosteroids and neuromuscular paralysis. The results indicated a much higher incidence of muscle weakness in the group that received both treatments.
The mechanism behind corticosteroid-induced muscle weakness is believed to involve metabolic processes at the skeletal muscle level, potentially leading to skeletal muscle atrophy and severe functional impairment. This impairment is characterised by tiredness, weakness, and fatigue during physical tasks. Additionally, asthma patients who choose a more sedentary lifestyle due to their condition may experience physical deconditioning, further exacerbating their symptoms and increasing the risk of obesity.
While the adverse effects of long-term corticosteroid use on respiratory muscle function remain a subject of debate, it is generally recognised that acute respiratory myopathy can be caused by therapy with high doses of systemic steroids. Furthermore, asthma patients undergoing mechanical ventilation for severe asthma are at risk of developing diffuse muscle weakness due to acute myopathy. However, the relative importance of corticosteroids and neuromuscular paralysis in causing this myopathy is still a matter of controversy.
Perineal Muscle Spasms: Urinary Problems and Solutions
You may want to see also
Explore related products





![]()
Asthma, muscle weakness, and obesity
Obesity is a major public health problem, with the World Health Organization reporting that over 650 million adults are obese. It is a risk factor for several diseases, including asthma. Obesity-induced asthma is an area of growing research interest, with studies suggesting that long-chain free fatty acids and their specific receptors FFAR1, expressed on airway smooth muscle, could be an important modulator of airway smooth muscle tone and its remodelling. Obese individuals have an increased risk of asthma, and obese asthmatics have more symptoms, frequent and severe exacerbations, a reduced response to asthma medications, and a decreased quality of life.
Asthma is a chronic inflammatory disease that impacts the airways of the lungs. It can be managed and controlled but not cured. Asthma can cause fatigue, which can also worsen asthma. Fatigue may be a sign of uncontrolled asthma, with symptoms such as shortness of breath, coughing, and wheezing, which can cause sleep disturbances and, consequently, daytime tiredness. Obesity can also exacerbate asthma symptoms, causing chronic coughing and disrupting sleep, which further contributes to fatigue.
The choice of a sedentary lifestyle, which may be influenced by asthma symptoms, can lead to physical deconditioning, aggravating asthma symptoms and increasing the risk of obesity. Patients with asthma have diminished activity patterns, which can result in impaired functional capacity and muscle weakness. This muscle weakness can be attributed to reduced motor neuron activity, decreased type I fibres, increased type IIb fibres, and reduced activity of enzymes involved in oxidative energy conversion. Additionally, corticosteroids, a common treatment for asthma, carry the risk of steroid-induced myopathy, causing respiratory muscle weakness.
Research has also found that adults with persistent asthma experience musculoskeletal dysfunction and chronic pain, with increased lower back, cervical, and shoulder pain compared to non-asthmatic subjects. These mechanical alterations related to the overload of respiratory muscles can lead to postural changes, muscle shortening, and decreased chest wall expansion, shoulder internal rotation, and thoracic spine flexibility.
How Muscle Loss Leads to Blood Pooling
You may want to see also
Explore related products




![]()
Asthma, muscle weakness, and fatigue
Asthma is an inflammatory disease that impacts the airways of the lungs. It is a chronic condition that can be managed and controlled but not cured. It is associated with several symptoms, including shortness of breath, coughing, wheezing, and sleep disturbances. These symptoms can lead to fatigue and tiredness, which is a common issue for people with asthma.
Fatigue is often a sign of uncontrolled asthma. The uncontrolled symptoms, such as coughing and wheezing, can cause sleep disturbances and nighttime flare-ups, resulting in daytime tiredness. Obesity can also exacerbate asthma symptoms, leading to disrupted sleep and increased fatigue. Additionally, the choice of a more sedentary lifestyle due to asthma can lead to physical deconditioning, aggravating asthma symptoms and further increasing fatigue.
Mechanical ventilation for severe asthma can lead to the development of diffuse muscle weakness due to acute myopathy. This myopathy may be caused by the use of corticosteroids and neuromuscular blocking agents, with a higher incidence of muscle weakness associated with the combined use of both treatments. Prolonged neuromuscular paralysis is a significant risk factor for the development of muscle weakness in these patients.
Asthma has also been linked to musculoskeletal dysfunction and chronic pain. Adults with persistent asthma may experience postural alterations, such as holding their head and shoulders more forward, decreased chest wall expansion, and reduced flexibility in the thoracic spine. These mechanical alterations may contribute to chronic pain in the lower back, cervical spine, and shoulders.
Overall, asthma can contribute to muscle weakness and fatigue through a combination of uncontrolled symptoms, sleep disturbances, obesity, sedentary lifestyle choices, medical treatments, and associated musculoskeletal dysfunction and pain. It is important for individuals with asthma to manage their symptoms effectively, maintain a healthy weight, and engage in suitable physical activities to help reduce the impact of asthma on their muscle strength and energy levels.
Lexapro Side Effects: Muscle Spasms Explained
You may want to see also
Explore related products





![]()
Asthma and musculoskeletal dysfunction
Asthma is an inflammatory disease that impacts the airways of the lungs. It is a chronic condition that can be managed and controlled but not cured. People with asthma often experience fatigue due to uncontrolled asthma symptoms, nocturnal asthma, asthma flare-ups, and asthma attacks. Obesity can also exacerbate asthma symptoms, leading to chronic coughing, disrupted sleep, and increased fatigue.
Several studies have found that adults with persistent asthma experience musculoskeletal dysfunction and chronic pain. Patients with asthma have diminished activity patterns, which can lead to deleterious physiologic alterations and impaired functional capacity. Lower limb fatigue, measured with the Borg scale, was found to be higher in asthmatic patients, suggesting that respiratory muscle weakness may be a factor.
Mechanical alterations related to the overload of respiratory muscles in adults with persistent asthma might lead to the development of chronic alterations in posture, musculoskeletal dysfunction, and pain. A study by Lunardi et al. (2011) found that compared to non-asthmatic subjects, patients with mild or severe persistent asthma held their head and shoulders more forward and had lower chest wall expansion, decreased shoulder internal rotation, and decreased thoracic spine flexibility. These mechanical alterations can lead to chronic lower back, cervical, and shoulder pain.
Additionally, patients who undergo mechanical ventilation for severe asthma are at risk of developing diffuse muscle weakness due to acute myopathy. The use of corticosteroids and neuromuscular blocking agents has been associated with a higher incidence of muscle weakness compared to the use of corticosteroids alone. However, the relative importance of corticosteroids and neuromuscular paralysis in causing myopathy is still controversial, and more research is needed to fully understand the relationship between asthma and musculoskeletal dysfunction.
How Muscles Affect Your Bowel Movement
You may want to see also
Frequently asked questions
Yes, asthma can cause muscle weakness. Patients with asthma have diminished activity patterns, which can lead to impaired functional capacity.
Asthma can cause muscle weakness due to reduced motor neuron activity, decreased percentage of type I fibers, increased percentage of type IIb fibers, and reduced activity of enzymes involved in oxidative energy conversion.
Yes, the administration of systemic corticosteroids, a common treatment for asthma, can also lead to steroid-induced myopathy and muscle weakness.
Respiratory and locomotor muscles are impacted in people with asthma, leading to abnormal exhalation of gases and physical deconditioning.
Asthma is often associated with fatigue and tiredness. This can be caused by uncontrolled asthma symptoms, sleep disturbances, and nighttime flare-ups, which can result in daytime fatigue. Mechanical ventilation for severe asthma can also increase the risk of developing diffuse muscle weakness.