Chronic Obstructive Pulmonary Disease (COPD) is a progressive lung disease that affects a significant number of people globally. COPD patients experience skeletal muscle dysfunction and wasting, which severely impacts their quality of life and survival. This is due to a combination of functional, metabolic, and anatomical alterations leading to suboptimal muscle work. Muscle atrophy, or muscle wasting, is a common symptom of COPD, and it can be caused by several factors, including inflammatory cytokines, oxidative stress, growth and anabolic hormones, nutritional status, and physical activity. The molecular and cellular events that occur in the lower extremity muscles lead to modifications in the muscle phenotype and function, contributing to muscle weakness. While the exact causes of muscle atrophy in COPD patients vary from person to person, it is clear that limiting muscle wasting can improve patients' quality of life and chances of survival.
| Characteristics | Values |
|---|---|
| Muscle dysfunction | Loss of strength or endurance |
| Muscle mass loss | Especially in the lower limbs |
| Comorbidities | Nutritional abnormalities, heart failure, and pulmonary hypertension |
| Exercise intolerance | Limited exercise capacity |
| Smoking | Cigarette smoking contributes to limb muscle dysfunction |
| Inflammation | No local inflammatory events in muscles of COPD patients |
| Oxidative stress | Inverse correlation with exercise capacity, body composition, and quadriceps strength |
| Molecular and cellular events | Modifications in the muscle phenotype and function |
| Survival | Muscle integrity increases chances of survival from COPD |
| Therapeutic opportunities | Pharmacological therapies and strength exercises |
Explore related products






What You'll Learn
![]()
COPD is associated with muscle wasting and weakness
Chronic obstructive pulmonary disease (COPD) is a progressive lung disease that affects a significant number of people globally. COPD is associated with muscle wasting and weakness, which can severely impact a patient's quality of life and survival. This muscle dysfunction is a result of a combination of functional, metabolic, and anatomical alterations, leading to suboptimal muscle work.
Muscle wasting and weakness are common in patients with COPD, and can affect both ventilatory and non-ventilatory muscle groups. This can lead to a loss of strength and endurance, impairing the patient's exercise capacity and daily activities. The mid-thigh cross-sectional area and quadriceps weakness, defined as a decline in force-generating capacity, strongly influence a patient's ability to perform physical tasks.
The mechanisms behind muscle wasting in COPD are complex and likely involve multiple factors. Inflammatory cytokines, oxidative stress, growth and anabolic hormones, nutritional status, and physical activity levels all play a role. High CO2 levels, for example, can cause skeletal muscle atrophy through various biological mechanisms. Cigarette smoking is also a significant contributor to limb muscle dysfunction in COPD, leading to decreased type I fiber sizes and proportions, as well as reduced mitochondrial activity.
In addition, COPD patients may experience a shift in fiber type composition, resulting in a slow-to-fast transition. This change can lead to muscle fatigue and weakness. The activation of the ubiquitin-proteasome pathway has also been implicated in peripheral skeletal muscle wasting during COPD, resulting in a loss of myosin and force-generating capacity. Furthermore, disuse, hypoxemia, malnutrition, oxidative stress, and systemic inflammation may all contribute to muscle atrophy in COPD patients.
The good news is that muscle wasting in COPD may be treatable, and there are emerging therapeutic approaches to tackle this issue. These include pharmacological therapies currently in development for muscle atrophy in other pathological states, which may also be relevant for treating muscle wasting in COPD patients. Additionally, muscle recovery measures such as pulmonary rehabilitation, optimised nutrition, and other strategies have been associated with a better prognosis when administered to stable patients and those experiencing exacerbations.
High Blood Pressure Medication: Muscle Cramp Culprit?
You may want to see also
Explore related products






![]()
COPD causes atrophy of limb muscles
Chronic Obstructive Pulmonary Disease (COPD) is a progressive lung disease that affects a significant number of people globally. It is an inflammatory condition that damages the lungs and often co-occurs with other chronic conditions such as cardiovascular disease and diabetes. COPD is associated with muscle dysfunction and wasting, which can severely impact a patient's quality of life and survival.
Muscle atrophy, or wasting, is a common symptom of COPD, particularly in the lower limbs. This atrophy leads to a loss of strength and endurance in the muscles, impairing the patient's exercise capacity and daily activities. The atrophy occurs due to a combination of functional, metabolic, and anatomical alterations, resulting in suboptimal muscle work. The diaphragm, in particular, is affected, leading to respiratory issues.
Several factors contribute to limb muscle atrophy in COPD patients. One of the main causes is cigarette smoking, which decreases type I fiber sizes and proportions, reduces mitochondrial activity, and increases oxidative stress levels. Other factors include disuse or inactivity, hypoxemia, malnutrition, oxidative stress, and systemic inflammation. The exact causes may vary from person to person, and it is likely that each individual has a unique combination of factors contributing to muscle atrophy.
The mechanisms of skeletal muscle dysfunction in COPD are complex and involve multiple biological processes. One hypothesis suggests that the disease causes immobilization and deconditioning, leading to peripheral muscle dysfunction. Another hypothesis proposes that high CO2 levels activate certain proteins and kinases, resulting in skeletal muscle atrophy. Additionally, a fiber-type switch from slow-twitch to fast-twitch fibers is observed in patients with advanced COPD, contributing to muscle weakness and atrophy.
To combat muscle atrophy and improve patients' quality of life, various therapeutic approaches are being explored. These include pharmacological therapies, pulmonary rehabilitation, optimized nutrition, and strength exercises. While there is currently no cure for COPD, these strategies can help slow the progression of the disease and improve patients' independence and comfort.
Facet Joint Injections: Unwanted Muscle Spasms?
You may want to see also
Explore related products






![]()
COPD patients experience skeletal muscle dysfunction
Skeletal muscle dysfunction is a major problem for many patients with chronic obstructive pulmonary disease (COPD). It affects both ventilatory and non-ventilatory muscle groups, leading to worse outcomes, including increased mortality and hospitalisation rates. It is associated with a poor quality of life and reduced survival rates.
Muscle dysfunction impairs a patient's exercise capacity and quality of life as daily life activities may be hampered by this problem. It is more significant in the lower limbs, compromising patients' ambulatory capacity and having a devastating effect on their daily lives. Skeletal muscle dysfunction occurs in about 40% of patients, limiting their exercise capacity.
Muscle dysfunction is a consequence of a complex combination of functional, metabolic, and anatomical alterations leading to suboptimal muscle work. Muscle atrophy, altered fibre type and metabolism, and chest wall remodelling are relevant etiological contributors to this process. A fibre-type switch from slow-twitch to fast-twitch fibres is a major feature in the vastus lateralis of patients with advanced COPD. Fast-twitch fibres are also smaller in patients with advanced COPD and poor muscle mass, thus contributing to muscle weakness.
Factors such as ageing, malnutrition, and systemic corticosteroid treatment may worsen the fast-twitch fibre atrophy observed in COPD. A reduction in capillary numbers and contacts could eventually impair oxygen delivery to the myofibers, providing another contributing biological mechanism. Cigarette smoking may also contribute to limb muscle dysfunction in COPD through several biological mechanisms, including decreased type I fibre sizes and proportions and reduced mitochondrial activity.
Anxiety Medication and Muscle Twitching: What's the Link?
You may want to see also
Explore related products






![]()
COPD patients have a reduced quality of life and survival rate
Chronic obstructive pulmonary disease (COPD) is a progressive disease that can lead to a reduced quality of life and survival rate for patients. COPD is characterised by persistent respiratory symptoms and airflow limitation, resulting in significant physical and psychological impacts on patients' well-being.
COPD patients often experience muscle wasting and dysfunction, which contributes to a decline in their overall quality of life. Muscle wasting in COPD patients is associated with a shift in fibre type composition, resulting in muscle weakness and early onset of muscle fatigue. This leads to exercise intolerance, impacting their daily activities and overall physical health. Additionally, the dyspnea spiral further exacerbates the problem, where patients avoid exertion to prevent dyspnea, resulting in a decline in fitness and an earlier occurrence of dyspnea.
The molecular basis of muscle atrophy in COPD involves oxidative stress, inflammation, and cigarette smoking. Oxidative stress markers inversely correlate with exercise capacity, body composition, and muscle strength. Cigarette smoking contributes to limb muscle dysfunction by decreasing type I fibre sizes, reducing mitochondrial activity, and increasing oxidative stress levels. These factors collectively impact the patients' ability to perform daily tasks and maintain their physical health, leading to a decreased quality of life.
Furthermore, COPD exacerbations significantly impact patients' quality of life and survival rates. Exacerbations result in decreased lung function, reduced physical activity levels, and detrimental effects on mental health. Hospitalisations due to COPD exacerbations carry a high risk of mortality, with a significant number of patients dying within a year of discharge. Comorbidities associated with COPD, such as nutritional abnormalities, heart failure, and pulmonary hypertension, further contribute to reduced quality of life and survival rates.
The prognosis and survival of COPD patients are also influenced by muscle dysfunction and mass loss. Quadriceps muscle weakness and atrophy are associated with advanced COPD, impacting patients' mobility and overall health. Early diagnosis, proactive treatment, and adherence to medications are critical for improving patients' quality of life and reducing mortality. Single-inhaler triple therapies have shown promising results in reducing mortality risk compared to other treatments.
Muscle Spasms: A Surprising Fever Cause
You may want to see also
Explore related products






![]()
COPD is an inflammatory condition that damages the lungs
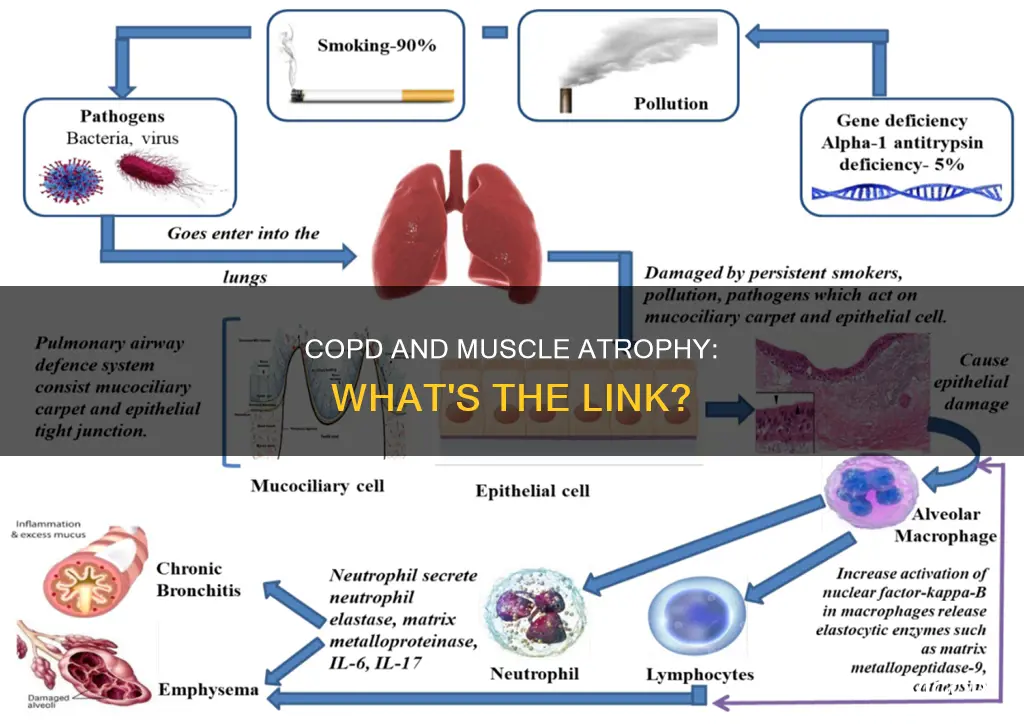
Chronic obstructive pulmonary disease (COPD) is a condition caused by damage to the airways or other parts of the lungs. This damage leads to inflammation and other problems that block airflow and make it hard to breathe. COPD is a progressive disease, and its symptoms often develop slowly but worsen over time. It can cause coughing that produces large amounts of mucus, shortness of breath, chest tightness, and other symptoms. It is a major cause of disability and is the sixth leading cause of death in the United States. Worldwide, COPD will become a leading cause of death over the next few years.
COPD is a chronic inflammatory lung disease causing tissue destruction and irreversible airflow limitation. Histopathologic findings include an increase in inflammatory cells, structural changes, and lymphoid follicles. Emphysema, which is common in COPD patients, is characterised by the destruction of the alveolar air sacs (gas-exchanging surfaces of the lungs) leading to obstructive physiology. This destruction is caused by an inflammatory response to irritants such as smoking. The inflammatory response involves the recruitment of neutrophils and macrophages, which release multiple inflammatory mediators, resulting in the destruction of the air sacs.
In addition to the direct damage caused by inflammation, COPD also contributes to muscle atrophy through several mechanisms. Firstly, oxidative stress and inflammation have been associated with muscle dysfunction in COPD patients, particularly through decreased type I fibre sizes and proportions and reduced mitochondrial activity. Secondly, cigarette smoking contributes to limb muscle dysfunction through biological mechanisms, including increased oxidative stress levels. Thirdly, disuse contributes significantly to alterations in skeletal muscle structure and function during COPD. Finally, other frequent comorbidities associated with COPD, such as nutritional abnormalities, heart failure, and pulmonary hypertension, may further contribute to skeletal muscle mass loss and dysfunction.
Muscle dysfunction and wasting are common in COPD patients and can impair their exercise capacity and quality of life. Quadriceps muscle weakness and atrophy are associated with advanced COPD. A fiber-type switch from slow-twitch to fast-twitch fibres is observed in the vastus lateralis of patients with advanced COPD, contributing to muscle weakness. Additionally, factors such as ageing, malnutrition, and systemic corticosteroid treatment may worsen the fast-twitch fiber atrophy observed in COPD. Overall, muscle atrophy and dysfunction are significant complications of COPD, impacting patients' quality of life and survival.
Carbon Monoxide: An Unseen Danger Causing Muscle Pain
You may want to see also
Frequently asked questions
Chronic Obstructive Pulmonary Disease (COPD) is a progressive lung disease that constitutes a major global health burden.
COPD causes muscle atrophy through several molecular and cellular events that mediate the effects of different etiologic factors, leading to modifications in the muscle phenotype and function. Factors such as ageing, malnutrition, and systemic corticosteroid treatment may worsen muscle atrophy.
Symptoms of muscle atrophy in COPD patients include muscle weakness, especially in the legs, and a decrease in exercise capacity and quality of life.
Muscle atrophy in COPD patients can be treated through pulmonary rehabilitation, optimised nutrition, and other strategies. Quitting smoking and engaging in physical activity can also help.































