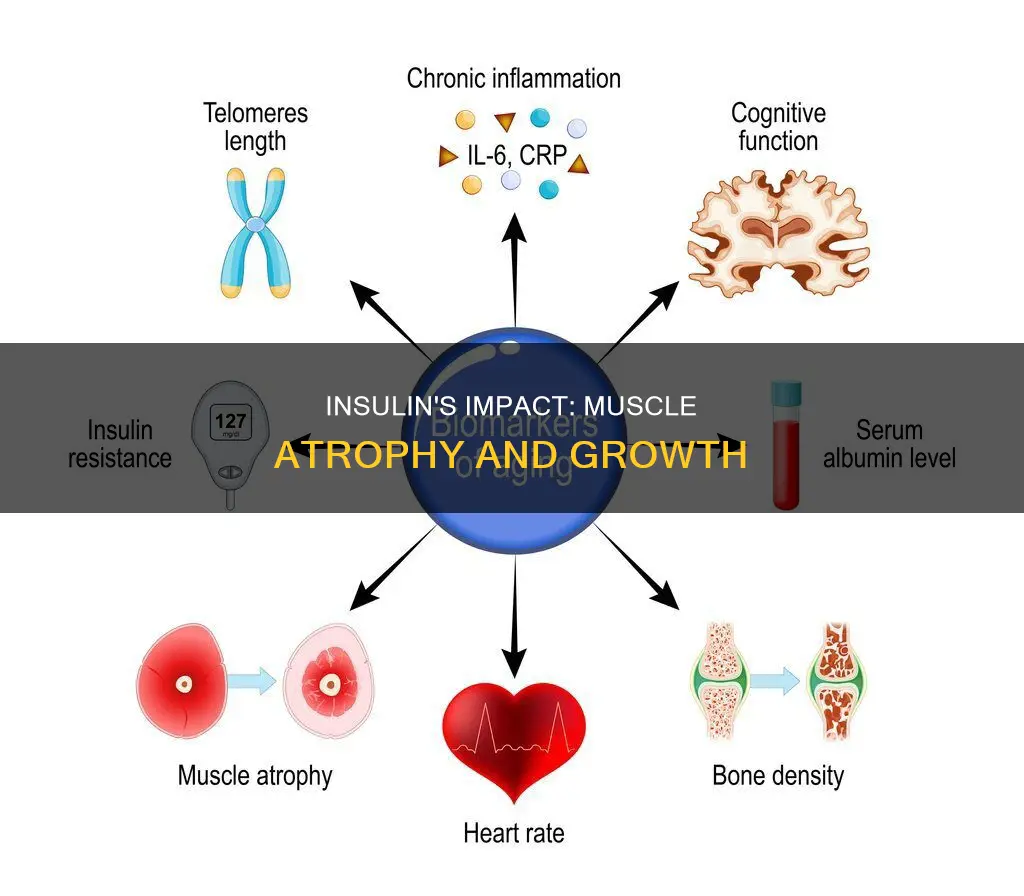
Insulin is a hormone that plays a crucial role in maintaining blood sugar levels in the body. Insufficient insulin or insulin resistance can lead to diabetes, which is associated with various health complications, including muscle atrophy or loss of skeletal muscle mass. While the exact mechanisms are not fully understood, research suggests that insulin resistance may contribute to muscle atrophy, especially in individuals with type 2 diabetes mellitus (T2DM). Studies have shown that insulin resistance can accelerate muscle protein degradation and suppress muscle protein synthesis, leading to a decline in skeletal muscle mass. Additionally, certain conditions such as acidosis, uremia, and sepsis, which are characterized by insulin resistance, may also play a role in muscle atrophy. Understanding the relationship between insulin and muscle atrophy has important implications for developing treatments for muscle-wasting conditions and improving overall health outcomes.
| Characteristics | Values |
|---|---|
| Insulin | Lowers blood sugar levels |
| Insulin | Promotes the growth and proliferation of cells |
| Insulin insufficiency | Thought to result in the suppression of growth and proliferation of muscle cells |
| Insulin insufficiency | Contributes to the decline in skeletal muscle mass |
| Insulin resistance | May be sufficient to cause muscle atrophy |
| Insulin resistance | Leads to muscle wasting |
| Insulin resistance | Causes muscle protein degradation |
| Insulin resistance | Is a major risk factor for type 2 diabetes |
| Insulin resistance | May be caused by obesity and inflammation |
| Insulin resistance | Is associated with muscle atrophy |
Explore related products






What You'll Learn
![]()
Insulin resistance and muscle atrophy
Insulin resistance is a condition in which muscle cells become resistant to the effects of insulin, a hormone that regulates blood sugar levels. Insulin resistance can lead to elevated blood sugar levels, which can have detrimental effects on various organs and tissues, including skeletal muscle.
Several studies have shown that insulin resistance is associated with muscle atrophy, or muscle wasting. In particular, insulin resistance has been found to accelerate muscle protein degradation through the activation of the ubiquitin-proteasome pathway, resulting in a decline in skeletal muscle mass. This decline in skeletal muscle mass is further exacerbated by insufficient insulin action, which contributes to the suppression of muscle cell growth and proliferation.
Research has also shown that certain proteins play a key role in diabetes-induced muscle mass loss. Specifically, the proteins KLF15 and WWP have been implicated in muscle atrophy associated with elevated blood sugar levels. Additionally, it has been found that the absence of KLF15 in the skeletal muscle of diabetic mice prevented diabetes-induced skeletal muscle mass decline, suggesting that this protein may be a critical factor in the process.
Furthermore, studies in mouse models of type 2 diabetes (T2DM) have provided valuable insights into the relationship between insulin resistance and muscle atrophy. For example, the db/db mouse model exhibits insulin resistance and reduced skeletal muscle size before the onset of chronic hyperglycemia, indicating that insulin resistance may be a sufficient factor for muscle atrophy independent of overt T2DM. Similarly, the TallyHo mouse model, which develops diabetes at a mature age, allows for the investigation of the impact of insulin resistance and hyperglycemia on fully developed muscle, providing clinically relevant insights into the progression and causal mechanisms of muscle atrophy in T2DM.
While the exact causal relationship between insulin resistance and muscle atrophy remains unclear, it is evident that the two are closely linked. Further research is needed to fully understand the underlying mechanisms and potential therapeutic interventions for muscle wasting associated with insulin resistance.
Muscle Pain: Tumor's Uncomfortable Touch
You may want to see also
Explore related products





![]()
Diabetes and muscle loss
Diabetes is associated with various health problems, including a decline in skeletal muscle mass. Insulin lowers blood sugar levels and promotes the growth and proliferation of cells. Insufficient insulin action has been linked to the suppression of muscle cell growth and proliferation, contributing to muscle atrophy.
Research has shown that a rise in blood sugar levels triggers a decline in muscle mass. Two proteins, KLF15 and WWP, have been identified as playing a crucial role in this process. Mice lacking KLF15 specifically in their muscles were found to be resistant to diabetes-induced skeletal muscle mass decline. These findings suggest that diabetes-induced muscle loss is due to increased KLF15 levels.
Additionally, insulin resistance has been linked to muscle wasting and atrophy. Conditions such as acidosis, uremia, and sepsis exhibit insulin resistance and muscle atrophy. Studies in mice have shown that insulin resistance may be sufficient to cause muscle atrophy before the onset of type 2 diabetes. Furthermore, muscle atrophy in patients with type 2 diabetes mellitus (T2DM) is associated with reduced Akt activation, leading to increased FoxO transcription factors and upregulation of specific ubiquitin ligases, which contribute to muscle degradation.
The relationship between insulin resistance and muscle atrophy is complex. While insulin resistance can lead to muscle atrophy, sarcopenia, a condition characterized by reduced muscle mass and function, can also result in insulin resistance. This bidirectional relationship indicates that addressing one issue may not necessarily resolve the other.
Currently, no drug is available to treat muscle loss directly. However, researchers are exploring the possibility of developing a drug that strengthens WWP1 or weakens KLF15, which could lead to a groundbreaking new treatment for diabetes-induced muscle loss.
Lactic Acid: Friend or Foe in Muscle Pain?
You may want to see also
Explore related products






![]()
The role of proteins in muscle atrophy
Insulin resistance has been found to accelerate muscle protein degradation, activating the ubiquitin-proteasome pathway. This pathway is one of the two most important cell proteolytic systems that control protein turnover in muscle. The other is the autophagy-lysosome machinery.
Muscle mass, like any other tissue, depends on protein turnover and cell turnover. Atrophy is defined as a decrease in the size of a tissue or organ due to cellular shrinkage, caused by the loss of organelles, cytoplasm, and proteins.
Insulin and insulin-like growth factor 1 (IGF-1) are potent anabolic factors that sustain muscle growth. They bind to specific receptors that activate a cascade of phosphorylation events that positively or negatively modulate proteins, enzymes, or transcription factors. This pathway regulates protein synthesis, protein degradation, cellular proliferation, and survival, as well as glucose uptake and energy production.
Several proteins have been identified as playing a role in muscle atrophy. For example, a protein belonging to the TGF-β family, known as myostatin, has been shown to be a strong negative regulator of muscle growth. Knockout or mutation of this protein results in enlarged muscles. The first ubiquitin ligases that were identified to play a role in muscle loss were Atrogin-1/MAFbx and MuRF1, which are considered the master genes of muscle atrophy. MuRF1 ubiquitinates several muscle structural proteins, including troponin I, myosin heavy chains, actin, myosin-binding protein C, and myosin light chains 1 and 2.
In the context of diabetes, research has revealed that an elevation of blood sugar levels leads to muscle atrophy and that two proteins, KLF15 and WWP, play key roles in this phenomenon. Mice that lack KLF15 in their muscles were found to be resistant to diabetes-induced skeletal muscle mass decline, indicating that diabetes-induced muscle loss is attributable to increased amounts of KLF15.
Understanding Leg Muscle Weakness: Causes and Triggers
You may want to see also
Explore related products





![]()
Exercise and muscle atrophy
Exercise is a common treatment for muscle atrophy. It helps relieve symptoms of atrophy by rebuilding strength and mass. Physiologic atrophy, caused by not using muscles enough, can often be reversed with exercise and better nutrition.
There are various exercises that can help with muscle atrophy. Dr Gallucci recommends leg raises, which strengthen the quadriceps and hip flexors, helping to maintain lower body strength and improving mobility. Dr Gallucci also recommends squats, which target the quadriceps, hamstrings, and glutes.
For those who cannot actively move one or more joints, exercises can be done using braces or splints. Exercises in a swimming pool can also help to reduce the muscle workload.
Neuromuscular reeducation, or vibration therapy, is another way to treat muscle atrophy. This therapy involves sending vibrations throughout a patient’s body, causing their muscles to contract and relax dozens of times per second, working the muscles as exercise would. This therapy can also improve balance and performance.
Muscle atrophy can be caused by diabetes, specifically by an elevation of blood sugar levels. Insulin resistance has been shown to accelerate muscle protein degradation, leading to muscle wasting.
Levofloxacin's Link to Muscle Atrophy: What You Need to Know
You may want to see also
Explore related products


![]()
Age and muscle atrophy
Insulin plays a role in muscle atrophy, particularly in the context of diabetes. Insulin resistance and diabetes are linked to muscle wasting and atrophy. However, the specific contribution of insulin resistance to muscle atrophy is still under investigation.
Age-related muscle atrophy, also known as sarcopenia, is a common condition affecting older adults. Sarcopenia is characterised by a progressive loss of muscle mass, strength, and function, leading to a decline in physical independence. The condition primarily occurs due to the natural ageing process, with muscle loss typically starting around the age of 30 and progressing at a faster rate after 60. The specific rate of muscle loss varies between individuals, with estimates ranging from 3% to 5% of muscle mass lost per decade after age 30.
Several factors contribute to sarcopenia. Firstly, ageing is associated with a decrease in the production of proteins essential for muscle growth, resulting in smaller muscle cells. Secondly, hormonal changes, including lower levels of testosterone and insulin-like growth factor (IGF-1), can affect muscle fibres and contribute to sarcopenia. Additionally, neurological decline, inflammatory pathway activation, reduced physical activity, chronic illness, fatty infiltration, and poor nutrition are also considered contributing factors to age-related muscle atrophy.
The impact of sarcopenia can be significant, impairing an individual's ability to perform daily tasks and reducing their quality of life. However, it is important to note that sarcopenia is not inevitable with ageing, and staying physically active can significantly reduce the risk of developing this condition. Additionally, adequate nutrition, particularly sufficient protein intake, is crucial in mitigating age-related muscle loss. While there is no drug treatment available for muscle loss, interventions such as strength training and targeted exercises can help treat and even reverse the effects of sarcopenia.
Impaired Blood Flow: Muscle Fatigue Culprit
You may want to see also
Frequently asked questions
Insulin resistance accelerates muscle protein degradation, which can lead to muscle atrophy. Insulin resistance may be caused by several mechanisms, including chronically increased production of reactive oxygen species and mitochondrial dysfunction.
Insulin resistance causes muscle wasting by suppressing PI3K/Akt signalling, leading to activation of caspase-3 and the ubiquitin-proteasome proteolytic pathway, causing muscle protein degradation.
Yes, diabetes is associated with muscle atrophy. A longitudinal study found that untreated diabetic individuals lost 435 g of muscle per year, compared to 193 g for non-diabetics.