Diplopia, or double vision, occurs when the two eyes do not move together in a coordinated manner, resulting in the formation of two disparate images. This can be caused by a variety of factors, including ocular motility disorders, brainstem gaze palsies, cranial neuropathies, and primary orbital disease. One specific cause of diplopia is the trapping or entrapment of the inferior oblique muscle, which is a known complication of orbital fractures and, in rare cases, transconjunctival lower lid blepharoplasty. The inferior oblique muscle is one of six extraocular muscles that control eye movement, and its trapping can lead to a reduction in motility and diplopia. While this condition is uncommon, it is important to understand its causes and potential treatments to ensure proper diagnosis and care.
| Characteristics | Values |
|---|---|
| Inferior oblique muscle palsy | Can be caused by transconjunctival lower lid blepharoplasty |
| Double vision | Caused by the absence of retinal correspondence |
| Transconjunctival lower lid blepharoplasty | Does not leave a scar on the skin and causes fewer adverse effects |
| Torsional diplopia | Caused by underaction of a superior or inferior oblique eye muscle |
| Treatment for diplopia | Spontaneous improvement, strabismus correction surgery, re-suturing the cut muscle, repositioning the muscle in the orbit |
Explore related products






What You'll Learn
- Orbital floor fractures can cause inferior oblique entrapment, leading to diplopia
- Transconjunctival lower lid blepharoplasty can result in transient or permanent inferior oblique muscle palsy and diplopia
- Techniques such as re-suturing the cut muscle or repositioning it in the orbit can be used to treat diplopia caused by inferior oblique entrapment
- The double-Maddox rod test can be used to diagnose torsional diplopia caused by inferior oblique muscle weakness
- Gaze and vision issues can be caused by the lagging of the left inferior oblique muscle, resulting in diplopia
![]()
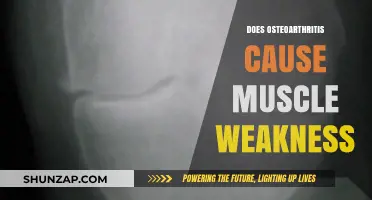
Orbital floor fractures can cause inferior oblique entrapment, leading to diplopia
Orbital floor fractures are a common type of facial injury, accounting for up to 40% of all trauma injuries in the mid-face region. These fractures can occur when a blunt object strikes the eye, transmitting force throughout the orbit and causing a fracture of the orbital floor. While the globe of the eye usually remains intact, the force can result in the entrapment of various structures within the fracture, including muscles, fat, and connective tissue.
One of the muscles that can become entrapped in an orbital floor fracture is the inferior rectus muscle. This entrapment can lead to a condition called residual diplopia (RD), where a patient experiences double vision. In some cases, RD can persist even after secondary corrective surgeries, although it may resolve spontaneously within 8 weeks or with the use of prisms for complete correction.
In addition to the inferior rectus muscle, other periorbital musculature can also become entrapped in orbital floor fractures. This includes the extraocular muscles, of which there are six: four rectus muscles and two oblique muscles, one of which is the inferior oblique muscle. While there are limited reports specifically mentioning the entrapment of the inferior oblique muscle in orbital floor fractures, it is reasonable to assume that this muscle could become entrapped, similar to the inferior rectus muscle.
The inferior oblique muscle is positioned deep within the orbit, and its function is to intort and extort the globe, or turn it clockwise or counter-clockwise. When this muscle is affected, it can result in torsional diplopia, where one image is rotated away from the other. While there are other causes of torsional diplopia, such as myasthenia gravis or transient inferior oblique muscle palsy following blepharoplasty, the entrapment of the inferior oblique muscle in an orbital floor fracture could potentially lead to similar symptoms of diplopia.
In conclusion, orbital floor fractures can cause the entrapment of various muscles, including the inferior rectus muscle, leading to diplopia. While there may be a lack of specific reports mentioning the inferior oblique muscle entrapment, its location within the orbit and its function suggest that it could also become entrapped in an orbital floor fracture, potentially resulting in diplopia. Therefore, it is important to consider this muscle when evaluating and treating patients with orbital floor fractures to ensure comprehensive care and management of diplopia.
Muscle Relaxers: Blurred Vision Side Effect?
You may want to see also
Explore related products






![]()
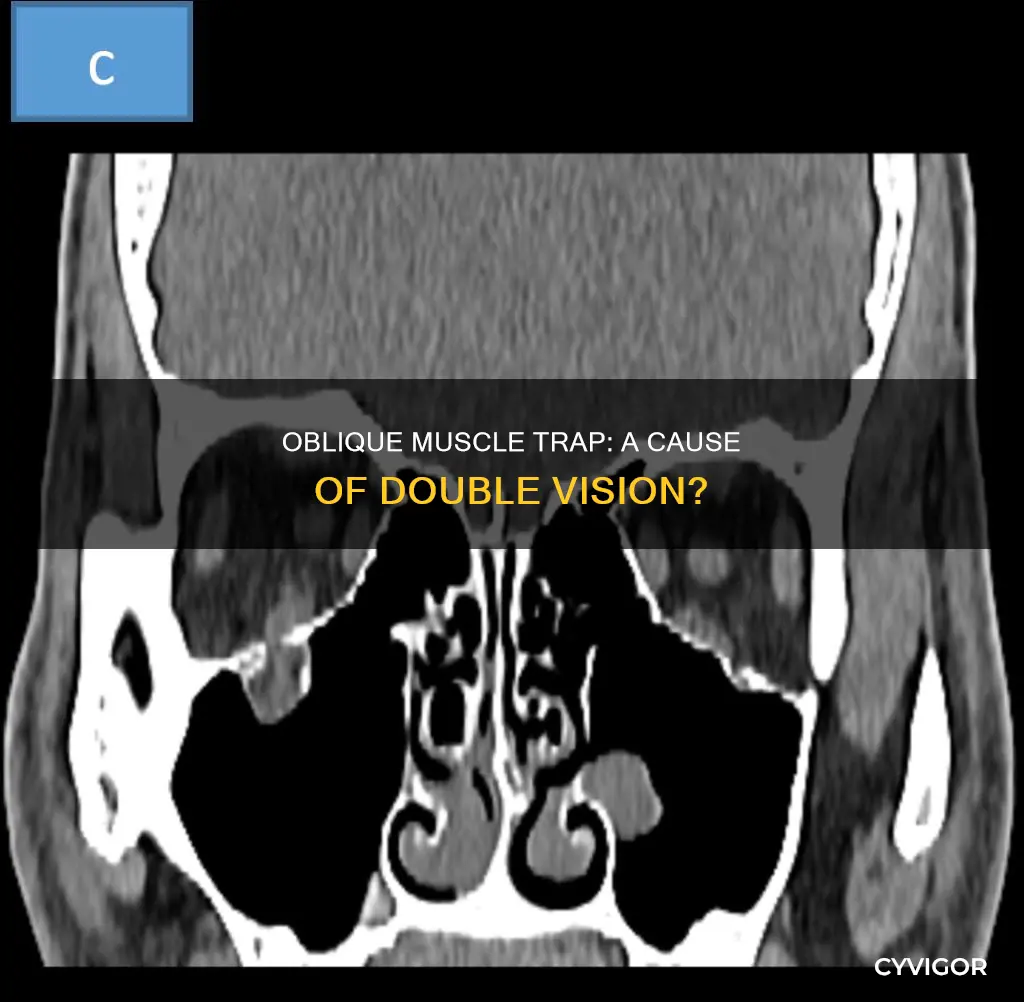
Transconjunctival lower lid blepharoplasty can result in transient or permanent inferior oblique muscle palsy and diplopia
Transconjunctival lower lid blepharoplasty is a type of aesthetic surgery that is performed to improve the appearance of the lower eyelid. The procedure involves making an incision inside the lower eyelid to remove excess fat and tighten the skin, resulting in a more youthful and alert appearance. While this procedure is generally safe and effective, there are some potential risks and complications that can occur.
One rare but significant complication of transconjunctival lower lid blepharoplasty is inferior oblique muscle palsy, which can lead to diplopia or double vision. The inferior oblique muscle is located deep within the orbit and plays a crucial role in eye movement. During the blepharoplasty procedure, this muscle can be inadvertently damaged, leading to palsy or paralysis. The exact incidence of this complication is unknown, but it has been reported in a small number of cases internationally.
The symptoms of inferior oblique muscle palsy typically include diplopia, particularly when gazing in the upper and right upper direction. In some cases, patients may also experience restriction of eye movements, such as in sursumversion, deorsumversion, and abduction. These symptoms can be quite debilitating and negatively impact an individual's quality of life. Therefore, it is essential to carefully inform patients about the possibility of diplopia before performing cosmetic blepharoplasty with a transconjunctival approach.
The diplopia resulting from inferior oblique muscle palsy can be transient or permanent. In most cases, the diplopia resolves within a few months, with complete recovery occurring in 2 to 6 months. However, in some rare instances, the diplopia may persist for longer or even become permanent. Prolonged diplopia may indicate more severe injury to the extraocular muscle, including intramuscular hemorrhage or muscle transection. Thus, it is crucial to closely monitor patients following blepharoplasty and provide prompt treatment if diplopia occurs.
To diagnose inferior oblique muscle palsy, several tests can be performed, such as the alternate prism cover test, the double Maddox rod test, and the Lancaster test. These tests help assess eye movement, measure the degree of diplopia, and monitor the improvement of symptoms over time. In some cases, corticosteroid therapy or surgical exploration may be necessary to treat diplopia and restore normal eye function.
Understanding Muscle Tears: Causes and Prevention
You may want to see also
Explore related products





![]()
Techniques such as re-suturing the cut muscle or repositioning it in the orbit can be used to treat diplopia caused by inferior oblique entrapment
The inferior oblique (IO) muscle is positioned deep in the orbit. Its disinsertion or myotomy during orbital surgery can lead to diplopia, a condition characterised by double vision. This is because the IO plays a role in intorsion and extorsion of the globe.
In some cases, diplopia can be caused by entrapment of the IO muscle following an orbital fracture. This can be addressed through surgical repair, which may involve transecting and repositioning the IO muscle within the orbit. Techniques such as re-suturing the cut muscle or repositioning it in the orbit can be used to treat diplopia caused by inferior oblique entrapment.
For instance, in a case study of an 84-year-old woman who sustained an orbital fracture, the IO muscle was successfully repositioned during surgery, and the patient did not develop diplopia or experience motility disruption postoperatively. Similarly, in a case of IO entrapment following a zygomaticomaxillary complex fracture, the IO muscle was transected and repositioned within the orbit, resulting in no damage to extraocular motility or subjective diplopia.
In addition to repositioning the IO muscle, addressing any herniated orbital tissue is crucial for successful repair. This involves repositioning the herniated tissue back into the orbit. However, it is important to note that even with a perfect repair, residual or permanent diplopia can still occur if the inferior rectus muscle is damaged. Furthermore, fat atrophy may occur, and enophthalmos may not be completely eliminated.
In summary, techniques such as re-suturing and repositioning the IO muscle within the orbit are effective approaches to treating diplopia caused by inferior oblique entrapment. These techniques are often utilised during surgical repair of orbital fractures, and they can help restore normal eye movement and alleviate double vision.
Keppra's Impact: Muscle Weakness and Its Causes
You may want to see also
Explore related products






![]()
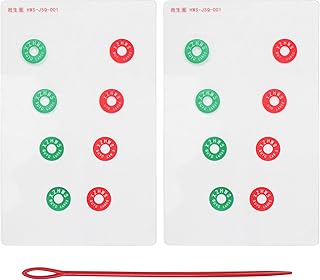
The double-Maddox rod test can be used to diagnose torsional diplopia caused by inferior oblique muscle weakness
The Maddox rod test can be used to subjectively detect and measure latent, manifest, horizontal, or vertical strabismus for near and distance. The test is based on the principle of diplopic projection. Dissociation of the deviation is brought about by presenting a red line image to one eye and a white light to the other, while prisms are used to superimpose these and effectively measure the angle of deviation (horizontal and vertical). The strength of the prism is increased until the streak of light passes through the centre of the prism, as the strength of the prism indicates the amount of deviation present. The Maddox rod is a handheld instrument composed of a red parallel plano-convex cylinder lens, which refracts light rays so that a point source of light is seen as a line or streak of light.
The double Maddox rod test is performed by placing Maddox rods into trial frames, one before each eye. Cylinders are placed into the trial frame vertically, making the two red lines horizontal. Vertical prisms (base-up or base-down) can also be added into the trial frames to separate the two red lines. The patient is then asked to fixate on a light source at 33 cm, which is held at eye level. The degree of deviation and the direction (incyclo or excyclo) can be determined by the angle of rotation that causes the line images to appear horizontal and parallel. The amount of cyclodeviation is measured in degrees, utilised from the scale on the trial frame.
The double Maddox rod test is particularly useful for diagnosing torsional diplopia caused by inferior oblique muscle weakness. This is because the test can measure the amount of deviation and the direction of the deviation, which is important for diagnosing torsional diplopia. Additionally, the test can help to differentiate between a skew deviation and other causes of vertical strabismus.
There are other tests that can be used to diagnose torsional diplopia caused by inferior oblique muscle weakness, such as the three-step test and the subjective red-glass test. However, the double Maddox rod test is a more sensitive test and can provide more detailed information about the deviation.
Flagyl's Muscle Pain: How Long Does it Last?
You may want to see also
Explore related products






![]()
Gaze and vision issues can be caused by the lagging of the left inferior oblique muscle, resulting in diplopia
The inferior oblique muscle is positioned deep in the orbit and plays a crucial role in eye movement. It is one of the extraocular muscles (EOMs) that control the movement of the eyes. When the inferior oblique muscle is affected, it can lead to diplopia, a condition where a person sees two images that are rotated clockwise or counter-clockwise away from each other. This is known as torsional diplopia and is characterised by the images becoming disparate.
Diplopia can be caused by various factors, including orbital fractures, blepharoplasty, and muscle weakness or palsy. In rare cases, monocular inferior oblique muscle palsy has been reported following transconjunctival lower lid blepharoplasty, a type of cosmetic surgery. This can result in diplopia, particularly when gazing in the upper or right upper direction. However, in most cases, diplopia resolves within a few months without any lasting postoperative motility deficits.
To diagnose diplopia, tests such as the red-glass test, double-Maddox rod test, and alternate prism cover test can be performed. These tests help to assess the relative positions of the disparate images and document torsional diplopia. Treatment options for diplopia may include strabismus correction surgery or repositioning the muscle within the orbit. In some cases, diplopia may resolve spontaneously without any intervention.
It is important to note that diplopia can also be a symptom of other underlying conditions, such as myasthenia gravis, brainstem gaze palsies, cranial neuropathies, or primary orbital disease. Therefore, a comprehensive evaluation is necessary to determine the underlying cause and provide appropriate treatment.
Skin Cancer and Muscle Pain: Is There a Link?
You may want to see also
Frequently asked questions
Diplopia is a condition where a patient sees two images, with one image being rotated clockwise or counter-clockwise away from the other. This is also known as double vision.
Diplopia occurs when the images do not fall on corresponding retinal points. This can be caused by a variety of factors, including the underaction of a superior or inferior oblique eye muscle, brainstem gaze palsies, cranial neuropathies, and primary orbital disease.
Yes, the entrapment of the inferior oblique muscle is a known complication of orbital fractures and can result in diplopia. In rare cases, diplopia can also occur following transconjunctival lower lid blepharoplasty, a type of aesthetic surgery.
The treatment for diplopia depends on the underlying cause. In some cases, diplopia may resolve on its own, while in others, surgery or other treatments may be required. For example, in cases of IO entrapment during orbital fracture repair, the muscle can be transected and repositioned within the orbit to correct the issue.