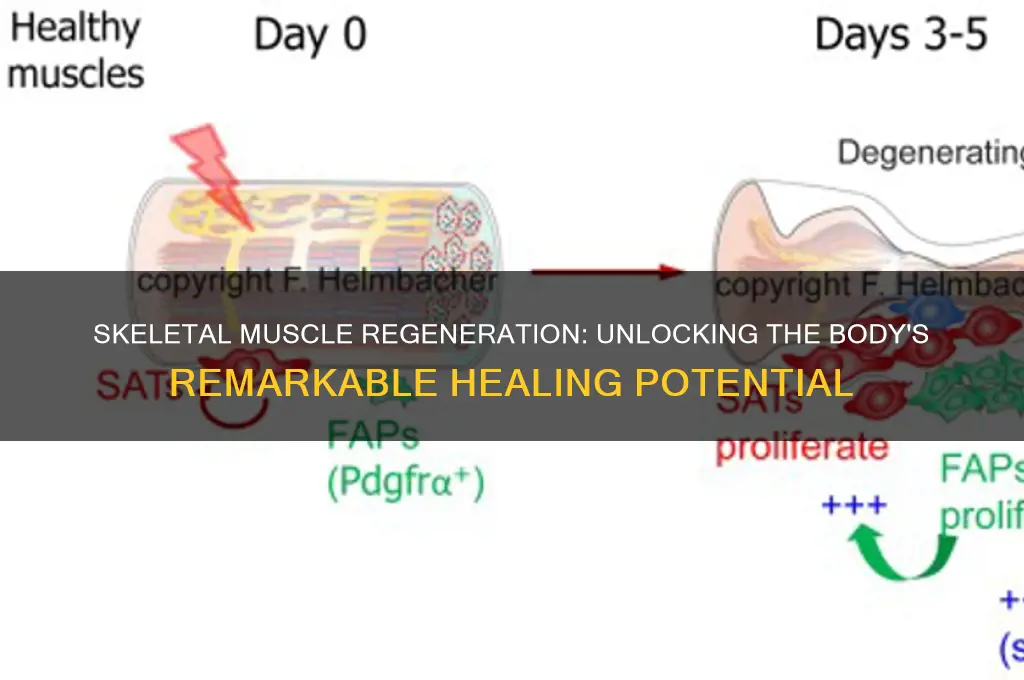
Skeletal muscle, a highly adaptable tissue, possesses a remarkable capacity for regeneration, primarily attributed to its resident stem cells known as satellite cells. When muscle fibers are damaged due to injury or disease, satellite cells become activated, proliferate, and differentiate to repair or replace the damaged tissue. This regenerative ability is essential for maintaining muscle function and mass throughout life, even in response to repeated or severe damage. However, the efficiency of muscle regeneration can decline with age, chronic disease, or prolonged disuse, highlighting the importance of understanding the underlying mechanisms to develop therapeutic strategies for muscle-related disorders.
| Characteristics | Values |
|---|---|
| Regeneration Capacity | High |
| Responsible Cells | Satellite Cells (muscle stem cells) |
| Regeneration Process | 1. Activation of satellite cells 2. Proliferation and differentiation into myoblasts 3. Fusion of myoblasts to form new muscle fibers or repair damaged fibers |
| Timeframe for Regeneration | 1-2 weeks for minor injuries; several weeks to months for severe injuries |
| Factors Affecting Regeneration | Age (declines with age), Nutrition, Hormones (e.g., growth hormone, testosterone), Physical Activity, and Immune Response |
| Limitations | Scar tissue formation in severe injuries, Reduced regenerative capacity in elderly or diseased individuals |
| Comparison to Other Tissues | Higher regenerative capacity than cardiac muscle or neurons, but lower than liver |
| Role of Extracellular Matrix | Provides structural support and signaling cues for regeneration |
| Role of Inflammation | Initial inflammatory response is necessary for clearing debris and activating satellite cells, but chronic inflammation can impair regeneration |
| Therapeutic Interventions | Physical therapy, stem cell therapy, growth factor administration, and gene therapy are being explored to enhance regeneration |
| Diseases Affecting Regeneration | Muscular dystrophies, cachexia, and sarcopenia can impair regenerative capacity |
Explore related products






What You'll Learn
![]()
Role of satellite cells in muscle regeneration
Skeletal muscle's remarkable ability to regenerate hinges on a specialized population of stem cells called satellite cells. Nestled beneath the basal lamina of muscle fibers, these quiescent cells spring into action upon injury, orchestrating a complex repair process.
Imagine a muscle fiber as a cable, and satellite cells as its repair crew. When the cable frays (muscle injury), these cells awaken, proliferate, and differentiate into myoblasts, the building blocks of new muscle tissue.
Activation and Proliferation: Upon injury, inflammatory signals and growth factors like hepatocyte growth factor (HGF) and fibroblast growth factor (FGF) rouse satellite cells from their dormant state. They begin to divide rapidly, expanding the pool of myoblasts available for repair. Think of this phase as the repair crew mobilizing and multiplying to tackle the damage.
Differentiation and Fusion: Myoblasts then undergo a metamorphosis, fusing with each other and with existing muscle fibers. This fusion process, akin to weaving new threads into a frayed cable, restores the structural integrity of the muscle. Myogenic regulatory factors (MRFs) like MyoD and myogenin act as the master weavers, guiding this intricate process.
Challenges and Considerations: While satellite cells are muscle's primary repair crew, their effectiveness can wane with age and certain conditions. Aging muscles exhibit a decline in satellite cell number and function, leading to slower and less complete regeneration. Additionally, diseases like muscular dystrophy can impair satellite cell activity, necessitating therapeutic interventions to boost their regenerative potential.
Harnessing Satellite Cell Power: Understanding satellite cell biology opens doors to potential therapies for muscle injuries and diseases. Strategies like satellite cell transplantation, gene therapy to enhance MRF expression, and stimulating satellite cell activation through exercise or pharmacological agents hold promise for improving muscle regeneration and restoring function.
Hot Tubs for Muscle Relief: Easing Tightness and Promoting Relaxation
You may want to see also
Explore related products






![]()
Impact of age on regenerative capacity
Skeletal muscle's regenerative prowess diminishes with age, a phenomenon linked to the decline in satellite cell function. These resident stem cells, nestled beneath the basal lamina, are pivotal for muscle repair. In youth, satellite cells swiftly activate, proliferate, and differentiate to mend damaged fibers. However, as individuals transition into their 60s and beyond, satellite cell numbers dwindle, and their responsiveness to injury signals wanes. This age-related impairment is exacerbated by systemic changes, such as reduced growth factor production and chronic low-grade inflammation, collectively termed "inflammaging." For instance, studies show that older adults exhibit a 30-50% reduction in muscle regeneration efficiency compared to their younger counterparts after injury or disuse.
To mitigate age-related regenerative decline, targeted interventions can be employed. Resistance training, particularly high-intensity protocols (e.g., 70-80% of one-rep max), stimulates satellite cell activation and enhances muscle protein synthesis in older adults. Incorporating 2-3 sessions weekly, focusing on compound movements like squats and deadlifts, can yield significant improvements within 8-12 weeks. Additionally, nutritional strategies, such as consuming 1.2-1.6 grams of protein per kilogram of body weight daily, support muscle repair. Supplementation with leucine (2.5-3.0 grams per dose) or HMB (3 grams daily) can further bolster protein synthesis in aging muscles.
A comparative analysis reveals that while young muscles recover within 2-3 weeks post-injury, older muscles may require 4-6 weeks or longer. This disparity underscores the importance of proactive measures. For example, older adults should prioritize gradual progression in exercise intensity to avoid overuse injuries, which can further compromise regenerative capacity. Moreover, managing comorbidities like diabetes or obesity is crucial, as these conditions accelerate muscle aging through mechanisms like oxidative stress and insulin resistance.
Descriptively, the aging muscle microenvironment becomes less conducive to regeneration. Extracellular matrix stiffening and fibrosis hinder satellite cell migration and differentiation. Concurrently, altered cytokine profiles, such as elevated TNF-α and IL-6, create a pro-inflammatory milieu that impairs repair. Practical tips include incorporating anti-inflammatory foods (e.g., fatty fish, turmeric) and staying hydrated to support cellular function. For those over 70, combining balance exercises with strength training reduces fall risk while promoting muscle health.
In conclusion, while skeletal muscle retains some regenerative capacity across the lifespan, age-induced changes necessitate tailored strategies. By understanding the interplay between satellite cell function, systemic factors, and environmental influences, individuals can optimize muscle repair and maintain functional independence as they age.
Potatoes and Muscle Recovery: Unlocking Post-Workout Nutrition Benefits
You may want to see also
Explore related products


$41.99 $44.99



![]()
Influence of inflammation on repair processes
Skeletal muscle's remarkable regenerative capacity hinges on a delicate interplay with inflammation, a double-edged sword in the repair process. While acute inflammation is essential for clearing debris and initiating repair, chronic or dysregulated inflammation can derail regeneration, leading to fibrosis and impaired function.
Consider the initial phase of muscle injury, where neutrophils and macrophages infiltrate the damaged site. These immune cells secrete pro-inflammatory cytokines like TNF-α and IL-6, which, in controlled amounts, stimulate satellite cell activation and proliferation. Satellite cells, resident stem cells nestled between the basal lamina and sarcolemma, are the primary drivers of muscle regeneration. However, excessive cytokine release can induce apoptosis in these cells, stifling repair. For instance, studies show that TNF-α concentrations above 10 ng/mL significantly reduce satellite cell viability in vitro, underscoring the importance of balanced inflammation.
Transitioning to the resolution phase, macrophages shift from a pro-inflammatory (M1) to an anti-inflammatory (M2) phenotype, promoting tissue repair and angiogenesis. M2 macrophages secrete growth factors like IGF-1 and TGF-β, which foster myoblast differentiation and fusion into myotubes. Yet, prolonged M1 dominance, often seen in conditions like muscular dystrophy or repetitive injuries, perpetuates tissue damage. Practical interventions, such as administering resolvins (e.g., 100 ng/kg of Resolvin D1) or limiting NSAID use during early repair stages, can tip the balance toward resolution, enhancing regeneration.
A comparative analysis reveals that age and systemic health significantly modulate inflammation’s impact. In younger individuals (under 30), robust immune responses typically support efficient repair, whereas older adults (over 60) often exhibit chronic low-grade inflammation (inflammaging), impairing satellite cell function. Similarly, conditions like diabetes or obesity exacerbate inflammatory responses, delaying muscle recovery. Tailored strategies, such as combining resistance training with anti-inflammatory diets rich in omega-3 fatty acids, can mitigate these effects, particularly in at-risk populations.
In conclusion, inflammation is both a catalyst and a potential saboteur of skeletal muscle regeneration. Mastering its modulation—through precise timing of interventions, lifestyle adjustments, and targeted therapies—holds the key to optimizing repair outcomes. Whether in clinical settings or athletic recovery, understanding this dynamic ensures that inflammation serves as an ally, not an adversary, in the regenerative process.
Plums and Muscle Growth: Unlocking the Fruit's Potential for Fitness
You may want to see also
Explore related products






![]()
Effects of exercise on muscle recovery
Skeletal muscle's remarkable regenerative capacity hinges on satellite cells, resident stem cells that activate in response to damage. Exercise, a potent stimulus for muscle adaptation, also plays a dual role in recovery by both inducing controlled damage and accelerating repair mechanisms. This paradoxical relationship underscores the importance of understanding how different exercise modalities influence muscle regeneration.
Consider resistance training, a cornerstone of muscle growth and repair. Studies show that moderate-intensity resistance exercise (60-80% of one-rep max) triggers satellite cell activation and proliferation, leading to increased muscle protein synthesis and hypertrophy. For instance, a 2018 study in the *Journal of Applied Physiology* found that young adults performing 3 sets of 8-12 repetitions of leg press exercises experienced a 25% increase in satellite cell activity within 24 hours post-workout. However, excessive volume or intensity can overwhelm the regenerative process, causing prolonged inflammation and delayed recovery. A practical guideline is to allow 48-72 hours of rest between intense resistance sessions for optimal muscle repair.
In contrast, aerobic exercise, such as running or cycling, primarily enhances mitochondrial density and capillary density, which indirectly support muscle recovery by improving nutrient and oxygen delivery. A 2017 study in *Medicine & Science in Sports & Exercise* demonstrated that 30 minutes of moderate-intensity aerobic exercise post-resistance training reduced muscle soreness by 30% in participants aged 20-40. This suggests that low-impact aerobic activity can serve as an active recovery tool, promoting blood flow without further damaging muscle fibers.
Aging introduces complexities, as satellite cell function declines with age, impairing muscle regeneration. For older adults (65+), combining resistance training with blood flow restriction (BFR) at 40-80% of arterial occlusion pressure has shown promise. A 2020 study in *Frontiers in Physiology* reported that BFR training increased muscle thickness by 15% in elderly participants, comparable to traditional high-load training but with lower joint stress. This highlights the need for tailored exercise strategies across age groups.
Finally, nutrition and hydration are critical adjuncts to exercise-induced recovery. Consuming 20-30 grams of high-quality protein (e.g., whey or casein) within 30 minutes post-exercise maximizes muscle protein synthesis. Adding 5-10 grams of branched-chain amino acids (BCAAs) can further enhance recovery, particularly after endurance exercises. Hydration, often overlooked, is essential; a 2% loss in body weight due to dehydration can impair muscle function and recovery. Practical tips include drinking 500 ml of water 2 hours before exercise and replenishing fluids at a rate of 150-200 ml every 15-20 minutes during prolonged activity.
In summary, exercise is a double-edged sword in muscle recovery, capable of both inducing damage and accelerating repair. By balancing intensity, modality, and recovery strategies, individuals can harness skeletal muscle’s regenerative potential to optimize healing and performance.
Are Protein Bars Effective for Building Lean Muscle? A Comprehensive Guide
You may want to see also
Explore related products






![]()
Role of growth factors in regeneration
Skeletal muscle's remarkable regenerative capacity hinges on a complex interplay of cellular and molecular mechanisms, with growth factors acting as key orchestrators. These signaling proteins, secreted by various cell types, regulate the proliferation, differentiation, and survival of muscle satellite cells—the resident stem cells responsible for muscle repair. Understanding the role of growth factors not only sheds light on muscle biology but also offers therapeutic avenues for enhancing regeneration in injury or disease.
Consider the example of hepatocyte growth factor (HGF), one of the earliest factors released after muscle injury. HGF activates the c-Met receptor on satellite cells, triggering their transition from quiescence to an active state. This initial step is critical, as it primes the cells for subsequent proliferation and differentiation. Studies in mice have shown that HGF administration accelerates muscle regeneration, with optimal doses ranging from 1 to 5 μg/kg body weight when delivered via intramuscular injection. However, timing is crucial; HGF’s effectiveness diminishes if administered beyond the first 24–48 hours post-injury, underscoring the need for precise intervention windows.
In contrast to HGF’s early role, insulin-like growth factor-1 (IGF-1) acts later in the regenerative process, promoting satellite cell differentiation and protein synthesis. IGF-1’s effects are particularly pronounced in aging muscle, where its levels naturally decline. Clinical trials have explored IGF-1 supplementation in older adults (ages 65+), demonstrating improved muscle mass and strength with systemic doses of 0.05–0.1 mg/kg/day. Yet, caution is warranted: prolonged IGF-1 exposure can lead to insulin resistance or tissue hypertrophy, highlighting the importance of balanced dosing and monitoring.
A comparative analysis of growth factors reveals their synergistic potential. For instance, combining HGF and fibroblast growth factor-2 (FGF-2) enhances satellite cell proliferation more effectively than either factor alone. FGF-2, known for its angiogenic properties, also promotes blood vessel formation, crucial for delivering nutrients to regenerating tissue. This combination approach has shown promise in preclinical models, particularly for volumetric muscle loss injuries, where single-factor therapies often fall short. However, translating these findings to humans requires careful consideration of delivery methods, such as localized hydrogel systems, to minimize off-target effects.
Practically, harnessing growth factors for muscle regeneration demands a tailored approach. For athletes recovering from strains, topical applications of HGF-infused patches could expedite healing, while older individuals might benefit from systemic IGF-1 therapy under medical supervision. Emerging technologies, like gene therapy to overexpress growth factors locally, offer exciting possibilities but remain experimental. Ultimately, the role of growth factors in muscle regeneration is not just theoretical—it’s a blueprint for innovative therapies, provided we navigate their complexities with precision and caution.
Top Websites for Buying Muscle Cars: A Comprehensive Guide
You may want to see also
Frequently asked questions
Yes, skeletal muscle has a remarkable capacity for regeneration due to the presence of satellite cells, which are muscle-specific stem cells that activate and differentiate to repair damaged muscle fibers.
Factors such as age, nutrition, overall health, and the extent of injury can impact skeletal muscle regeneration. Older individuals or those with poor nutrition may experience slower or less effective regeneration.
While skeletal muscle can regenerate effectively in many cases, severe injuries, repeated damage, or certain diseases (e.g., muscular dystrophy) may overwhelm its regenerative capacity, leading to incomplete recovery or scarring.































