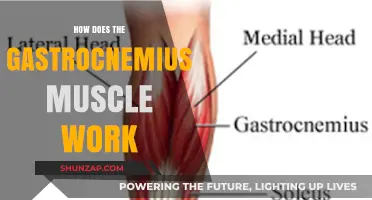
The ryanodine receptor (RyR) is a crucial calcium release channel in skeletal muscle, playing a central role in muscle contraction through a process known as excitation-contraction (EC) coupling. Located on the sarcoplasmic reticulum (SR), RyR is activated by mechanical interaction with the dihydropyridine receptor (DHPR), a voltage-gated calcium channel on the transverse tubule (T-tubule) membrane, following depolarization of the muscle fiber. When an action potential reaches the muscle fiber, it triggers the opening of DHPRs, which physically couple with RyRs, causing them to open and release calcium ions (Ca²⁺) from the SR into the cytoplasm. This rapid increase in cytosolic calcium binds to troponin C on the thin filaments, enabling myosin heads to interact with actin and initiate muscle contraction. After contraction, calcium is actively pumped back into the SR by the sarco/endoplasmic reticulum Ca²⁺ ATPase (SERCA), lowering cytosolic calcium levels and allowing muscle relaxation. Dysfunction of RyR, often due to mutations or oxidative stress, can lead to disorders such as malignant hyperthermia or central core disease, highlighting its critical role in muscle physiology.
| Characteristics | Values |
|---|---|
| Function | Calcium release channel in the sarcoplasmic reticulum (SR) of skeletal muscle fibers. |
| Activation Mechanism | Activated by mechanical coupling with dihydropyridine receptors (DHPRs) via conformational changes during muscle depolarization. |
| Calcium Release Process | Releases calcium ions (Ca²⁺) from the SR into the cytoplasm, triggering muscle contraction via interaction with troponin-C. |
| Structure | Homotetrameric protein complex with a large cytoplasmic "foot" structure and a pore-forming region. |
| Subunit Composition | Composed of RyR1 isoform (specific to skeletal muscle), along with auxiliary proteins like FKBP12 and calmodulin. |
| Regulation | Regulated by luminal Ca²⁺ concentration, ATP, caffeine, and ryanodine (binds to modulate activity). |
| Inhibition | Inhibited by high luminal Ca²⁺ levels, Mg²⁺, and low pH; ryanodine at high concentrations blocks the channel. |
| Role in Excitation-Contraction Coupling | Essential for converting electrical signals (action potentials) into mechanical responses (muscle contraction). |
| Pathological Relevance | Mutations in RyR1 are linked to malignant hyperthermia, central core disease, and other skeletal muscle disorders. |
| Pharmacological Modulation | Sensitive to drugs like caffeine (activator) and dantrolene (inhibitor), used in treating muscle disorders. |
| Energy Dependence | Requires ATP for proper function; ATP depletion impairs calcium release. |
| Localization | Located on the SR membrane, juxtaposed to T-tubules where DHPRs are present. |
Explore related products

$108.39 $169.99





What You'll Learn
- Ryanodine receptor structure and function in muscle calcium release
- Activation mechanisms: mechanical and chemical signaling pathways
- Role in excitation-contraction coupling process in muscle fibers
- Regulation by accessory proteins and post-translational modifications
- Dysfunction and its link to muscular diseases and disorders
![]()
Ryanodine receptor structure and function in muscle calcium release
The ryanodine receptor (RyR) is a calcium release channel embedded in the sarcoplasmic reticulum (SR) of skeletal muscle cells, playing a pivotal role in muscle contraction. Its structure is complex, consisting of four identical subunits, each containing a cytoplasmic domain that interacts with other proteins and a transmembrane domain that forms the calcium-conducting pore. This tetrameric assembly ensures precise regulation of calcium flux, which is essential for the rapid and coordinated release of calcium ions during muscle activation.
Consider the process of excitation-contraction coupling: when an action potential reaches the muscle fiber, it triggers the opening of voltage-gated L-type calcium channels (dihydropyridine receptors, DHPRs) on the sarcolemma. This influx of calcium acts as a signal, causing the DHPRs to mechanically couple with the RyRs, leading to their activation. The RyR’s cytoplasmic domain contains binding sites for various modulators, including calcium, ATP, and caffeine, which fine-tune its activity. For instance, caffeine at doses as low as 5–10 mg/kg can sensitize RyRs, increasing calcium release and potentially causing muscle spasms or weakness in susceptible individuals.
A critical aspect of RyR function is its regulation by accessory proteins. The FK506 binding protein (FKBP12) stabilizes the closed state of the RyR, preventing spontaneous calcium leaks. In certain genetic disorders, such as malignant hyperthermia or central core disease, mutations in the RyR gene disrupt this interaction, leading to uncontrolled calcium release and muscle dysfunction. For example, individuals with RyR1 mutations may experience episodes of hyperthermia and rigidity during anesthesia, requiring careful management with dantrolene (1–2.5 mg/kg) to inhibit calcium release and prevent complications.
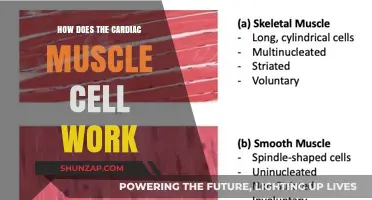
Comparing RyR function across muscle types highlights its adaptability. In skeletal muscle, RyR1 isoforms are activated by mechanical coupling with DHPRs, ensuring rapid calcium release for forceful contractions. In contrast, cardiac muscle relies on RyR2 isoforms, which are primarily activated by calcium-induced calcium release (CICR), allowing for rhythmic, sustained contractions. This distinction underscores the importance of RyR structure and localization in tailoring calcium signaling to specific physiological demands.
To optimize muscle performance and prevent RyR-related disorders, practical strategies include maintaining adequate magnesium levels (300–400 mg/day for adults), as magnesium acts as a natural calcium channel blocker, stabilizing RyR function. Additionally, avoiding excessive caffeine intake and monitoring anesthetic risks in susceptible individuals can mitigate the risk of RyR dysfunction. Understanding the intricate structure and function of the ryanodine receptor provides actionable insights into both muscle physiology and pathology, offering targeted interventions for improved health outcomes.
V-Sit Workout: Targeting Core Muscles for Strength and Stability
You may want to see also
Explore related products






![]()
Activation mechanisms: mechanical and chemical signaling pathways
The ryanodine receptor (RyR) in skeletal muscle is a calcium release channel that plays a pivotal role in muscle contraction. Its activation is a finely tuned process involving both mechanical and chemical signaling pathways, ensuring rapid and coordinated muscle responses. Understanding these mechanisms sheds light on the intricate interplay between physical forces and biochemical signals in muscle physiology.
Mechanical signaling pathways are initiated by muscle stretching or deformation. When a muscle is stretched, the sarcolemma and transverse tubules (T-tubules) experience mechanical stress, which is transmitted to the RyR via accessory proteins like the dihydropyridine receptor (DHPR). This mechanical force induces conformational changes in the RyR, increasing its sensitivity to calcium ions. For instance, in fast-twitch muscle fibers, even subtle stretches can enhance RyR activity, allowing for quicker calcium release and contraction. Practical applications of this mechanism are seen in athletic training, where dynamic stretching routines leverage mechanical signaling to improve muscle responsiveness. Athletes aged 18–35 can benefit from incorporating 10–15 minutes of dynamic stretches pre-workout to optimize RyR activation.
Chemical signaling pathways, on the other hand, rely on the binding of specific ligands or second messengers to the RyR. The primary activator is calcium itself, creating a positive feedback loop. When a small amount of calcium enters the cell through voltage-gated DHPRs, it binds to the RyR, triggering a larger release of calcium from the sarcoplasmic reticulum (SR). This process, known as calcium-induced calcium release (CICR), is essential for generating the high calcium concentrations needed for muscle contraction. Additionally, caffeine and certain drugs like 4-chloro-m-cresol can directly activate RyR by mimicking calcium binding, though their effects are dose-dependent. For example, a 5 mg/kg dose of caffeine in adults can enhance RyR activity, but excessive intake (>400 mg/day) may lead to desensitization and impaired muscle function.
Comparing these pathways reveals their complementary roles. Mechanical signaling acts as a rapid, force-dependent trigger, ideal for sudden movements or stretches, while chemical signaling provides sustained activation, crucial for prolonged contractions. Dysregulation in either pathway can lead to disorders like malignant hyperthermia or central core disease, underscoring their importance. For instance, mutations in the RyR1 gene that impair mechanical sensitivity are linked to exercise-induced rhabdomyolysis in young adults. Genetic testing and tailored exercise regimens can mitigate risks in susceptible individuals.
In practical terms, optimizing RyR activation involves balancing both pathways. Resistance training, particularly eccentric exercises, enhances mechanical signaling by improving muscle fiber resilience. Similarly, maintaining adequate calcium and magnesium levels through diet (e.g., 1000–1300 mg calcium daily for adults) supports chemical signaling. Caution should be exercised with RyR-modulating substances like statins or alcohol, which can interfere with receptor function. By understanding and harnessing these activation mechanisms, individuals can improve muscle performance and prevent related disorders.
Incline Dumbbell Press: Target Muscles and Benefits Explained
You may want to see also
Explore related products


$145.24 $219.99




![]()
Role in excitation-contraction coupling process in muscle fibers
The ryanodine receptor (RyR) is a calcium release channel embedded in the sarcoplasmic reticulum (SR) of skeletal muscle fibers, playing a pivotal role in the excitation-contraction (EC) coupling process. When an action potential reaches the muscle fiber, it triggers the opening of voltage-gated L-type calcium channels (dihydropyridine receptors, DHPRs) in the transverse tubule (T-tubule) membrane. This influx of a small amount of calcium ions acts as a signal, causing the RyR to open and release a large amount of calcium from the SR into the cytoplasm. This rapid increase in cytoplasmic calcium concentration binds to troponin, initiating the sliding filament mechanism and muscle contraction.
Consider the sequence of events as a finely tuned relay race. The action potential is the starting gun, the DHPRs are the first runners passing the baton (calcium ions) to the RyRs, which then unleash the main event—calcium release. This amplification step is critical; a single calcium ion entering through the DHPR triggers the release of approximately 50 calcium ions from the SR, ensuring a robust and coordinated contraction. Without this mechanism, muscle fibers would lack the sensitivity and strength required for even simple movements.
From a practical standpoint, understanding RyR function is essential in diagnosing and treating muscle disorders. For instance, mutations in the RyR1 gene can lead to malignant hyperthermia, a life-threatening condition triggered by certain anesthetics. Patients with this condition require careful management during surgery, avoiding triggers like volatile anesthetics and succinylcholine. Additionally, RyR dysfunction is implicated in central core disease and other muscular dystrophies, highlighting the receptor’s central role in muscle health. Regular genetic screening for at-risk individuals, particularly children and young adults, can prevent catastrophic outcomes.
Comparatively, the RyR’s role in skeletal muscle contrasts with its function in cardiac muscle, where calcium-induced calcium release (CICR) is the primary mechanism. In skeletal muscle, the physical coupling between DHPRs and RyRs ensures precise control, whereas cardiac muscle relies more on CICR for rhythmic contractions. This distinction underscores the adaptability of calcium signaling across tissues. For athletes or fitness enthusiasts, optimizing RyR function through adequate magnesium intake (300–400 mg/day) and maintaining electrolyte balance can enhance muscle performance and reduce cramping, as magnesium stabilizes the RyR in its closed state, preventing spontaneous calcium leaks.
In summary, the RyR is not merely a calcium channel but a master regulator of muscle contraction, translating electrical signals into mechanical action. Its role in EC coupling is both delicate and powerful, requiring precise coordination to ensure muscle function. Whether in clinical settings or athletic performance, appreciating the RyR’s mechanics provides actionable insights for prevention, treatment, and optimization of muscle health.
Squats: Targeting Quads, Glutes, Hamstrings, and Core Muscles Effectively
You may want to see also
Explore related products

$7.32 $13.99
$11.99 $21.69




![]()
Regulation by accessory proteins and post-translational modifications
The ryanodine receptor (RyR) in skeletal muscle is a complex molecular machine whose activity is finely tuned by accessory proteins and post-translational modifications (PTMs). These regulatory mechanisms ensure that calcium release is precisely controlled, matching the demands of muscle contraction. Among the key accessory proteins, FKBP12 (also known as calstabin) stabilizes the RyR in its closed state, preventing spontaneous calcium leaks. When FKBP12 dissociates from RyR, as seen in certain disease states or under stress, the receptor becomes hyperactive, leading to pathological calcium release. This interaction underscores the critical role of accessory proteins in maintaining RyR function.
Post-translational modifications further refine RyR activity by altering its conformation or interaction with other proteins. Phosphorylation, for instance, is a well-studied PTM that modulates RyR sensitivity to calcium and activators like caffeine. Studies show that phosphorylation at specific sites, such as Ser-2843 by PKA, enhances RyR activity, while dephosphorylation by protein phosphatases like PP1 reverses this effect. This dynamic regulation allows the RyR to respond rapidly to physiological signals, such as adrenergic stimulation during exercise. Understanding these phosphorylation events is crucial for developing targeted therapies for conditions like malignant hyperthermia, where RyR hyperactivity is a hallmark.
Another layer of regulation involves oxidative modifications, particularly nitrosylation and S-glutathionylation, which can impair RyR function. Oxidative stress, common in aging or muscular dystrophies, leads to aberrant PTMs that disrupt RyR’s calcium handling. For example, nitrosylation of RyR cysteine residues reduces its affinity for FKBP12, destabilizing the channel. Conversely, S-glutathionylation can protect RyR from excessive oxidation, highlighting the dual role of PTMs in both dysfunction and protection. Practical strategies to mitigate oxidative damage, such as antioxidant supplementation (e.g., vitamin E at 400–800 IU/day for adults) or exercise regimens tailored to reduce oxidative stress, may help preserve RyR function in at-risk populations.
Comparatively, the interplay between accessory proteins and PTMs reveals a sophisticated regulatory network. While accessory proteins like FKBP12 provide structural stability, PTMs offer dynamic control, allowing the RyR to adapt to changing cellular conditions. For instance, during prolonged exercise, increased phosphorylation enhances calcium release to meet energy demands, while simultaneous protection by S-glutathionylation prevents oxidative damage. This dual regulation exemplifies the RyR’s ability to balance responsiveness and resilience. By targeting these mechanisms, researchers can develop interventions that either enhance muscle performance or alleviate RyR-related disorders, such as using FKBP12 stabilizers for treating cardiac arrhythmias.
In conclusion, the regulation of RyR by accessory proteins and post-translational modifications is a multifaceted process that ensures precise calcium signaling in skeletal muscle. From the stabilizing role of FKBP12 to the dynamic effects of phosphorylation and oxidative PTMs, these mechanisms collectively govern RyR activity. Practical applications, such as antioxidant therapies or exercise protocols, can leverage this knowledge to improve muscle health and treat diseases. By dissecting these regulatory pathways, scientists can unlock new strategies for optimizing muscle function across diverse age groups and physiological states.
Strengthen Your Vision: Effective Eye Muscle Workouts for Better Focus
You may want to see also
Explore related products


$9.59 $11.99


![]()
Dysfunction and its link to muscular diseases and disorders
The ryanodine receptor (RyR) is a calcium release channel crucial for muscle contraction, but its dysfunction can lead to a cascade of muscular disorders. When RyR malfunctions, calcium homeostasis is disrupted, impairing muscle function and leading to conditions like malignant hyperthermia (MH) and central core disease (CCD). MH, a life-threatening reaction to certain anesthetics, is often linked to RyR1 mutations that cause excessive calcium release, triggering hypermetabolism and muscle rigidity. Patients with a family history of MH should undergo genetic testing to identify RyR1 mutations and avoid triggering agents like succinylcholine and volatile anesthetics. Early recognition and treatment with dantrolene sodium, a RyR stabilizer, are critical to managing MH episodes.
In contrast to MH, central core disease (CCD) is a congenital myopathy characterized by muscle weakness and central cores on muscle biopsy, often caused by dominant RyR1 mutations. These mutations reduce calcium release, impairing excitation-contraction coupling and leading to chronic muscle dysfunction. Children with CCD may present with delayed motor milestones, hypotonia, and mild to moderate weakness, particularly in the facial and proximal limb muscles. Physical therapy and occupational therapy can help manage symptoms, but there is no cure. Families should be counseled on the autosomal dominant inheritance pattern, as even mild mutations can cause significant disease in offspring.
RyR dysfunction also plays a role in age-related muscle decline, known as sarcopenia. With aging, RyR becomes leaky, causing intracellular calcium elevations that activate proteases and impair muscle repair. Studies show that in individuals over 65, RyR leakiness correlates with reduced muscle mass and strength. Interventions like resistance training and calcium-regulating supplements (e.g., vitamin D and magnesium) may mitigate these effects. Additionally, emerging therapies targeting RyR stabilization, such as S107, show promise in preclinical models of sarcopenia, though clinical trials are ongoing.
Comparatively, RyR dysfunction in muscular dystrophies like Duchenne muscular dystrophy (DMD) exacerbates disease progression. In DMD, dystrophin deficiency leads to sarcolemmal instability, which in turn causes RyR mislocalization and calcium mishandling. This creates a vicious cycle of muscle damage and inflammation. Early intervention with corticosteroids remains the standard of care, but novel approaches like gene therapy (e.g., micro-dystrophin) and RyR modulators are being explored. For instance, the RyR stabilizer ARM210 has shown potential in reducing muscle damage in DMD mouse models, highlighting the receptor’s therapeutic relevance.
Finally, understanding RyR dysfunction offers practical insights for prevention and management. For instance, individuals with RyR mutations should avoid strenuous exercise in hot environments, as heat stress can exacerbate calcium dysregulation. Hydration and gradual acclimatization are essential for those at risk. In clinical settings, anesthesiologists must screen for MH susceptibility before surgery, particularly in pediatric and young adult populations. Advances in genetic testing and targeted therapies provide hope for personalized treatment strategies, emphasizing the need for continued research into RyR’s role in muscular health and disease.
Effective Remedies for Muscle Soreness After Intense Workouts
You may want to see also
Frequently asked questions
The ryanodine receptor (RyR) is a calcium release channel located on the sarcoplasmic reticulum (SR) membrane in skeletal muscle cells. It plays a critical role in muscle contraction by releasing stored calcium ions into the cytoplasm.
The RyR is activated by mechanical coupling with the dihydropyridine receptor (DHPR), a voltage-sensitive calcium channel on the T-tubule membrane. When an action potential depolarizes the T-tubule, the DHPR undergoes a conformational change, which physically triggers the opening of the RyR.
Calcium ions released from the RyR bind to troponin on the actin filaments, causing a conformational change that exposes myosin-binding sites. This allows myosin heads to interact with actin, initiating the sliding filament mechanism and resulting in muscle contraction.
The RyR is regulated by various factors, including calcium concentration, magnesium, ATP, and accessory proteins like FKBP12. Dysregulation of RyR, such as mutations or improper calcium handling, can lead to disorders like malignant hyperthermia or central core disease.
Ryanodine is a plant alkaloid that binds to the RyR, initially activating it at low concentrations and blocking it at higher concentrations. This property has been instrumental in studying the receptor's function and mechanisms in calcium signaling and muscle physiology.