Diagnosing hip muscle pain involves a systematic approach to identify the underlying cause, which can range from overuse injuries and muscle strains to more serious conditions like arthritis or labral tears. The process typically begins with a thorough medical history, including details about the onset, duration, and nature of the pain, as well as any recent physical activities or injuries. A physical examination follows, where a healthcare provider assesses range of motion, strength, and tenderness in the hip area, often using specific tests like the FABER test or the impingement test to pinpoint the source of discomfort. Imaging studies such as X-rays, MRIs, or ultrasounds may be ordered to rule out structural issues, while additional diagnostic tools like blood tests can help identify inflammatory conditions. Accurate diagnosis is crucial for developing an effective treatment plan, which may include rest, physical therapy, medication, or, in severe cases, surgical intervention.
Hip Muscle Pain Diagnosis Characteristics
| Characteristics | Values |
|---|---|
| Location of Pain | Groin, buttock, outer hip, front of thigh, radiating down the leg |
| Pain Type | Dull ache, sharp pain, burning sensation, stiffness |
| Aggravating Factors | Walking, running, climbing stairs, sitting for long periods, rotating hip, getting up from a seated position |
| Relieving Factors | Rest, ice, heat, stretching, anti-inflammatory medications |
| Range of Motion | Limited hip flexion, extension, abduction, adduction, internal/external rotation |
| Tenderness | Pain upon palpation of specific muscles (e.g., gluteus medius, piriformis, iliopsoas) |
| Strength Testing | Weakness in hip abductors, adductors, flexors, or extensors |
| Special Tests | FABER test, Patrick's test, Trendelenburg test, Ober's test (depending on suspected muscle involvement) |
| Imaging | X-ray (to rule out fractures or arthritis), MRI (for soft tissue injuries), Ultrasound (for tendon or muscle tears) |
| Medical History | Recent injury, overuse, previous hip problems, underlying conditions (e.g., arthritis, bursitis) |
Explore related products



$15.99 $19.99



What You'll Learn
- Identify Pain Location: Pinpoint where hip pain originates: front, side, back, or groin area
- Assess Movement Limitations: Evaluate difficulty in walking, bending, or rotating the hip joint
- Check for Tenderness: Palpate hip muscles to detect specific areas of sensitivity or pain
- Rule Out Referral Pain: Determine if pain is from hip muscles or radiating from lower back
- Use Diagnostic Tests: Apply tests like FABER or impingement tests to isolate muscle issues
![]()
Identify Pain Location: Pinpoint where hip pain originates: front, side, back, or groin area
Hip pain is not a one-size-fits-all complaint. It’s a symptom with a geography, and understanding its location is the first step in decoding its cause. Pain in the front of the hip often points to issues with the hip joint itself, such as osteoarthritis or labral tears, especially in adults over 50 or athletes. Side hip pain, typically felt over the greater trochanter, usually indicates inflammation of the tendons or bursae, a condition exacerbated by repetitive activities like running or climbing stairs. Pain in the back of the hip, less common but equally important, may suggest problems with the sacroiliac joint or piriformis muscle, often aggravated by prolonged sitting or improper lifting. Groin pain, meanwhile, frequently implicates the adductor muscles or hip flexors, common in sports requiring sudden changes in direction, like soccer or hockey.
To pinpoint the source, start by palpating the area gently. For front hip pain, press around the inguinal crease and anterior joint line. Side pain warrants pressure on the greater trochanter and surrounding bursae. For back hip pain, focus on the sacroiliac joint and gluteal region. Groin pain requires careful examination of the adductor tendons and pubic symphysis. Note any tenderness, swelling, or warmth, as these can guide further investigation. For instance, sharp pain in the groin with resistance against hip adduction suggests an adductor strain, while tenderness over the greater trochanter with lateral hip pressure indicates trochanteric bursitis.
A comparative approach can also clarify the diagnosis. Ask the patient to describe the pain’s quality: is it sharp, dull, throbbing, or radiating? Front hip pain often feels deep and aching, while side pain tends to be more superficial and worsens with pressure. Groin pain may be sharp and worsen with hip flexion or rotation. Back hip pain can feel dull and diffuse, sometimes mimicking lower back discomfort. For example, a 35-year-old runner with sharp, localized side hip pain after increasing mileage likely has bursitis, whereas a 60-year-old with dull, aching front hip pain climbing stairs may have early osteoarthritis.
Practical tips can aid in self-assessment. Use a mirror or smartphone camera to observe gait and posture, as asymmetry or limping can highlight the affected area. Test specific movements: pain with hip flexion (e.g., lifting the knee) suggests hip flexor strain, while pain with internal rotation points to groin or adductor issues. For side hip pain, lie on the unaffected side and press on the greater trochanter—if it reproduces pain, bursitis is likely. Always avoid aggravating activities during assessment, and apply ice to the area if swelling or warmth is present.
In conclusion, identifying the precise location of hip pain is both an art and a science. It requires a systematic approach, combining palpation, movement testing, and comparative analysis. By narrowing down the pain’s geography, you can significantly reduce the diagnostic possibilities, paving the way for targeted treatment. Whether it’s front, side, back, or groin, each location tells a story—one that, when deciphered, can lead to relief and recovery.
Understanding the Permanent and Painful Shortening of Muscles: Causes and Impact
You may want to see also
Explore related products






![]()
Assess Movement Limitations: Evaluate difficulty in walking, bending, or rotating the hip joint
Difficulty walking, bending, or rotating the hip joint is often the first red flag signaling hip muscle pain. These limitations aren’t just inconveniences—they’re your body’s way of communicating that something is wrong. For instance, a sharp pain when pivoting during a walk or an inability to bend down to tie your shoes can point directly to strained or inflamed hip muscles, such as the iliopsoas or gluteal group. Observing these specific movement restrictions helps narrow down the root cause, whether it’s overuse, injury, or underlying conditions like bursitis.
To systematically assess movement limitations, start by evaluating gait patterns. Does the individual limp, favor one side, or struggle with balance? A noticeable asymmetry in walking, like a reduced stride length or an uneven rhythm, often indicates hip abductor or adductor weakness. Next, test bending capabilities. Ask the person to perform a simple forward fold or squat. Difficulty in these actions, especially if accompanied by pain or stiffness, suggests tightness in the hip flexors or hamstrings. For rotation, observe how easily they can turn their leg inward or outward while seated or standing. Limited internal or external rotation may implicate issues with the hip rotator cuff muscles or joint capsule.
Practical tips for accurate assessment include using a mirror or video recording to observe movement objectively. Encourage the individual to move slowly and mindfully, noting where discomfort begins. For older adults or those with chronic conditions, modify tests to avoid strain—for example, assess bending by having them slide down a wall instead of attempting a full squat. In younger, active individuals, compare movement limitations to their baseline mobility to identify deviations. Always document the range of motion in degrees or descriptive terms (e.g., "50% of normal rotation") for consistency.
Cautions are critical when evaluating movement limitations. Avoid forcing any motion that causes sharp or worsening pain, as this can exacerbate injuries. Be mindful of comorbidities like arthritis or previous surgeries, which may skew results. For instance, a hip replacement patient might naturally have reduced rotation due to prosthetic design, not muscle pain. If limitations persist or are severe, refer to a physical therapist or orthopedic specialist for further evaluation, such as imaging or strength testing.
In conclusion, assessing movement limitations is a dynamic process that combines observation, testing, and context. By focusing on walking, bending, and rotating the hip joint, you can pinpoint muscle-related issues with precision. This approach not only aids in diagnosis but also informs tailored treatment plans, whether it’s stretching tight hip flexors, strengthening weak abductors, or addressing underlying conditions. Master this assessment, and you’ll transform vague complaints of hip pain into actionable insights.
Bone and Muscle Pain: A Potential Symptom of Lymphoma?
You may want to see also
Explore related products






![]()
Check for Tenderness: Palpate hip muscles to detect specific areas of sensitivity or pain
Palpation, the act of pressing on the body to feel for abnormalities, is a cornerstone of diagnosing hip muscle pain. By systematically applying pressure to specific hip muscles, you can pinpoint areas of tenderness, a key indicator of injury or strain. This technique allows you to differentiate between generalized soreness and localized pain, guiding further diagnostic steps.
Imagine a map of the hip, with muscles like the gluteus medius, piriformis, and iliopsoas as landmarks. Palpation is your compass, helping you navigate this terrain to identify the source of discomfort.
Begin with the patient in a comfortable position, ideally lying down. Use your fingertips or the palm of your hand to apply gentle, gradual pressure to the suspected muscle groups. Start with light pressure, gradually increasing until you reach a point of resistance or the patient reports discomfort. Important: Always communicate with the patient throughout the process, asking them to rate the pain on a scale of 1 to 10 and to describe the sensation (sharp, dull, burning, etc.). This qualitative feedback is crucial for accurate assessment.
Be mindful of the patient's pain threshold and adjust your pressure accordingly. Avoid causing unnecessary discomfort, as this can lead to guarding, making it difficult to accurately assess tenderness. Remember, the goal is to identify specific areas of sensitivity, not to exacerbate the pain.
For example, when palpating the piriformis muscle, located deep in the buttock, use a deeper, more focused pressure. This muscle is often implicated in sciatica-like pain, and tenderness here can be a telltale sign.
Palpation is a skill that improves with practice. Familiarize yourself with the anatomical landmarks of the hip and the specific locations of key muscles. Visual aids, such as anatomical charts or 3D models, can be invaluable tools for learning and reference. By mastering this technique, you'll become adept at deciphering the body's signals, leading to more accurate diagnoses and targeted treatment plans for hip muscle pain.
Effective Remedies for Muscle Pain: Relief Strategies That Actually Work
You may want to see also
Explore related products






![]()
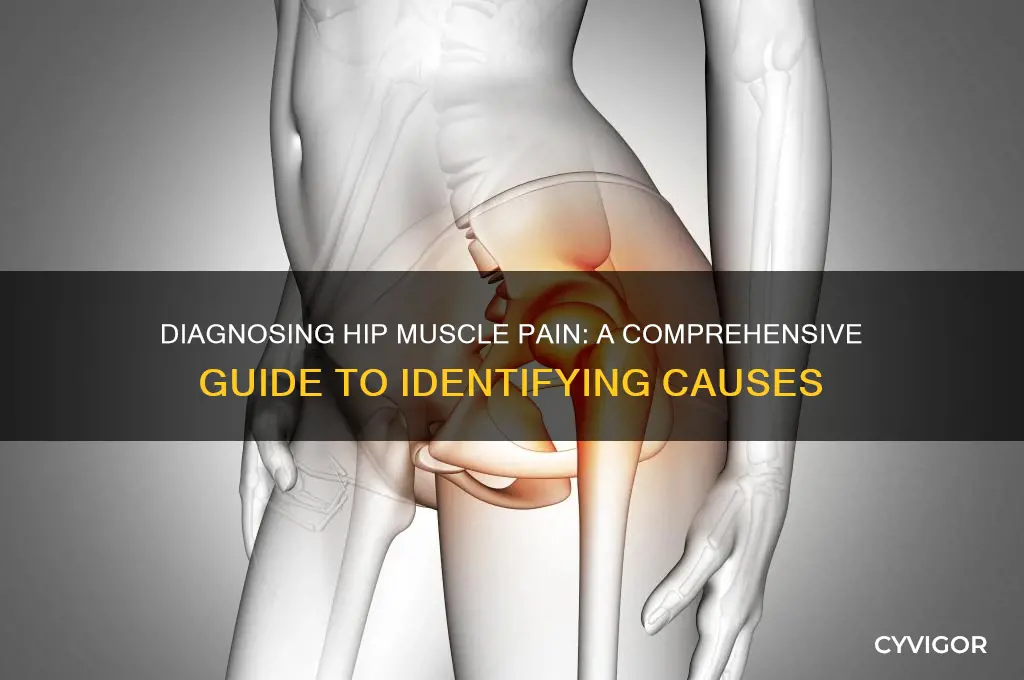
Rule Out Referral Pain: Determine if pain is from hip muscles or radiating from lower back
Hip pain can be deceptive. What feels like a deep ache in your hip might actually originate from your lower back, a phenomenon known as referred pain. This occurs when nerve pathways overlap, causing pain to be felt in a location different from its source. For instance, a herniated disc in the lumbar spine can send pain signals down the sciatic nerve, manifesting as hip discomfort. Recognizing this distinction is crucial, as treating the hip alone may provide temporary relief but fail to address the root cause.
To differentiate between hip muscle pain and referred pain from the lower back, start by assessing the pain’s characteristics. Hip muscle pain typically worsens with specific movements, such as climbing stairs or rotating the leg outward, and is often localized to the groin, outer hip, or buttocks. In contrast, referred pain from the lower back may radiate along a predictable pathway, like down the back of the thigh, and is frequently accompanied by symptoms like numbness, tingling, or weakness. A simple test: if bending or twisting your spine exacerbates the pain, the source is likely your lower back, not your hip muscles.
Next, consider your medical history and lifestyle. Prolonged sitting, heavy lifting, or repetitive motions can strain the lower back, increasing the likelihood of referred pain. Similarly, conditions like osteoarthritis or tendinitis are more commonly associated with hip muscle pain. For older adults (ages 50+), degenerative changes in the spine or hips may complicate diagnosis, making a thorough evaluation essential. Younger individuals (ages 20–40) should examine recent physical activities or injuries that could have triggered the pain.
Practical steps can help clarify the origin. Try the straight leg raise test: lie flat on your back, keep one leg straight, and slowly lift it. If pain radiates down your leg or into your hip before your leg reaches 30–70 degrees, it suggests nerve involvement, often linked to the lower back. For hip muscle pain, the Faber test is useful: sit on a table with one leg crossed over the other, then gently press down on the bent knee. Pain in the hip or groin indicates local muscle or joint issues. Always perform these tests gently to avoid aggravating the condition.
In conclusion, ruling out referral pain requires a combination of symptom analysis, history evaluation, and targeted tests. Misdiagnosis can lead to ineffective treatment, such as unnecessary physical therapy for the hip when the lower back is the true culprit. If uncertainty persists, consult a healthcare professional for imaging studies like X-rays or MRIs to pinpoint the source. Addressing the correct cause ensures a more accurate and lasting solution to your pain.
Effective Strategies to Relieve Kratom Withdrawal Muscle Pain
You may want to see also
Explore related products






![]()
Use Diagnostic Tests: Apply tests like FABER or impingement tests to isolate muscle issues
Hip pain can stem from various sources, but isolating muscle issues requires precision. Diagnostic tests like the FABER (Flexion, Abduction, External Rotation) test and impingement tests are invaluable tools for clinicians. These maneuvers systematically stress specific structures, revealing patterns of discomfort or restriction that point to muscle strain, imbalance, or referred pain. For instance, a positive FABER test—where pain occurs during hip flexion, abduction, and external rotation—often indicates pathology in the hip joint or surrounding musculature, such as the piriformis or gluteal muscles.
Performing these tests correctly is crucial for accurate diagnosis. The FABER test, for example, involves positioning the patient supine, then flexing one hip to 90 degrees, abducting the leg, and externally rotating the hip. The clinician observes for pain, asymmetry, or resistance, which may suggest muscle tightness, inflammation, or joint dysfunction. Impingement tests, like the FADIR (Flexion, Adduction, Internal Rotation) test, are similarly structured but target different movements to identify labral tears or femoroacetabular impingement. These tests are not standalone solutions but part of a comprehensive assessment that includes patient history and imaging when necessary.
While these diagnostic tests are effective, they require careful interpretation. False positives can occur if the patient has generalized stiffness or if the examiner applies excessive force. For example, elderly patients or those with arthritis may exhibit pain during FABER due to joint degeneration rather than muscle issues. Clinicians must correlate test results with other findings, such as localized tenderness upon palpation or specific activity-related pain patterns. Additionally, patient positioning and relaxation are critical; tension in the lower back or hamstrings can skew results, so ensuring comfort and proper alignment is essential.
In practice, these tests serve as a bridge between subjective complaints and objective findings. A 30-year-old runner with lateral hip pain, for instance, might show positive FABER and impingement test results, suggesting gluteus medius strain or labral irritation. Conversely, a sedentary individual with similar pain may exhibit negative results, pointing to non-muscular causes like bursitis. By systematically applying these tests, clinicians can tailor treatment plans—whether stretching, strengthening, or referral for imaging—with greater confidence and precision. Mastery of these techniques transforms diagnosis from guesswork into a science, ensuring patients receive targeted care for their hip muscle pain.
Managing Anxiety-Induced Muscle Pain: Effective Strategies for Relief and Relaxation
You may want to see also
Frequently asked questions
Hip muscle pain can result from overuse, injury, muscle strain, tendonitis, bursitis, arthritis, or underlying conditions like sciatica or hip labral tears.
Muscle pain typically feels achy or sore and worsens with movement, while joint pain is often sharp, stiff, and may be accompanied by swelling or reduced range of motion.
Perform gentle stretches or movements to identify specific areas of discomfort. Note if pain worsens with activity, improves with rest, or is accompanied by symptoms like numbness or weakness.
Consult a doctor if pain persists for more than a week, is severe, or is accompanied by fever, swelling, redness, or inability to bear weight on the affected leg.
Doctors may use physical exams, X-rays, MRI, ultrasound, or blood tests to rule out underlying conditions and determine the exact cause of the pain.