The hyoid bone is a small, U-shaped bone located in the midline of the neck, at the base of the mandible. It is considered an unconventional bone as it is not interconnected with any adjacent bones. However, it is closely linked with an extended tendon-muscular complex and serves as an anchor for the suprahyoid and infrahyoid muscles. To palpate the hyoid bone, a clinician must first ask the patient to gently tuck their chin. Then, the clinician gently places their fingertips on the superior surface of the hyoid bone and asks the patient to swallow, feeling for the hyoid's movement. This procedure is important for diagnosing hyoid-related issues such as hyoid bone insertion tendinitis, which causes neck pain, particularly when swallowing.
| Characteristics | Values |
|---|---|
| Position of the patient | Sitting, standing, or lying supine |
| Position of the clinician | Anterior to the patient |
| Action before palpating | Ask the patient to gently tuck their chin |
| Part of the body to palpate | The superior surface of the hyoid bone |
| How to palpate | Very gently place your fingertips on the superior surface of the hyoid bone |
| Sensation | It feels like resting your fingers on a shelf |
| Action during palpating | Ask the patient to swallow |
| Sensation during palpating | Let your fingers move up and then down during the swallow |
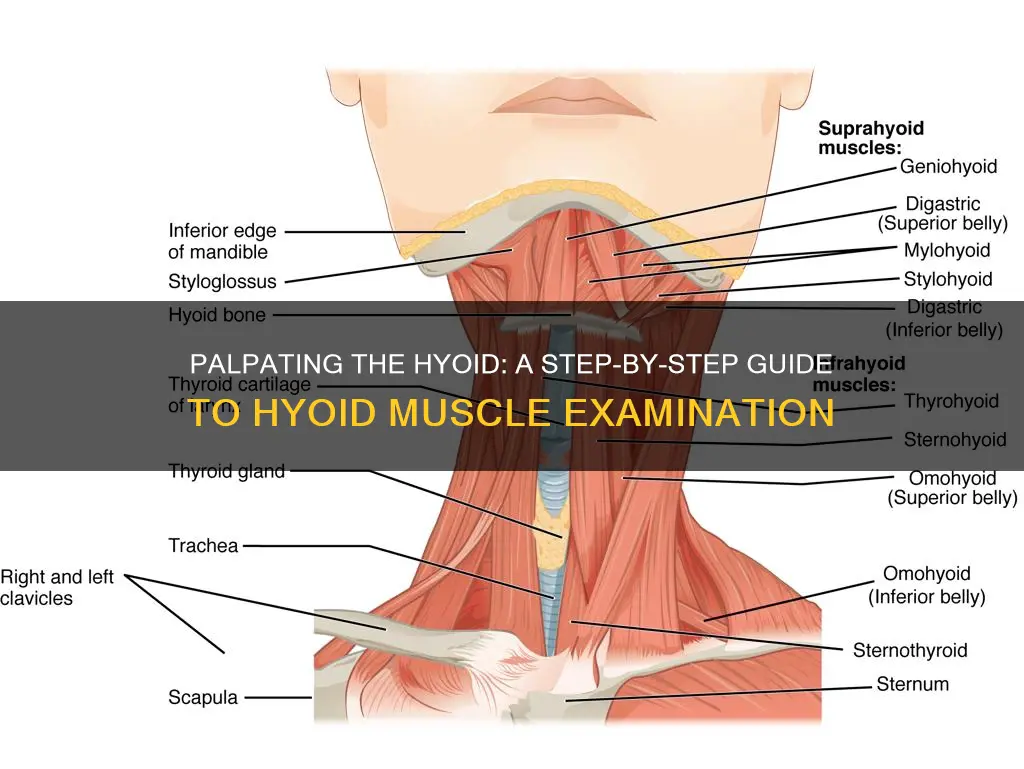
| Muscles connected to the hyoid bone | Suprahyoid and infrahyoid muscles |
| Suprahyoid muscles | Digastric, stylohyoid, mylohyoid, and geniohyoid |
| Infrahyoid muscles | Sternohyoid, sternothyroid, omohyoid, and thyrohyoid |
Explore related products






What You'll Learn
![]()
Patient positioning
To palpate the hyoid muscles, the patient should be positioned in a seated or reclined position, with their head and neck supported upright on the bed. The clinician should then identify the hyoid bone by locating the greater and lesser horns of the hyoid. This can be done by running your finger down the free edge of the thyroid cartilage (Adam's apple) and feeling for the cricoid cartilage just below it. The clinician should then place their first two digits of both hands just below the cricoid cartilage so that the left and right fingers meet on the patient's midline.
The middle finger should be placed on the identified spot, with the forefinger above it to palpate the base of the tongue, and the ring finger below on the thyroid notch. The little finger should be placed on the cricoid. This is known as the four-finger placement. The clinician can then ask the patient to swallow saliva to sense the hyoid movement upward, forward, and downward post-swallow.
It is important to note that the hyoid bone cannot be felt in the midline, although sometimes its lateral end is misidentified as a hard lymph node. Thus, it is crucial to have a proper understanding of the anatomy and the correct patient positioning to ensure accurate palpation and assessment.
Muscle Tears: When Surgery is the Only Option
You may want to see also
Explore related products

![]()
Clinician finger placement
The hyoid bone is a small, U-shaped (or horseshoe-shaped) bone situated in the midline of the neck at the base of the mandible. It is considered an unconventional bone as it is not interconnected with any adjacent bones. It is closely linked with an extended tendon-muscular complex and is considered a bone of clinical and forensic significance.
When palpating the hyoid bone, the clinician should first ask the patient to gently tuck their chin. The clinician then places their finger tips gently on the superior surface of the hyoid bone, which will feel like resting your fingers on a shelf. The patient is then asked to swallow, allowing the clinician to feel the hyoid move up and down.
The S-Hyoid Finder method is a technique used by dysphagia clinicians to identify key landmarks with ease and precision. This involves the clinician running their forefinger down the midline of the patient's face, over the mandible and the patient's fingers, which are placed under the mandibular margin. The clinician's forefinger will then land on a small depression or supple area immediately posterior to the patient's fingers. The clinician palpates gently in this depression and can feel for the hyoid bone in that space. Asking the patient to swallow again allows the clinician to sense the hyoid's movement. The clinician can then keep their middle finger on the identified spot, moving their forefinger above to palpate the base of the tongue, and their ring and little fingers to the thyroid notch and cricoid, respectively (four-finger placement).
The stylohyoid ligament connects the hyoid bone to the styloid process, and the hyoid is steadied by pressure applied to the opposite side. The clinician places their index finger on the greater cornu on the non-painful side and uses their thumb to stabilize the affected greater cornu. The hyoid is then rocked from side to side.
Muscle-Skin Connection: Understanding the Attachment Science
You may want to see also
![]()
Patient swallow
The hyoid bone and hyoid muscles play a crucial role in the act of swallowing, and palpation is a technique used to assess hyolaryngeal excursion, or the movement of the hyoid bone and larynx during swallowing. This can help clinicians understand a patient's swallowing function and identify any potential issues or disorders, such as dysphagia.
To perform a patient swallow assessment, the clinician will first identify the hyoid bone by palpating the depression in the patient's neck and feeling for the hyoid. The patient is then asked to swallow saliva, and the clinician can sense the upward, forward, and downward movement of the hyoid bone post-swallow. This is often done with the clinician's middle finger on the hyoid bone, their forefinger on the base of the tongue, the ring finger on the thyroid notch, and the little finger on the cricoid—known as the four-finger placement. This technique allows for a clinical assessment of the patient's swallow.
It is important to note that laryngeal palpation can be challenging when there is excess adipose tissue in the neck, as it may impede the ability to properly sense the movement of the larynx. In such cases, applying more pressure during palpation may be necessary, but care must be taken not to choke the patient. Additionally, terms like "appeared to be" or "suspect" should be used to reflect the subjective nature of the assessment.
The patient may be asked to take cup sips of thin liquids during the evaluation to observe hyolaryngeal movement. The timing and completeness of the swallow, as well as the number of swallows, are important factors to consider. Delayed hyolaryngeal movement or differences between the first and final swallows (e.g., slower final swallows) may indicate patient fatigue or other issues. If there are any signs of pharyngeal or oesophageal involvement, an instrumental evaluation is recommended to further investigate the patient's swallowing function.
In addition to palpation, other methods such as muscle ultrasound and videofluoroscopy are also used to assess hyoid muscle function during swallowing. Ultrasound investigations, for example, can focus on the dynamic movements of the geniohyoid muscle and the influence of bolus size on velocity, slope distance, and swallow time. This can be particularly relevant for patients with muscle wasting, where the force and speed of muscle contraction may be altered, leading to potential dyssynchrony during swallowing.
The Muscles of the Mouth: A Complex System
You may want to see also
![]()
Clinician finger movement
The hyoid bone is a small, U-shaped (or horseshoe-shaped) bone situated in the midline of the neck, at the base of the mandible. It is considered an unconventional bone as it is not interconnected to any adjacent bones. However, it is closely linked with an extended tendon-muscular complex and is considered a bone of clinical and forensic significance.
When palpating the hyoid, the clinician should first ask the patient to gently tuck their chin. The clinician then places their finger tips gently on the superior surface of the hyoid bone. This will feel like resting your fingers on a shelf. The patient is then asked to swallow, and the clinician will be able to feel the hyoid move up and down.
The clinician can then run their forefinger down the midline of the patient's face, over the mandible, and the patient's fingers, which should be placed under the mandibular margin. The clinician's forefinger will then land on a small depression immediately posterior to the patient's fingers. The clinician palpates gently in this depression and can feel for the hyoid. Asking the patient to swallow again will allow the clinician to sense the hyoid's movement.
The clinician can then keep their middle finger on the identified spot, and move their forefinger above to palpate the base of the tongue. The ring finger is placed below on the thyroid notch, and the little finger on the cricoid (four-finger placement). The patient is asked to swallow again, and the clinician clinically assesses this action.
The index finger is placed on the greater cornu on the non-painful side, and the clinician uses their thumb to stabilise the affected greater cornu. The hyoid is then rocked from side to side.
Muscles: A Complex Organ of Discrete Power Units
You may want to see also
![]()
Hyoid bone identification
The hyoid bone is a small, U-shaped (or horseshoe-shaped) bone situated in the midline of the neck. It is located at the base of the mandible and is considered an unconventional bone as it is not interconnected with any adjacent bones. The hyoid is closely linked with an extended tendon-muscular complex and anchored in the anterior triangle of the neck by muscles from the larynx, pharynx, tongue, and the floor of the mouth.
To palpate the hyoid bone, the patient can be sitting, standing, or lying supine. Ask the patient to gently tuck their chin and gently place your fingertips on the superior surface of the hyoid bone. This will feel like resting your fingers on a shelf. Ask the patient to swallow and let your fingers move up and down during the swallow.
Another method to identify the hyoid bone is the S-Hyoid Finder method. Here, the clinician runs their forefinger along the midline of the patient's face, over the mandible, and the patient's fingers, which are placed under the mandibular margin. The clinician's forefinger will land on a small depression or supple area immediately posterior to the patient's fingers. The clinician then palpates gently in that depression and feels for the hyoid. Asking the patient to swallow will allow the clinician to sense the hyoid's movement upward, forward, and downward post-swallow.
The stylohyoid ligament suspends the hyoid from the temporal styloid process on either side. The styloid process is a bony projection that originates from the petrous part of the temporal bone. From this process, three muscles originate: the stylopharyngeus, the styloglossus, and the stylohyoideus.
Relieving Muscle Soreness: Effective Strategies for Quick Recovery
You may want to see also
Frequently asked questions
The hyoid bone is a small, U-shaped (or horseshoe-shaped) bone located in the midline of the neck at the base of the mandible. It is considered an unconventional bone as it is not interconnected with any adjacent bones.
To palpate the hyoid bone, ask the patient to gently tuck their chin. Place your fingertips gently on the superior surface of the hyoid bone and ask the patient to swallow. You should feel the hyoid move up, forward, and down.
The hyoid functions as an anchor for the suprahyoid muscles (digastric, stylohyoid, mylohyoid, and geniohyoid) and the infrahyoid muscles (sternohyoid, sternothyroid, omohyoid, and thyrohyoid).
The stylohyoid ligament connects the lesser horn of the hyoid to the tip of the styloid process.
Hyoid bone syndrome, or hyoid bone insertion tendinitis, is neck pain that increases with swallowing and movement of the neck. The pain can be dull or sharp and radiates to the temporal area, posterior pharyngeal wall, sternocleidomastoid muscle, ear, and supraclavicular region.