The iliotibial band, or IT band, is a thick band of fascia formed proximally at the hip by the fascia of the gluteus maximus, gluteus medius, and tensor fasciae latae muscles. It is not a muscle, but a tendon that can get irritated or swollen from rubbing against hip or knee bones. This causes iliotibial band syndrome, or IT band syndrome, which is a common injury in runners, cyclists, and other athletes. The condition causes pain on the outside of the knee and can be treated with physical therapy, medication, or, in rare cases, surgery.
| Characteristics | Values |
|---|---|
| Composition | Collagen fibres, elastin fibres, fascia tissue |
| Structure | Longitudinal fibrous sheath, thick band of fascia |
| Functions | Pelvic stabilisation, posture control, supports knee during flexion and extension, helps lift the leg to the front and side of the body |
| Location | Runs from the hip to the knee, along the lateral thigh |
| Blood supply | Ascending branch of the lateral femoral circumflex artery (LFCA) |
| Innervation | Superior gluteal nerve (SGN), inferior gluteal nerve (IGN) |
| Conditions | Iliotibial band syndrome (ITBS), snapping hip syndrome, iliotibial band friction syndrome, iliotibial band impingement syndrome |
| Symptoms | Knee pain, hip pain, swelling, irritation, inflammation |
| Risk factors | Weak hip muscles, excessive foot pronation, hip abductor weakness, decreased flexibility, muscle strength imbalances, faulty movement patterns, repetitive motion (running, rowing, cycling), exercising on uneven surfaces |
| Treatment | Physical therapy, medications, surgery, steroid injections, soft-tissue work, dry needling, NSAIDs, strengthening core and gluteal muscles, leg-strengthening exercises |
Explore related products






What You'll Learn
![]()
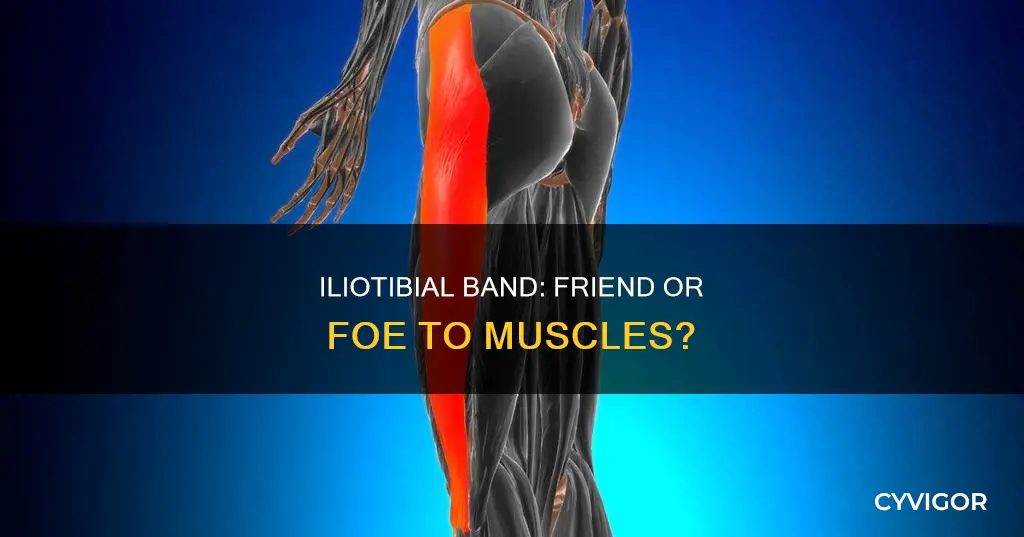
The iliotibial band is not a muscle
The iliotibial band (ITB) is not a muscle. It is a tendon, a thick band of fascia, or flexible fibrous tissue, that runs from the hip to just below the outside of the knee. The ITB is formed proximally at the hip by the fascia of the gluteus maximus, gluteus medius, and tensor fasciae latae muscles. Its main functions are pelvic stabilisation and posture control.
The ITB is involved in lower extremity motion, helping to lift the leg to the front and side of the body and supporting the knee during flexion and extension. It has no bony attachment along the femur, so it can shift front to back as the knee flexes and extends. The collagen fibres in the ITB are aligned vertically, allowing for better force absorption during weight-bearing activities. There is also a small amount of elastin fibre, which gives the ITB some elasticity and pliability. However, it cannot stretch like a muscle.
IT band syndrome is a common overuse injury, causing pain on the outside of the knee. It is often seen in runners, cyclists, and other athletes, as well as active adults and children. The syndrome is caused when the ITB gets irritated or swollen from rubbing against the hip or knee bones due to repetitive motion. This can lead to inflammation and pain along the outside of the leg.
To prevent and treat IT band syndrome, it is important to maintain core, leg, and gluteal muscle strength and flexibility, as well as correct any training errors that may contribute to the injury. Physical therapy and exercises that target the whole leg can help relieve the IT band's workload.
Understanding Muscle Fiber Types and Their Functions
You may want to see also
Explore related products






![]()
Iliotibial band syndrome (ITBS)
The iliotibial band (ITB) is a thick band of fascia formed proximally at the hip by the fascia of the gluteus maximus, gluteus medius, and tensor fasciae latae muscles. It is made up mostly of collagen fibres, with a small amount of elastin fibres that give it some elasticity. The ITB runs from the hip to the kneecap, serving as an important structure involved in lower extremity motion.
The exact cause of ITBS is still being debated, but it is believed to be related to repetitive knee movements that irritate the surrounding tissues. Other factors that may contribute to ITBS include individual anatomy, flexibility, and muscle strength. For example, variations in hip and knee alignment, decreased flexibility, and muscle strength imbalances can increase strain on the ITB.
ITBS can affect one or both legs and is characterised by aching or sharp pain on the outside of the knee or hip. Other symptoms include grating sounds or feelings when moving the knee or hip, pain over the greater trochanter of the hip, and pain that worsens when going downhill.
Treatment for ITBS typically involves rest from activities that exacerbate the pain, followed by a gradual return to these activities. Physical therapy, medications, and, in rare cases, surgery may also be recommended. Preventative measures include correcting individual risk factors, improving flexibility and strength, and adopting proper exercise techniques.
Tendons' Intricate Attachment to Muscles Explained
You may want to see also
Explore related products






![]()
ITBS causes
The iliotibial band (ITB) is a thick band of fascia formed proximally at the hip by the fascia of the gluteus maximus, gluteus medius, and tensor fasciae latae muscles. It is not a muscle, but a tendon.
ITBS is caused by the iliotibial band rubbing against the hip or knee bones, causing friction and irritation. This friction leads to inflammation in the bone, tendons, and small, fluid-filled sacs in the area. The iliotibial band may also abnormally compress the tissue beneath it, causing pain. ITBS is associated with repetitive bending and extending of the knee, which is common in distance runners, but may also occur in other sports such as cycling, skiing, rowing, or soccer.
There are several factors that can increase the risk of developing ITBS. These include bowed legs, having one leg longer than the other, knee arthritis, rotating the ankle, leg, or foot inward when moving, and weakness in the hip, butt, or abdominal muscles. Additionally, decreased flexibility and muscle strength imbalances in the pelvis, hip, knees, foot, and ankle can lead to faulty movement patterns and increased stress on the ITB. Training on tilted surfaces, sudden increases in training volume or intensity, improper footwear, and inadequate rest or stretching before exercise can also contribute to ITBS.
ITBS is a common injury among athletes, especially those involved in running, cycling, and other sports requiring repetitive knee movements. It is important to note that anyone can develop ITBS, and it is not limited to athletes. However, certain traits or activities can increase the likelihood of experiencing ITBS.
Understanding Muscle Hypertonicity: Causes, Effects, and Management
You may want to see also
Explore related products






![]()
ITBS treatments
Iliotibial Band Syndrome (ITBS) is a medical condition that causes pain on the outside of the knee. It is commonly found in athletes, especially distance runners, but anyone can get it. The iliotibial band is a strong, thick band of tissue that runs down the outside of the thigh, from the hip bones to the top of the shinbone. When the leg is bent and extended, the band moves over the outer lower edge of the thighbone, and repeated bending and extending of the knee can irritate the surrounding tissues, causing pain.
If you suspect you have ITBS, you should consult a sports medicine physician, physiatrist, or physical therapist. A doctor will interview you about your medical history and symptoms and conduct a physical exam to determine whether you have ITBS or a different condition with similar symptoms, such as a runner's knee, meniscus injuries, or stress fracture.
If you are diagnosed with ITBS, there are several treatment options available:
- Rest and Ice: The initial treatment for ITBS aims to reduce pain and inflammation. This can be done by resting the affected area and applying ice or a cold compress for 15-20 minutes at a time, every two to three hours.
- Medicines: Over-the-counter painkillers such as non-steroidal anti-inflammatory drugs (NSAIDs), including ibuprofen, can help ease pain and reduce inflammation.
- Physical Therapy: Physiotherapy can be effective in gradually getting you back to your usual activities. A physical therapist can work with you to identify your individual risk factors and start a treatment and prevention strategy, which may include specific strengthening exercises to do at home.
- Stretching and Strengthening Exercises: Intermittent stretching interventions may not change the ITB's length or mechanical properties, but a comprehensive exercise program should include flexibility and strength training.
- Running Retraining: This is a promising intervention for ITBS, but more research is needed to test different physiotherapeutic treatment approaches.
- Surgery: In rare instances, if other treatments have not worked, surgery may be recommended to remove the part of the iliotibial band that moves over the femur.
In addition to these treatments, there are some general guidelines to prevent ITBS or stop it from getting worse:
- Proper conditioning
- A slow increase in activity
- Warm-up and stretching before exercise
- Wearing proper shoes for the activity
- Avoiding crowned surfaces or too much running on a track
- Shortening the running stride
- Improving your running form and bike fit
Muscle Testing: Understanding the Procedure and Benefits
You may want to see also
Explore related products






![]()
Iliotibial band composition
The iliotibial band (ITB) is a thick band of fascia formed proximally at the hip by the fascia of the gluteus maximus, gluteus medius, and tensor fasciae latae muscles. It is a longitudinal fibrous reinforcement of the fascia lata. The ITB is also sometimes known as Maissiat's band.
The ITB is made up of mostly collagen fibres. Collagen is the strongest protein found in nature. The collagen fibres are aligned in a very organised, vertical fashion as this allows for better force absorption with weight-bearing activities. There is a small amount of elastin fibres among the layers of collagen, which allow it to be slightly elastic and pliable, helping it to act as a spring. However, this does not give it the ability to stretch like a muscle. The ITB is a tendinous extension of the tensor fascia lata (TFL) and is, therefore, a tendon itself.
The TFL is the deep investing fascia of the thigh, encompassing the muscles of the hip and lower extremity in this region. Proximally in the thigh, the ITB receives fascial contributions from the deep fascia of the thigh, gluteus maximus, and tensor fascia lata. Distally, the ITB becomes a distinct soft tissue layer of the lateral knee. The gluteus maximus muscle and the tensor fasciae latae insert upon the tract. The ITB contributes to lateral knee stabilization.
The ITB runs along the lateral thigh and serves as an important structure involved in lower extremity motion. Its main functions are pelvic stabilization and posture control. The ITB moves anterior to the lateral condyle of the femur during knee extension, while at about 30 degrees of knee flexion, the ITB moves posterior to the lateral condyle.
MRI Scans: Muscle Visibility and What They Show
You may want to see also
Frequently asked questions
The iliotibial band (ITB) is a thick band of fascia that runs from the hip to just below the outside of the knee. It is made up of mostly collagen fibres, with a small amount of elastin fibres.
The iliotibial band helps lift your leg to the front and side of your body, and supports your knee during flexion and extension. It also helps with pelvic stabilisation and posture control.
Iliotibial band syndrome (ITBS) is when the iliotibial band becomes irritated or swollen from rubbing against your hip or knee bones, causing pain on the outside of the knee. It is a common overuse injury, often seen in runners, cyclists and other athletes.
Treatment for iliotibial band syndrome can include physical therapy, medication or, in rare cases, surgery. To prevent the syndrome, you can maintain your core, leg and gluteal muscle strength, and ensure you are correctly stretching and resting.