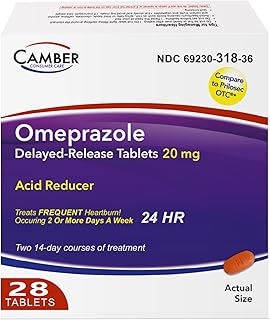
Omeprazole is a widely recognized medication primarily used to treat conditions related to excess stomach acid, such as gastroesophageal reflux disease (GERD), ulcers, and Zollinger-Ellison syndrome. It belongs to a class of drugs known as proton pump inhibitors (PPIs), which work by reducing the production of acid in the stomach. While omeprazole is highly effective for its intended uses, it is not classified as a muscle relaxer. Muscle relaxers, also known as skeletal muscle relaxants, are medications designed to alleviate muscle spasms, pain, and stiffness by acting on the central nervous system or directly on the muscles. Since omeprazole’s mechanism of action is unrelated to muscle relaxation, it is not used for this purpose, and individuals seeking relief from muscle-related issues should consult a healthcare provider for appropriate treatment options.
Explore related products

$33.99

$14.28 $22.79




What You'll Learn
- Omeprazole's primary function: acid reducer, not muscle relaxant
- Muscle relaxers vs. PPIs: different drug classes, distinct uses
- Omeprazole side effects: no muscle relaxation properties listed
- Common muscle relaxers: cyclobenzaprine, baclofen, not omeprazole
- Omeprazole usage: treats GERD, ulcers, not muscle-related conditions
![]()
Omeprazole's primary function: acid reducer, not muscle relaxant
Omeprazole is a proton pump inhibitor (PPI) primarily designed to reduce stomach acid production. Its mechanism of action involves blocking the enzyme in the stomach wall that produces acid, providing relief from conditions like gastroesophageal reflux disease (GERD), peptic ulcers, and Zollinger-Ellison syndrome. Typically, adults are prescribed 20–40 mg once daily, taken 30–60 minutes before breakfast for optimal effectiveness. This targeted approach to acid reduction distinguishes omeprazole from muscle relaxants, which act on the central nervous system or muscle fibers to alleviate tension and pain.
Confusion may arise when patients experience muscle-related side effects while taking omeprazole, such as muscle pain or weakness. However, these symptoms are not due to omeprazole acting as a muscle relaxant but rather as potential adverse reactions. Long-term use of PPIs like omeprazole has been associated with magnesium deficiency, which can contribute to muscle cramps or spasms. To mitigate this, healthcare providers may recommend magnesium supplements or periodic monitoring of electrolyte levels, especially in older adults or those on prolonged therapy.
Comparatively, muscle relaxants like cyclobenzaprine or baclofen work by depressing the central nervous system or directly affecting muscle fibers to reduce spasms and pain. Omeprazole, on the other hand, has no such mechanism. Patients seeking relief from muscle tension should consult their healthcare provider for appropriate medications, as using omeprazole for this purpose would be ineffective and potentially misleading. Clear communication about the drug’s intended use is essential to avoid confusion and ensure proper treatment.
Practically, individuals prescribed omeprazole should adhere to specific guidelines to maximize its benefits. For instance, the delayed-release capsules should not be crushed or chewed, as this can compromise their enteric coating. Additionally, omeprazole is not intended for immediate relief of heartburn; antacids may be used concurrently for quick symptom management. Patients should also be aware that omeprazole’s effects may take several days to manifest fully, requiring consistent use as directed. By understanding its primary function as an acid reducer, users can manage expectations and use the medication appropriately.
In summary, omeprazole’s role as an acid reducer is distinct from that of a muscle relaxant, both in mechanism and purpose. While side effects like muscle pain may occur, they are unrelated to muscle relaxation and should prompt medical evaluation rather than misuse of the drug. Adhering to prescribed dosages, understanding its limitations, and recognizing potential side effects ensures safe and effective use of omeprazole for its intended purpose. Clarity in its function prevents misapplication and fosters informed patient decisions.
Pre-Race Muscle Relaxation: Techniques for Optimal Performance and Recovery
You may want to see also
Explore related products

$9.99





![]()
Muscle relaxers vs. PPIs: different drug classes, distinct uses
Omeprazole is not a muscle relaxer. This common misconception stems from its widespread use in treating gastrointestinal issues, while muscle relaxers target entirely different physiological systems. Understanding the distinction between these two drug classes—proton pump inhibitors (PPIs) like omeprazole and muscle relaxers—is crucial for safe and effective medication use.
PPIs, including omeprazole, work by reducing stomach acid production. They are primarily prescribed for conditions such as gastroesophageal reflux disease (GERD), peptic ulcers, and Zollinger-Ellison syndrome. Omeprazole, typically taken once daily in doses of 20–40 mg, inhibits the enzyme responsible for acid secretion in the stomach lining. Its mechanism of action is systemic but focused on the gastrointestinal tract, offering no direct effect on muscle tension or relaxation.
Muscle relaxers, on the other hand, are a diverse group of medications designed to alleviate muscle spasms, stiffness, and pain. They act on the central nervous system or directly on muscle fibers to reduce contraction. Examples include cyclobenzaprine (Flexeril), tizanidine (Zanaflex), and baclofen. These drugs are often prescribed for acute musculoskeletal conditions, such as lower back pain or injury-related spasms. Unlike PPIs, muscle relaxers carry a higher risk of side effects like drowsiness, dizziness, and impaired coordination, necessitating caution during activities like driving.
A key difference lies in their intended use and patient populations. PPIs are generally safe for long-term use in adults and, in some cases, children, though prolonged use may require monitoring for potential side effects like osteoporosis or vitamin B12 deficiency. Muscle relaxers, however, are typically recommended for short-term use (2–3 weeks) due to their sedative properties and potential for dependence. Combining these drug classes without medical supervision is inadvisable, as they serve distinct purposes and interact with the body in fundamentally different ways.
Practical tips for patients include verifying the purpose of each medication with a healthcare provider and adhering to prescribed dosages. For instance, if experiencing both acid reflux and muscle pain, a PPI like omeprazole should not be substituted for a muscle relaxer. Instead, consult a physician to address both conditions appropriately. Understanding these differences ensures targeted treatment and minimizes the risk of adverse effects, promoting better health outcomes.
Understanding Regular Strength Muscle Relaxer Dosage: How Many MG?
You may want to see also
Explore related products






![]()
Omeprazole side effects: no muscle relaxation properties listed
Omeprazole, a proton pump inhibitor (PPI), is widely prescribed to manage conditions like gastroesophageal reflux disease (GERD) and peptic ulcers by reducing stomach acid. Despite its effectiveness in these roles, a review of its side effects reveals no muscle relaxation properties. This absence is significant, as patients often seek multi-purpose medications to address overlapping symptoms. For instance, while omeprazole alleviates heartburn, it does not relieve muscle tension or spasms, which may coexist in individuals with stress-related gastrointestinal issues. Understanding this limitation helps healthcare providers tailor treatments more effectively, pairing omeprazole with appropriate muscle relaxants when necessary.
Analyzing the pharmacological profile of omeprazole clarifies why it lacks muscle relaxation properties. Unlike drugs such as cyclobenzaprine or tizanidine, which act on the central nervous system to reduce muscle tone, omeprazole targets parietal cells in the stomach to inhibit acid secretion. Its mechanism of action is highly specific, with no known interaction with muscle fibers or neural pathways involved in relaxation. This specificity is advantageous for minimizing systemic side effects but underscores the need for adjunctive therapies when muscle-related symptoms are present. Patients should be informed of this distinction to manage expectations and ensure comprehensive care.
From a practical standpoint, individuals prescribed omeprazole should monitor their symptoms closely to identify whether muscle tension or pain persists. For adults, the standard dosage of 20 mg once daily is effective for acid-related conditions but offers no relief for musculoskeletal discomfort. If muscle spasms or stiffness occur, consulting a healthcare provider for a separate muscle relaxant is advisable. Combining omeprazole with medications like baclofen or methocarbamol can address both gastrointestinal and muscular symptoms simultaneously, provided there are no contraindications. Always disclose all medications to avoid potential drug interactions.
A comparative perspective highlights the importance of aligning medication properties with patient needs. While omeprazole excels in managing acid-related disorders, its lack of muscle relaxation effects contrasts with drugs like dicyclomine, which treats gastrointestinal issues and acts as an antispasmodic. This comparison emphasizes the need for personalized treatment plans. For example, older adults or those with chronic conditions may require a dual approach, balancing acid suppression with muscle relaxation to improve overall quality of life. Clear communication between patients and providers is essential to navigate these distinctions.
In conclusion, omeprazole’s side effect profile notably excludes muscle relaxation properties, a fact that should guide its use in clinical practice. Patients and providers must recognize this limitation to avoid misconceptions and ensure holistic symptom management. By pairing omeprazole with targeted muscle relaxants when appropriate, healthcare professionals can address both gastrointestinal and musculoskeletal concerns effectively. This nuanced understanding enhances treatment outcomes and fosters informed decision-making in patient care.
Hyoscyamine as a Muscle Relaxer: Uses, Effects, and Safety
You may want to see also
Explore related products

$11.84 $15.99





![]()
Common muscle relaxers: cyclobenzaprine, baclofen, not omeprazole
Omeprazole, a proton pump inhibitor, is often confused with muscle relaxers due to its widespread use in treating gastrointestinal issues. However, it does not alleviate muscle spasms or tension. Instead, it reduces stomach acid, making it ineffective for muscle-related conditions. For those seeking relief from muscle pain, understanding the correct medications is crucial. Common muscle relaxers like cyclobenzaprine and baclofen are specifically designed to target muscle spasms and stiffness, offering distinct benefits and considerations for use.
Cyclobenzaprine, often prescribed under the brand name Flexeril, is a go-to option for acute muscle spasms, particularly in adults. Typically, a 5–10 mg dose is taken 3 times daily, with a maximum of 30 mg per day. It works by acting on the central nervous system to reduce muscle hyperactivity. However, it’s not suitable for long-term use due to potential side effects like drowsiness and dizziness. Patients should avoid alcohol and activities requiring alertness while on this medication. For older adults, lower doses are often recommended to minimize risks.
Baclofen, sold as Lioresal, is another muscle relaxer commonly used for conditions like multiple sclerosis or spinal cord injuries. It acts directly on the spinal cord to inhibit nerve signals causing muscle spasms. Dosage starts at 5 mg three times daily and can increase gradually to 20 mg three times daily, depending on tolerance. Unlike cyclobenzaprine, baclofen can be used long-term but requires careful monitoring due to potential withdrawal symptoms if stopped abruptly. It’s also important to note that baclofen can cause drowsiness, so patients should adjust their activities accordingly.
Comparing these two, cyclobenzaprine is ideal for short-term relief of acute muscle spasms, while baclofen is better suited for chronic conditions requiring prolonged management. Neither should be confused with omeprazole, which serves an entirely different purpose. Always consult a healthcare provider to determine the most appropriate medication for your specific needs, as misuse can lead to ineffective treatment or adverse effects. Proper usage ensures maximum benefit with minimal risk.
Do Muscle Relaxers Cause Numbness? Exploring Side Effects and Sensations
You may want to see also
Explore related products






![]()
Omeprazole usage: treats GERD, ulcers, not muscle-related conditions
Omeprazole, a proton pump inhibitor (PPI), is widely recognized for its effectiveness in managing acid-related disorders, but it is not a muscle relaxer. This distinction is crucial for patients seeking relief from specific conditions. While muscle relaxers target musculoskeletal issues by alleviating tension and pain, omeprazole works by reducing stomach acid production. Its primary uses include treating gastroesophageal reflux disease (GERD), peptic ulcers, and erosive esophagitis. For instance, a standard dosage of 20 mg once daily for 4–8 weeks is often prescribed for GERD, with adjustments based on severity and patient response. Understanding this clear functional difference ensures that individuals receive appropriate treatment for their symptoms.
Consider the mechanism of action to further clarify why omeprazole is not a muscle relaxer. PPIs like omeprazole inhibit the enzyme in the stomach wall that produces acid, providing relief from acid-induced damage. In contrast, muscle relaxers, such as cyclobenzaprine or baclofen, act on the central nervous system or directly on muscles to reduce spasms and pain. For example, cyclobenzaprine is often prescribed for acute musculoskeletal conditions at doses of 5–10 mg three times daily. This comparison highlights the distinct purposes of these medications, emphasizing that omeprazole’s role is strictly acid suppression, not muscle relaxation.
Practical application of omeprazole underscores its inapplicability to muscle-related conditions. Patients with GERD or ulcers often experience symptoms like heartburn, regurgitation, or abdominal pain, which omeprazole effectively addresses. However, those with muscle strains, spasms, or chronic pain require a different therapeutic approach. For instance, a 40-year-old with GERD might benefit from omeprazole 20 mg daily, while a 30-year-old with lower back spasms would need a muscle relaxer like tizanidine. Misidentifying omeprazole as a muscle relaxer could lead to delayed or ineffective treatment, reinforcing the importance of accurate medication selection.
Finally, it’s essential to consult healthcare providers for proper diagnosis and treatment. Self-medication based on misconceptions, such as using omeprazole for muscle pain, can exacerbate underlying issues. For example, a patient with acid reflux might mistakenly take a muscle relaxer, which would not address their condition. Conversely, someone with muscle spasms might take omeprazole, finding no relief. Healthcare professionals can provide tailored advice, such as recommending omeprazole for acid-related disorders while suggesting physical therapy or appropriate muscle relaxers for musculoskeletal issues. This clarity ensures effective, safe, and targeted treatment for all patients.
Traction Therapy: PubMed Insights on Muscle Relaxation Mechanisms
You may want to see also
Frequently asked questions
No, omeprazole is not a muscle relaxer. It is a proton pump inhibitor (PPI) used to reduce stomach acid production.
Omeprazole is primarily used to treat conditions caused by excess stomach acid, such as gastroesophageal reflux disease (GERD), ulcers, and heartburn.
No, omeprazole does not relieve muscle pain or tension, as it is not designed to act as a muscle relaxer or pain reliever.
Muscle relaxers include drugs like cyclobenzaprine, tizanidine, and baclofen, which are specifically prescribed to alleviate muscle spasms and tension, unlike omeprazole.