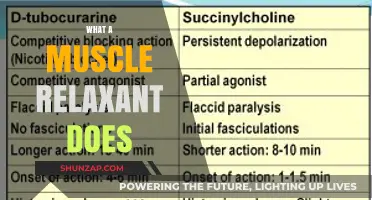
Depolarizing muscle relaxants are a class of neuromuscular blocking agents that act by prolonging the depolarization of the motor endplate, leading to muscle paralysis. Unlike non-depolarizing agents, which competitively block acetylcholine receptors, depolarizing relaxants mimic acetylcholine, binding to and activating these receptors, causing sustained depolarization and subsequent muscle relaxation. The most well-known example is succinylcholine, which is widely used in anesthesia to facilitate endotracheal intubation due to its rapid onset and short duration of action. However, its use is associated with specific risks, such as hyperkalemia and prolonged paralysis in certain patient populations, making careful patient selection and monitoring essential. Understanding the mechanism and clinical implications of depolarizing muscle relaxants is crucial for safe and effective use in medical practice.
| Characteristics | Values |
|---|---|
| Mechanism of Action | Bind to nicotinic acetylcholine receptors (nAChRs) at the neuromuscular junction, initially causing depolarization and muscle contraction, followed by desensitization and paralysis. |
| Examples | Succinylcholine (Suxamethonium), Decamethonium |
| Onset of Action | Rapid (within 30-60 seconds) |
| Duration of Action | Short (5-10 minutes for succinylcholine) |
| Metabolism | Rapidly hydrolyzed by plasma butyrylcholinesterase (pseudocholinesterase) |
| Clinical Uses | Induction of rapid sequence intubation (RSI), facilitation of endotracheal intubation, surgical paralysis |
| Side Effects | Muscle fasciculations, hyperkalemia, increased intraocular/intraabdominal pressure, malignant hyperthermia (rare), prolonged paralysis in deficient pseudocholinesterase activity |
| Contraindications | Hyperkalemia, burns, trauma, tetanus, personal/family history of malignant hyperthermia, myasthenia gravis, elevated intracranial pressure |
| Reversal Agent | None (effects wear off with metabolism/redistribution) |
| Pharmacokinetics | Distributed into extracellular fluid; minimal hepatic/renal elimination |
| Allergic Reactions | Rare (due to short duration and rapid metabolism) |
| Special Considerations | Requires careful monitoring of serum potassium levels; avoid in patients with neuromuscular diseases |
Explore related products






What You'll Learn
- Mechanism of Action: Bind to nicotinic receptors, prolonging depolarization and causing muscle paralysis
- Examples: Succinylcholine is the most common depolarizing muscle relaxant used clinically
- Onset and Duration: Rapid onset (30-60 seconds), short duration (5-10 minutes) due to rapid metabolism
- Clinical Uses: Induced during anesthesia for intubation, seizures, and short surgical procedures
- Side Effects: Bradycardia, hyperkalemia, muscle fasciculations, and potential malignant hyperthermia risk
![]()
Mechanism of Action: Bind to nicotinic receptors, prolonging depolarization and causing muscle paralysis
Depolarizing muscle relaxants are a unique class of neuromuscular blocking agents that exert their effects through a fascinating mechanism. Unlike their non-depolarizing counterparts, these drugs don't simply antagonize the nicotinic acetylcholine receptors at the neuromuscular junction. Instead, they bind to these receptors and activate them, mimicking the action of acetylcholine, the body's natural neurotransmitter. This initial activation leads to muscle fiber depolarization, causing a brief contraction.
Crucially, depolarizing muscle relaxants differ from acetylcholine in their duration of action. While acetylcholine is rapidly broken down by acetylcholinesterase, these drugs resist this enzyme's action, leading to a prolonged depolarization. This sustained depolarization ultimately results in muscle fiber fatigue and paralysis.
Understanding the Binding Process
Imagine the nicotinic receptor as a lock, and acetylcholine as its key. Depolarizing muscle relaxants act as a key that not only fits the lock but also gets stuck in it, preventing the lock from returning to its resting state. This prolonged binding keeps the ion channels open, allowing a continuous influx of sodium ions, leading to sustained depolarization.
Clinical Implications and Dosage
Succinylcholine, the prototypical depolarizing muscle relaxant, is commonly used in anesthesia to facilitate endotracheal intubation. Its rapid onset (within 30-60 seconds) and short duration of action (5-10 minutes) make it ideal for this purpose. Dosage is typically 1-2 mg/kg intravenously, with careful consideration of patient factors like age, renal function, and pre-existing conditions.
It's important to note that succinylcholine can trigger a massive release of potassium from muscle cells, potentially leading to hyperkalemia, particularly in patients with burns, trauma, or neuromuscular disorders. Therefore, its use requires careful monitoring and is contraindicated in certain populations.
Comparing Depolarizing and Non-Depolarizing Agents
While both types of muscle relaxants result in paralysis, their mechanisms and clinical profiles differ significantly. Non-depolarizing agents competitively block nicotinic receptors without activating them, leading to a more gradual onset and longer duration of action. They are often preferred for maintaining muscle relaxation during surgery. Depolarizing agents, with their rapid onset and short duration, are primarily used for brief procedures requiring quick intubation.
The choice between these agents depends on the specific surgical needs, patient characteristics, and potential side effects. Understanding their distinct mechanisms of action is crucial for informed clinical decision-making.
Effective Techniques to Release and Relax Tight Thoracic Muscles
You may want to see also
Explore related products






![]()
Examples: Succinylcholine is the most common depolarizing muscle relaxant used clinically
Depolarizing muscle relaxants are a class of drugs that induce muscle relaxation by activating the nicotinic acetylcholine receptors (nAChRs) at the neuromuscular junction, leading to prolonged depolarization and subsequent muscle paralysis. Among these agents, succinylcholine stands out as the most widely used in clinical practice. Its rapid onset (30–60 seconds) and short duration of action (5–10 minutes) make it ideal for procedures requiring brief, complete muscle relaxation, such as endotracheal intubation or electroconvulsive therapy. However, its use is not without risks, and understanding its mechanism, dosage, and contraindications is critical for safe administration.
Mechanism and Dosage: Succinylcholine mimics acetylcholine by binding to nAChRs, causing muscle fibers to depolarize. Unlike acetylcholine, it is not rapidly hydrolyzed by cholinesterases, leading to sustained depolarization and flaccid paralysis. The typical intravenous dose for adults is 1–2 mg/kg, with effects peaking within 1 minute. Pediatric dosing varies by age: 2 mg/kg for infants and 1–1.5 mg/kg for older children. It is crucial to avoid repeated dosing, as this can prolong paralysis due to cumulative effects. Always ensure adequate ventilation support, as succinylcholine paralyzes respiratory muscles, necessitating mechanical ventilation until recovery.
Clinical Applications and Cautions: While succinylcholine is invaluable for rapid sequence intubation, it is contraindicated in specific populations. Patients with malignant hyperthermia, muscular dystrophy, or severe burns are at risk of hyperkalemia due to massive skeletal muscle depolarization. In such cases, non-depolarizing alternatives like rocuronium are preferred. Additionally, prolonged immobilization or pre-existing elevated potassium levels (e.g., in renal failure) increase the risk of cardiac arrhythmias. Always pre-oxygenate patients and have resuscitation equipment readily available, as succinylcholine’s rapid onset leaves no margin for error during intubation.
Practical Tips for Administration: To minimize adverse effects, administer 100 mg of lidocaine intravenously 30–60 seconds before succinylcholine to attenuate its fasciculation-induced potassium release. Monitor for signs of hyperkalemia (e.g., ECG changes, muscle weakness) post-administration, especially in high-risk patients. For pediatric cases, ensure precise dosing based on weight and age, as overdosing can prolong paralysis. Finally, educate the team about the drug’s short duration; prepare for immediate extubation or reversal if necessary, but avoid succinylcholine in cases requiring prolonged paralysis.
Takeaway: Succinylcholine remains the gold standard depolarizing muscle relaxant due to its unmatched speed and reliability in critical scenarios. However, its use demands meticulous attention to patient selection, dosing, and monitoring. By adhering to guidelines and anticipating risks, clinicians can harness its benefits while mitigating potential complications, ensuring safe and effective muscle relaxation in time-sensitive procedures.
Muscle Relaxers and Bodybuilding: Benefits, Risks, and Impact Explained
You may want to see also
Explore related products






![]()
Onset and Duration: Rapid onset (30-60 seconds), short duration (5-10 minutes) due to rapid metabolism
Depolarizing muscle relaxants, such as succinylcholine, are unique in their rapid onset of action, typically occurring within 30 to 60 seconds after administration. This swift effect is due to their mechanism of action, which involves prolonged depolarization of the motor endplate, leading to muscle relaxation. For clinicians, this quick onset is invaluable in emergency situations, such as rapid sequence intubation, where immediate muscle paralysis is critical. However, the dosage must be carefully calibrated—usually 1–1.5 mg/kg for adults—to ensure efficacy without prolonging the effect unnecessarily.
The short duration of action, lasting only 5 to 10 minutes, is a direct result of the rapid metabolism of these agents, primarily by plasma pseudocholinesterase. This enzyme breaks down succinylcholine efficiently, making it ideal for brief procedures like endotracheal intubation or electroconvulsive therapy. However, this brevity also demands precise timing; clinicians must anticipate the need for additional doses or transition to a longer-acting agent if the procedure extends beyond the drug’s duration. Pediatric patients, due to their higher muscle mass-to-weight ratio, may experience slightly shorter durations, requiring closer monitoring.
While the rapid onset and short duration are advantageous, they also necessitate careful patient selection. Individuals with conditions that impair pseudocholinesterase activity, such as liver disease or genetic deficiencies, may experience prolonged paralysis, increasing the risk of complications like hyperkalemia. Similarly, patients with burns, trauma, or chronic illnesses may exhibit altered pharmacodynamics, requiring dose adjustments. Practitioners should always review the patient’s medical history and consider alternatives if depolarizing agents are contraindicated.
In practice, the key to leveraging these properties lies in anticipation and preparation. For instance, during rapid sequence intubation, the anesthesia provider must be ready to ventilate the patient immediately after succinylcholine administration, as apnea occurs swiftly. Additionally, having a non-depolarizing muscle relaxant on standby ensures continuity of muscle relaxation if needed. This combination of rapid onset, short duration, and metabolic considerations makes depolarizing agents both powerful and demanding tools in the anesthesiologist’s arsenal.
Is Nitrazepam a Muscle Relaxant? Exploring Its Uses and Effects
You may want to see also
Explore related products






![]()
Clinical Uses: Induced during anesthesia for intubation, seizures, and short surgical procedures
Depolarizing muscle relaxants, such as succinylcholine, are essential tools in anesthesia, particularly for rapid-sequence intubation (RSI). Their unique mechanism of action—prolonged depolarization of the neuromuscular junction—ensures immediate and profound muscle relaxation, making them ideal for securing the airway in emergency settings. A typical dose of 1–1.5 mg/kg intravenously achieves intubating conditions within 60 seconds, a critical advantage when managing patients with full stomachs or at risk of aspiration. However, their use is not without risks, including hyperkalemia, myalgia, and potential triggering of malignant hyperthermia in susceptible individuals. Thus, while indispensable for RSI, their selection demands careful patient assessment and monitoring.
In the context of seizures, depolarizing muscle relaxants serve a distinct but equally vital role. Status epilepticus, a life-threatening condition of prolonged or recurrent seizures, often requires rapid intervention to prevent neurological damage or respiratory compromise. Succinylcholine, administered at 1 mg/kg intravenously, can swiftly terminate seizures by inducing muscle paralysis, thereby interrupting the seizure’s motor manifestations. This effect is particularly useful when anticonvulsant medications fail to achieve control. However, its use in this setting is controversial due to the risk of hyperkalemia, especially in patients with pre-existing neurological conditions or prolonged seizure activity. Clinicians must weigh the benefits of rapid seizure cessation against the potential risks, often opting for alternative agents like benzodiazepines or non-depolarizing muscle relaxants in less urgent cases.
Short surgical procedures, particularly those requiring brief but complete muscle relaxation, also benefit from depolarizing muscle relaxants. For instance, in pediatric patients undergoing procedures like lumbar puncture or reduction of fractures, succinylcholine’s rapid onset and short duration of action (3–5 minutes) align well with the procedural timeline. A dose of 2–3 mg/kg intramuscularly in children ensures adequate relaxation without prolonging recovery time. However, its use in this population requires caution, as children are more susceptible to side effects such as postoperative myalgia. Additionally, the drug’s cholinesterase-dependent metabolism necessitates avoiding its use in patients with genetic cholinesterase deficiency or those on cholinesterase inhibitors.
Despite their clinical utility, depolarizing muscle relaxants are not universally applicable. Contraindications include hyperkalemia, burns, trauma, and neuromuscular diseases, where their use can exacerbate potassium release from damaged tissues. Practitioners must also consider the drug’s pharmacokinetics, particularly in elderly patients or those with renal impairment, where prolonged effects may occur. Practical tips include ensuring adequate ventilation post-administration, as apnea is immediate and complete, and having reversal agents like neostigmine available, though typically unnecessary due to the drug’s short duration. In summary, while depolarizing muscle relaxants offer unparalleled advantages in specific clinical scenarios, their use requires precision, vigilance, and a thorough understanding of patient-specific risks.
Soothing Soaks: How Baths Effectively Relax and Ease Muscles
You may want to see also
Explore related products






![]()
Side Effects: Bradycardia, hyperkalemia, muscle fasciculations, and potential malignant hyperthermia risk
Depolarizing muscle relaxants, such as succinylcholine, are potent agents used to induce rapid muscle paralysis during surgical procedures. While their efficacy is undeniable, their mechanism of action—prolonged depolarization of the neuromuscular junction—triggers a cascade of side effects that demand careful monitoring and management. Among these, bradycardia, hyperkalemia, muscle fasciculations, and the risk of malignant hyperthermia stand out as critical concerns, each requiring specific attention to ensure patient safety.
Bradycardia, a slowing of the heart rate, is a well-documented side effect of depolarizing muscle relaxants, particularly in pediatric and elderly patients. Succinylcholine stimulates muscarinic receptors in the heart, leading to reflex bradycardia, which can be profound in infants and young children. To mitigate this risk, pretreatment with anticholinergic agents like glycopyrrolate (0.01 mg/kg) is recommended, especially in patients under 12 years of age. Clinicians should also be prepared to administer atropine (0.02 mg/kg) if bradycardia occurs, ensuring immediate access to emergency medications during induction.
Hyperkalemia poses a more insidious threat, particularly in patients with predisposing conditions such as burns, trauma, or neuromuscular disorders. Succinylcholine causes a transient release of potassium from skeletal muscles, which can elevate serum potassium levels by 0.5–1.0 mEq/L. In vulnerable populations, this increase may trigger life-threatening arrhythmias. Preoperative screening for at-risk patients is essential, and alternatives to succinylcholine should be considered. If used, continuous electrocardiographic monitoring is mandatory, and calcium gluconate (10–20 mL of 10% solution) should be readily available to stabilize the myocardium in case of hyperkalemic complications.
Muscle fasciculations, though brief and often benign, can be distressing to patients if not adequately sedated. These involuntary muscle twitches occur due to the initial depolarization phase before paralysis sets in. To minimize fasciculations, ensure patients are deeply anesthetized with a potent induction agent like propofol or etomidate before administering succinylcholine. Additionally, a small dose of a non-depolarizing muscle relaxant (e.g., vecuronium 0.03 mg/kg) can be given 30–60 seconds prior to succinylcholine to attenuate fasciculations without delaying intubation.
Finally, the risk of malignant hyperthermia (MH) looms as a rare but catastrophic complication. Succinylcholine, though not a direct trigger of MH, can exacerbate the condition in susceptible individuals. Patients with a personal or family history of MH or unexplained anesthesia-related complications should avoid depolarizing muscle relaxants altogether. For all patients, early recognition of MH signs—rigidity, tachycardia, hypercarbia, and hyperthermia—is critical. Treatment protocols, including immediate discontinuation of triggering agents and administration of dantrolene (2.5 mg/kg IV), must be readily accessible in any setting where succinylcholine is used.
In summary, while depolarizing muscle relaxants offer unparalleled rapidity of onset, their side effects necessitate meticulous planning and vigilance. By understanding the mechanisms behind bradycardia, hyperkalemia, muscle fasciculations, and MH risk, clinicians can optimize patient outcomes through tailored pretreatment, vigilant monitoring, and prompt intervention.
Gabapentin for Muscle Relaxation: Efficacy, Uses, and Side Effects Explained
You may want to see also
Frequently asked questions
Depolarizing muscle relaxants are a class of drugs that cause muscle relaxation by prolonged depolarization of the motor end plate, leading to temporary paralysis.
Depolarizing muscle relaxants mimic the action of acetylcholine, binding to nicotinic receptors at the neuromuscular junction, causing sustained depolarization and preventing further muscle contraction.
Succinylcholine is the most commonly used depolarizing muscle relaxant, widely utilized in anesthesia to facilitate endotracheal intubation and provide skeletal muscle relaxation during surgical procedures.
Common side effects include muscle fasciculations, increased potassium release, hyperkalemia (especially in susceptible individuals), and prolonged apnea due to neuromuscular blockade.
Depolarizing muscle relaxants are preferred in situations requiring rapid onset and short duration of action, such as emergency intubation, or when a non-depolarizing agent might be contraindicated.