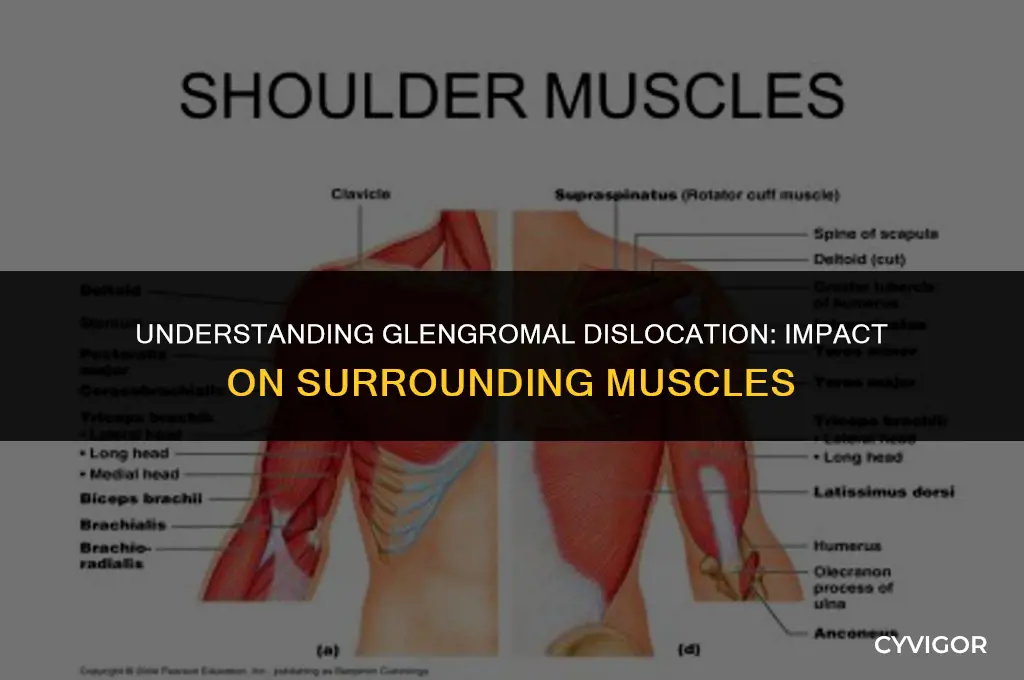
A glenohumeral dislocation, commonly referred to as a shoulder dislocation, occurs when the head of the upper arm bone (humerus) is forced out of the shoulder socket (glenoid). This injury can significantly impact the muscles surrounding the shoulder joint. The primary muscles affected include the deltoid, which covers the shoulder and helps in lifting the arm; the rotator cuff muscles (supraspinatus, infraspinatus, teres minor, and subscapularis), which stabilize the shoulder and enable rotation; and the pectoralis major, which assists in shoulder movement and arm rotation. Additionally, the biceps and triceps may also be affected due to their role in stabilizing the shoulder joint. Understanding the impact on these muscles is crucial for effective treatment and rehabilitation strategies.
| Characteristics | Values |
|---|---|
| Muscle Name | Gluteus maximus, Gluteus medius, Gluteus minimus, Piriformis, Obturator internus, Obturator externus, Gracilis, Sartorius, Iliopsoas, Rectus femoris, Vastus lateralis, Vastus intermedius, Vastus medialis, Semitendinosus, Semimembranosus, Biceps femoris, Adductor magnus, Adductor longus, Adductor brevis, Pectineus, Iliacus, Psoas major, Psoas minor |
| Location | Hip and thigh region |
| Function | Hip flexion, extension, abduction, adduction, rotation, and stabilization |
| Nerve Supply | Sciatic nerve, Femoral nerve, Obturator nerve, Lumbar plexus |
| Blood Supply | Femoral artery, Popliteal artery, Deep femoral artery, Superficial femoral artery, Circumflex femoral artery, Medial femoral artery, Lateral femoral artery |
| Common Injuries | Strains, sprains, tendinitis, bursitis, dislocations, fractures, muscle tears, nerve entrapments |
| Treatment | Physical therapy, rest, ice, compression, elevation, anti-inflammatory medications, pain management, surgery (in severe cases) |
| Prevention | Proper warm-up and cool-down, stretching, strengthening exercises, maintaining good posture, avoiding overuse and repetitive motions |
| Rehabilitation | Gradual return to activity, range of motion exercises, muscle strengthening, balance and proprioception training, functional exercises |
| Associated Conditions | Arthritis, osteoporosis, tendinopathies, muscle imbalances, biomechanical dysfunctions |
| Special Considerations | Elderly individuals, athletes, individuals with pre-existing conditions, those who perform repetitive or high-impact activities |
Explore related products





What You'll Learn
- Muscle Groups Impacted: Identify specific muscles affected by glenohumeral dislocations, such as deltoids, pectoralis major, and rotator cuff muscles
- Symptoms and Signs: Describe common symptoms like pain, swelling, bruising, and limited range of motion in the shoulder area
- Causes and Risk Factors: Explain potential causes including trauma, falls, sports injuries, and predisposing conditions like joint laxity
- Diagnosis and Imaging: Outline diagnostic methods such as physical examination, X-rays, MRI, and CT scans to assess the extent of the dislocation
- Treatment Options: Discuss various treatment approaches including closed reduction, surgical intervention, immobilization, and physical therapy for rehabilitation
![]()
Muscle Groups Impacted: Identify specific muscles affected by glenohumeral dislocations, such as deltoids, pectoralis major, and rotator cuff muscles
Glenohumeral dislocations primarily impact the muscles surrounding the shoulder joint. The deltoid muscle, which is responsible for lifting the arm away from the body, is often affected due to its attachment to the humerus. The pectoralis major, a large muscle in the chest that assists in arm movement, can also be implicated in the dislocation process. Additionally, the rotator cuff muscles, a group of four muscles that stabilize the shoulder joint, are frequently injured during glenohumeral dislocations. These muscles include the supraspinatus, infraspinatus, teres minor, and subscapularis.
The mechanism of injury typically involves a forceful movement that pushes the humerus out of the glenoid cavity. This can occur in various directions, such as anteriorly or posteriorly, and the specific muscles affected may vary depending on the type of dislocation. For example, an anterior dislocation often impacts the posterior rotator cuff muscles, while a posterior dislocation may affect the anterior rotator cuff muscles.
In addition to the primary muscles mentioned, secondary muscles such as the trapezius, rhomboids, and serratus anterior may also be affected due to their role in shoulder stabilization and movement. These muscles work in conjunction with the primary muscles to maintain proper shoulder function and alignment.
Rehabilitation for glenohumeral dislocations often focuses on strengthening the affected muscles and improving joint stability. Physical therapy exercises may include resistance training, stretching, and proprioceptive activities to help restore normal shoulder function. It is essential to address the specific muscles impacted by the dislocation to ensure a comprehensive and effective rehabilitation program.
In conclusion, glenohumeral dislocations can have a significant impact on the muscles surrounding the shoulder joint. Understanding the specific muscles affected and their roles in shoulder function is crucial for developing an appropriate treatment and rehabilitation plan. By focusing on strengthening and stabilizing these muscles, individuals can improve their shoulder function and reduce the risk of future dislocations.
Understanding Cerebral Palsy's Impact on Children's Muscle Tone
You may want to see also
Explore related products






![]()
Symptoms and Signs: Describe common symptoms like pain, swelling, bruising, and limited range of motion in the shoulder area
Individuals experiencing a glenohumeral dislocation often present with a constellation of symptoms that can significantly impact their daily activities. One of the primary symptoms is intense pain in the shoulder area, which can radiate to the arm and even the neck. This pain is typically exacerbated by movement and can be severe enough to limit the individual's ability to perform even simple tasks.
Swelling is another common symptom, often accompanied by bruising. The swelling can be localized to the shoulder joint or extend down the arm, and it may take several days to subside. Bruising, on the other hand, can appear in various shades of blue, purple, and yellow, indicating the progression of the injury over time. The bruising may be more pronounced in cases where the dislocation was caused by a high-impact trauma.
Limited range of motion is a significant symptom that can persist even after the initial pain and swelling have subsided. Individuals may find it difficult to raise their arm above their head, rotate their shoulder, or reach behind their back. This limitation can be particularly challenging for those who require full use of their shoulder for work or daily activities.
In addition to these primary symptoms, individuals may also experience muscle spasms, tingling or numbness in the arm, and a general sense of weakness in the shoulder area. These symptoms can further complicate the recovery process and may require additional medical intervention to manage.
It is essential for individuals experiencing these symptoms to seek medical attention promptly, as a glenohumeral dislocation can lead to more severe complications if left untreated. A healthcare professional can provide a proper diagnosis and develop a treatment plan that addresses the specific needs of the individual, helping them to regain full function and mobility in their shoulder.
Exploring the Impact of Advil on Muscle Recovery: What You Need to Know
You may want to see also
Explore related products






![]()
Causes and Risk Factors: Explain potential causes including trauma, falls, sports injuries, and predisposing conditions like joint laxity
Glenohumeral dislocations, commonly referred to as shoulder dislocations, occur when the head of the upper arm bone (humerus) is forced out of the shoulder socket (glenoid). This injury can be caused by various factors, including trauma, falls, sports injuries, and predisposing conditions like joint laxity.
Trauma is a significant cause of glenohumeral dislocations. This can include direct blows to the shoulder, such as those experienced in car accidents or physical altercations. The force of the impact can disrupt the normal alignment of the shoulder joint, leading to dislocation.
Falls are another common cause, particularly among older adults and individuals with osteoporosis. When someone falls onto an outstretched hand or arm, the force can travel up the arm and dislocate the shoulder. This is often seen in elderly individuals who fall from a standing position or from a height, such as a step or a curb.
Sports injuries also contribute to the incidence of glenohumeral dislocations. Contact sports like football, hockey, and rugby pose a high risk due to the physical nature of the game. Non-contact sports like gymnastics, swimming, and tennis can also lead to dislocations, especially if the athlete performs repetitive overhead movements or experiences a sudden, forceful impact.
Predisposing conditions like joint laxity can increase the likelihood of a glenohumeral dislocation. Joint laxity refers to the looseness of the ligaments and tendons that hold the shoulder joint together. Individuals with joint laxity may have a higher risk of dislocation because their shoulder joint is less stable and more prone to injury.
In summary, glenohumeral dislocations can be caused by a variety of factors, including trauma, falls, sports injuries, and predisposing conditions like joint laxity. Understanding these causes and risk factors can help individuals take preventive measures to reduce their risk of experiencing this painful and debilitating injury.
Exploring the Connection: Muscle Soreness and Its Impact on Weight
You may want to see also
Explore related products






![]()
Diagnosis and Imaging: Outline diagnostic methods such as physical examination, X-rays, MRI, and CT scans to assess the extent of the dislocation
A glenohumeral dislocation, commonly referred to as a shoulder dislocation, occurs when the head of the upper arm bone (humerus) is forced out of the shoulder socket (glenoid). This injury can be extremely painful and may result in significant disability if not properly treated. Diagnosis of a glenohumeral dislocation typically involves a combination of physical examination and imaging studies.
The initial assessment of a potential shoulder dislocation begins with a thorough physical examination. The healthcare provider will carefully inspect the shoulder for signs of deformity, swelling, and bruising. They will also palpate the shoulder joint to assess for tenderness and instability. In some cases, the provider may perform specific maneuvers, such as the apprehension test, to help confirm the diagnosis.
X-rays are often the first imaging study ordered to evaluate a suspected shoulder dislocation. They provide a clear view of the bones in the shoulder joint and can help identify any fractures or dislocations. In particular, an anteroposterior (AP) view of the shoulder is useful for visualizing the alignment of the humeral head and the glenoid cavity.
While X-rays are helpful in diagnosing a shoulder dislocation, they may not provide enough detail to assess the extent of the injury or to identify any associated soft tissue damage. In such cases, more advanced imaging studies, such as magnetic resonance imaging (MRI) or computed tomography (CT) scans, may be necessary. MRI is particularly useful for evaluating the soft tissues surrounding the shoulder joint, including the muscles, tendons, and ligaments. CT scans, on the other hand, provide a more detailed view of the bones and can help identify any fractures or other abnormalities that may not be visible on X-rays.
In addition to imaging studies, other diagnostic tests may be ordered to help assess the extent of the injury. For example, a nerve conduction study may be performed to evaluate the function of the nerves in the shoulder and arm. This test can help identify any nerve damage that may have occurred as a result of the dislocation.
Once a diagnosis of a glenohumeral dislocation has been confirmed, treatment typically involves a combination of pain management, immobilization, and physical therapy. In some cases, surgery may be necessary to repair any associated fractures or soft tissue damage. Early and accurate diagnosis is critical to ensure the best possible outcome for patients with this type of injury.
Estrogen's Impact on Pelvic Muscle Tone: A Comprehensive Guide
You may want to see also
Explore related products






![]()
Treatment Options: Discuss various treatment approaches including closed reduction, surgical intervention, immobilization, and physical therapy for rehabilitation
Closed reduction is often the first-line treatment for glenohumeral dislocations, particularly for younger patients and those without significant trauma. This non-surgical procedure involves manually repositioning the humeral head back into the glenoid socket under sedation or anesthesia. It is typically performed in an emergency room or outpatient setting and can be successful in relieving pain and restoring function. However, closed reduction may not be suitable for all patients, especially those with recurrent dislocations or associated fractures.
Surgical intervention may be necessary for patients with recurrent glenohumeral dislocations or those with significant trauma that has damaged the surrounding soft tissues or bones. Procedures such as arthroscopic repair or open surgery can be used to address the underlying issues and stabilize the joint. Surgery is often followed by a period of immobilization to allow the joint to heal properly. The choice of surgical procedure depends on the individual patient's condition and the extent of the damage.
Immobilization is a crucial component of the treatment plan for glenohumeral dislocations, regardless of whether a closed reduction or surgical intervention is performed. The joint is typically immobilized using a sling or cast to prevent further injury and allow the soft tissues to heal. The duration of immobilization varies depending on the severity of the dislocation and the patient's overall health, but it usually lasts for several weeks. During this time, patients are advised to avoid activities that put stress on the shoulder joint.
Physical therapy plays a vital role in the rehabilitation process for patients with glenohumeral dislocations. Once the joint has healed sufficiently, physical therapists work with patients to restore strength, flexibility, and range of motion. This involves a series of exercises and stretches that are tailored to the individual patient's needs and abilities. Physical therapy can help patients regain function and reduce the risk of future dislocations. It is important for patients to follow their therapist's instructions and attend regular sessions to achieve optimal results.
Understanding Seizures: Types That Impact Muscle Function
You may want to see also
Frequently asked questions
The muscles commonly affected by a glenohumeral dislocation include the deltoid, pectoralis major, latissimus dorsi, teres major, and the rotator cuff muscles (supraspinatus, infraspinatus, teres minor, and subscapularis).
A glenohumeral dislocation can lead to significant impairment in shoulder function. The displacement of the humeral head from the glenoid cavity can stretch or tear the surrounding muscles and ligaments, resulting in pain, weakness, and limited range of motion. The affected muscles may also experience spasms or atrophy due to disuse following the injury.
Typical symptoms of a glenohumeral dislocation involving the shoulder muscles include severe pain, swelling, bruising, and a visible deformity of the shoulder. Patients may also experience muscle weakness, numbness or tingling in the arm, and difficulty moving the shoulder or arm. In some cases, there may be a popping or grinding sensation at the time of the injury.