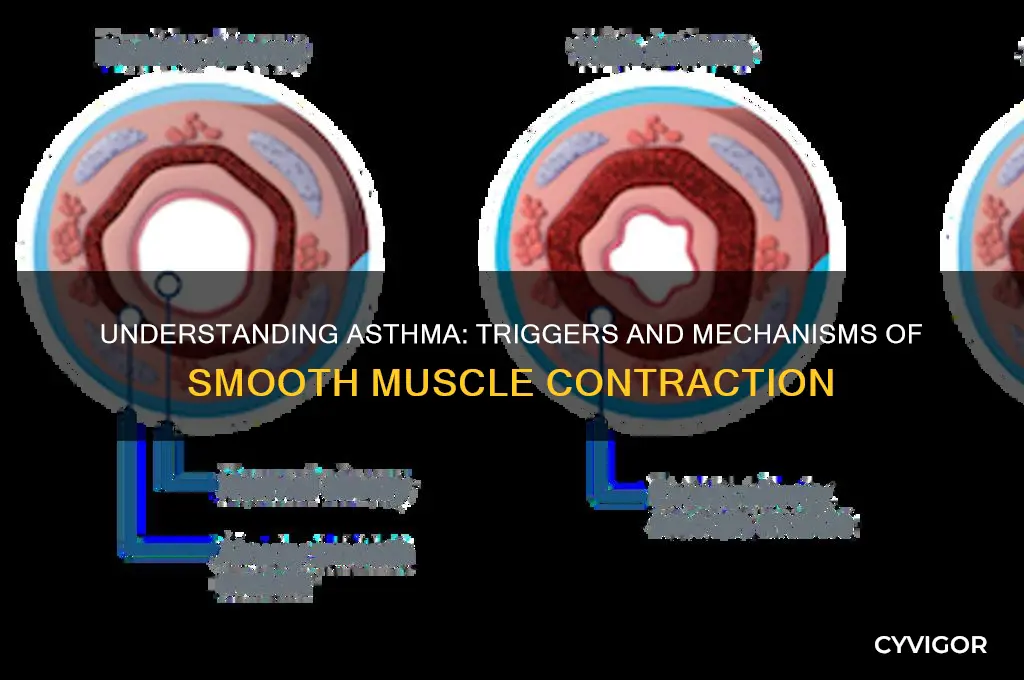
Smooth muscle contraction in asthma is primarily driven by a complex interplay of inflammatory mediators, neural mechanisms, and pharmacological factors. During an asthma attack, exposure to allergens or irritants triggers the release of inflammatory cytokines and leukotrienes from immune cells, such as mast cells and eosinophils, which stimulate bronchial smooth muscle cells to contract. Additionally, parasympathetic nerve activation leads to the release of acetylcholine, binding to muscarinic receptors on smooth muscle and inducing contraction via the IP3/DAG signaling pathway. Elevated intracellular calcium levels, facilitated by calcium release from the sarcoplasmic reticulum and influx through voltage-gated channels, activate calmodulin and myosin light chain kinase, promoting cross-bridge cycling and muscle shortening. These mechanisms collectively contribute to bronchoconstriction, airway narrowing, and the characteristic symptoms of asthma.
| Characteristics | Values |
|---|---|
| Primary Cause | Release of inflammatory mediators (e.g., histamine, leukotrienes, prostaglandins) from immune cells (mast cells, eosinophils) in response to allergens or triggers. |
| Key Mediators | Histamine, leukotrienes (LTC4, LTD4, LTE4), prostaglandin D2 (PGD2), thromboxane A2 (TXA2), and cytokines (IL-4, IL-5, IL-13). |
| Receptor Activation | Binding of mediators to receptors on smooth muscle cells (e.g., histamine to H1 receptors, leukotrienes to CysLT1 receptors) triggers intracellular signaling pathways. |
| Intracellular Signaling | Activation of G-proteins, phospholipase C (PLC), and inositol trisphosphate (IP3), leading to calcium release from the sarcoplasmic reticulum and calcium influx via voltage-gated channels. |
| Calcium Role | Increased intracellular calcium binds to calmodulin, activating myosin light chain kinase (MLCK), which phosphorylates myosin light chains, enabling actin-myosin interaction and muscle contraction. |
| Role of Rho-Kinase Pathway | Rho-kinase activation leads to phosphorylation of myosin light chains independently of calcium, contributing to sustained muscle contraction. |
| Inflammatory Cells Involved | Mast cells, eosinophils, T lymphocytes, and macrophages release mediators that enhance smooth muscle contraction and airway inflammation. |
| Airway Hyperresponsiveness | Chronic inflammation leads to increased sensitivity of smooth muscle to contractile agonists, even at low concentrations. |
| Structural Changes | Airway remodeling, including smooth muscle hypertrophy and hyperplasia, exacerbates contraction and airway narrowing. |
| Neurogenic Factors | Activation of sensory nerves releasing neuropeptides (e.g., substance P, neurokinin A) can potentiate smooth muscle contraction. |
| Environmental Triggers | Allergens (pollen, dust mites), irritants (smoke, pollution), respiratory viruses, cold air, and exercise can induce mediator release and muscle contraction. |
| Pharmacological Targets | Bronchodilators (β2-agonists, anticholinergics) and anti-inflammatory drugs (corticosteroids, leukotriene modifiers) target these pathways to relieve contraction. |
Explore related products






What You'll Learn
- Role of bronchial hyperresponsiveness in airway smooth muscle contraction
- Impact of inflammatory mediators on smooth muscle constriction
- Effect of histamine release on airway smooth muscle
- Influence of cholinergic receptors in smooth muscle contraction
- Contribution of leukotrienes to airway smooth muscle narrowing
![]()
Role of bronchial hyperresponsiveness in airway smooth muscle contraction
Bronchial hyperresponsiveness (BHR) is a hallmark feature of asthma and plays a pivotal role in the excessive contraction of airway smooth muscle (ASM), a key driver of asthma symptoms. BHR refers to the exaggerated response of the airways to various stimuli, such as allergens, irritants, or pharmacological agents, resulting in ASM contraction and subsequent airway narrowing. This heightened sensitivity is central to understanding why asthmatic individuals experience bronchoconstriction even in response to mild triggers. The underlying mechanisms of BHR involve complex interactions between inflammatory cells, neural pathways, and structural changes in the airways, all of which contribute to the abnormal ASM behavior observed in asthma.
One of the primary mechanisms linking BHR to ASM contraction is the release of inflammatory mediators from immune cells, such as mast cells, eosinophils, and T-lymphocytes. In asthmatic airways, these cells are often activated by allergens or other triggers, leading to the secretion of pro-inflammatory cytokines (e.g., IL-4, IL-5, IL-13) and bronchoconstrictor substances (e.g., histamine, leukotrienes, prostaglandins). These mediators act directly or indirectly on ASM cells, enhancing their contractility. For instance, leukotrienes bind to specific receptors on ASM, triggering intracellular signaling pathways that promote calcium influx and actin-myosin cross-bridge formation, ultimately leading to muscle contraction. This inflammatory milieu not only amplifies the contractile response but also lowers the threshold for ASM activation, contributing to BHR.
Neural mechanisms also play a critical role in BHR and ASM contraction. The parasympathetic nervous system, in particular, is heavily involved, with vagal nerve stimulation releasing acetylcholine (ACh), a potent bronchoconstrictor. In asthmatic individuals, the airways exhibit increased sensitivity to ACh due to upregulation of muscarinic receptors on ASM cells. Additionally, neurogenic inflammation, where sensory nerves release neuropeptides like substance P and neurokinin A, further exacerbates ASM contraction by promoting inflammatory cell recruitment and mediator release. This neuro-immune crosstalk creates a feedback loop that sustains BHR and perpetuates ASM hypercontractility.
Structural changes in the airways, often referred to as airway remodeling, also contribute to BHR and ASM contraction in asthma. Chronic inflammation leads to thickening of the airway wall, increased deposition of extracellular matrix proteins, and hypertrophy or hyperplasia of ASM cells. These alterations enhance the mechanical ability of ASM to contract and reduce the compliance of the airway wall, making it more susceptible to narrowing. Furthermore, remodeling can disrupt the normal balance between contractile and relaxant signals, favoring a pro-contractile state. For example, reduced expression of β2-adrenergic receptors, which mediate bronchodilation, diminishes the effectiveness of endogenous or therapeutic relaxant stimuli, thereby amplifying BHR.
In summary, bronchial hyperresponsiveness is a multifaceted phenomenon that significantly contributes to airway smooth muscle contraction in asthma. Through the interplay of inflammatory mediators, neural pathways, and structural airway changes, BHR creates an environment where ASM cells are primed for excessive and inappropriate contraction. Understanding these mechanisms is crucial for developing targeted therapies that address not only the symptoms but also the underlying causes of asthma. By mitigating BHR, it may be possible to reduce the frequency and severity of ASM contractions, thereby improving airway function and quality of life for asthmatic individuals.
Understanding Depolarization Triggers in Cardiac Muscle Cell Contractions
You may want to see also
Explore related products





![]()
Impact of inflammatory mediators on smooth muscle constriction
In asthma, smooth muscle constriction is a key factor in the narrowing of airways, leading to breathing difficulties. Inflammatory mediators play a pivotal role in this process by directly and indirectly stimulating smooth muscle contraction. These mediators are released by various cells involved in the inflammatory response, such as mast cells, eosinophils, and T lymphocytes. One of the primary mediators is histamine, which is rapidly released by mast cells upon allergen exposure. Histamine binds to H1 receptors on smooth muscle cells, activating signaling pathways that increase intracellular calcium levels. This rise in calcium triggers muscle contraction by promoting the interaction between actin and myosin filaments, resulting in airway constriction.
Another critical inflammatory mediator is leukotriene, specifically LTC4, LTD4, and LTE4, which are potent bronchoconstrictors produced by mast cells and eosinophils. Leukotrienes bind to CysLT1 and CysLT2 receptors on smooth muscle cells, leading to calcium mobilization and subsequent muscle contraction. Unlike histamine, which acts rapidly but has a short duration, leukotrienes cause sustained smooth muscle constriction, contributing to prolonged airway narrowing in asthma. Additionally, leukotrienes enhance vascular permeability and mucus secretion, further exacerbating airway obstruction.
Prostaglandins, particularly PGD2, are also significant mediators in asthma-induced smooth muscle constriction. PGD2 is primarily synthesized by mast cells and acts via DP1 and DP2 receptors. Activation of DP1 receptors leads to relaxation, but DP2 receptor activation causes bronchoconstriction by increasing calcium influx and activating protein kinases. This dual role of prostaglandins highlights the complexity of inflammatory mediator effects on smooth muscle. Furthermore, PGD2 metabolites, such as 15-deoxy-Δ12,14-PGJ2, can also influence muscle tone by modulating intracellular signaling pathways.
Cytokines, such as interleukin-4 (IL-4), IL-5, and IL-13, produced by Th2 cells, indirectly contribute to smooth muscle constriction by amplifying the inflammatory response. IL-4 and IL-13 promote IgE production and eosinophil recruitment, while IL-5 activates and prolongs eosinophil survival. Eosinophils release mediators like major basic protein (MBP) and eosinophil peroxidase, which damage airway epithelium and enhance smooth muscle responsiveness to contractile agonists. This heightened sensitivity to mediators like histamine and leukotrienes further exacerbates muscle constriction.
Finally, thromboxane A2 (TXA2), produced by platelets and airway cells, is another potent bronchoconstrictor. TXA2 binds to TP receptors on smooth muscle cells, stimulating calcium release and muscle contraction. Its effects are particularly pronounced in severe asthma, where platelet activation and thromboxane production are elevated. Inhibiting thromboxane synthesis or blocking its receptors has been explored as a therapeutic strategy to reduce smooth muscle constriction in asthma. Collectively, these inflammatory mediators create a cascade of events that significantly impact airway smooth muscle tone, underscoring their central role in asthma pathophysiology.
Fever and Muscle Weakness: What's the Link?
You may want to see also
Explore related products





![]()
Effect of histamine release on airway smooth muscle
In asthma, smooth muscle contraction in the airways is a key factor leading to bronchoconstriction, airflow obstruction, and respiratory symptoms. One of the primary triggers for this contraction is the release of histamine, a potent inflammatory mediator. Histamine is released by mast cells and basophils in response to allergens or other stimuli, and it plays a central role in the pathophysiology of asthma. When histamine is released, it binds to specific receptors on airway smooth muscle cells, primarily the H1 receptors, initiating a cascade of events that result in muscle contraction.
The effect of histamine release on airway smooth muscle is multifaceted. Upon binding to H1 receptors, histamine activates phospholipase C, which leads to the production of inositol trisphosphate (IP3) and diacylglycerol (DAG). IP3 causes the release of calcium ions from intracellular stores, while DAG activates protein kinase C (PKC). The increase in intracellular calcium concentration triggers calcium to bind to calmodulin, which then activates myosin light-chain kinase (MLCK). MLCK phosphorylates the myosin light chains, allowing them to interact with actin filaments and initiate muscle contraction. This process is a direct mechanism by which histamine induces bronchoconstriction.
Additionally, histamine release contributes to airway smooth muscle contraction indirectly by enhancing inflammation and airway hyperresponsiveness. Histamine stimulates the production of pro-inflammatory cytokines and chemokines, which recruit and activate other immune cells, such as eosinophils and lymphocytes. This inflammatory milieu further sensitizes the airway smooth muscle to contractile agonists, amplifying the response to histamine and other stimuli. Moreover, histamine promotes the release of leukotrienes and prostaglandins from mast cells, which are additional potent bronchoconstrictors, creating a synergistic effect on airway smooth muscle contraction.
Another critical effect of histamine on airway smooth muscle is its role in airway remodeling, a chronic feature of asthma. Repeated or prolonged exposure to histamine can lead to structural changes in the airway wall, including smooth muscle cell proliferation and hypertrophy. This remodeling increases the mass of smooth muscle surrounding the airways, making them more susceptible to contraction and less responsive to bronchodilators. Histamine-induced remodeling is mediated through its effects on growth factors and cytokines, such as transforming growth factor-beta (TGF-β) and interleukin-13 (IL-13), which promote fibrosis and muscle cell growth.
In summary, the release of histamine has a profound effect on airway smooth muscle contraction in asthma through both direct and indirect mechanisms. Directly, histamine binds to H1 receptors and activates signaling pathways that increase intracellular calcium, leading to muscle contraction. Indirectly, histamine exacerbates inflammation, enhances airway hyperresponsiveness, and contributes to airway remodeling, all of which perpetuate and worsen bronchoconstriction. Understanding these effects is crucial for developing targeted therapies that can mitigate histamine-induced smooth muscle contraction and improve asthma management.
Tight Muscles and Erectile Dysfunction: What's the Link?
You may want to see also
Explore related products






![]()
Influence of cholinergic receptors in smooth muscle contraction
Smooth muscle contraction in asthma is a complex process involving multiple pathways, and one of the key players is the cholinergic system. Cholinergic receptors, specifically muscarinic receptors, play a significant role in regulating airway smooth muscle tone. When activated, these receptors initiate a cascade of intracellular events leading to muscle contraction, which is a hallmark of bronchoconstriction in asthma. The influence of cholinergic receptors on smooth muscle contraction is primarily mediated through the release of acetylcholine (ACh), a neurotransmitter that binds to muscarinic receptors on the smooth muscle cells. This interaction triggers a series of signaling events that ultimately result in calcium influx and muscle contraction.
Muscarinic receptors are G protein-coupled receptors (GPCRs) classified into five subtypes (M1–M5), with M2 and M3 receptors being the most relevant in airway smooth muscle. The M3 receptor is particularly important as it is coupled to the Gq protein, which activates phospholipase C (PLC). Upon ACh binding, PLC hydrolyzes phosphatidylinositol 4,5-bisphosphate (PIP2) into inositol trisphosphate (IP3) and diacylglycerol (DAG). IP3 then binds to its receptor on the sarcoplasmic reticulum, releasing stored calcium ions into the cytoplasm. This increase in intracellular calcium concentration activates calcium-calmodulin-dependent kinase II and myosin light chain kinase (MLCK), leading to phosphorylation of myosin light chains and subsequent smooth muscle contraction.
The M2 receptor, on the other hand, is coupled to the Gi protein and primarily acts to inhibit adenylate cyclase, reducing cyclic adenosine monophosphate (cAMP) levels. While M2 receptors are less directly involved in contraction, their activation can modulate the overall tone of the smooth muscle by counteracting the relaxing effects of beta-adrenergic stimulation. However, in asthma, the balance between M2 and M3 receptor activity is often disrupted, favoring excessive contraction due to heightened cholinergic tone and increased M3 receptor signaling.
Pharmacological interventions targeting cholinergic receptors have been developed to manage asthma symptoms. Anticholinergic drugs, such as ipratropium bromide, act as muscarinic receptor antagonists, primarily blocking M3 receptors. By inhibiting ACh-induced calcium mobilization and MLCK activation, these agents reduce smooth muscle contraction and alleviate bronchoconstriction. This highlights the critical influence of cholinergic receptors in mediating airway smooth muscle hyperresponsiveness in asthma.
In summary, cholinergic receptors, particularly muscarinic M3 receptors, are central to smooth muscle contraction in asthma. Their activation by ACh initiates signaling pathways that increase intracellular calcium and activate contractile proteins. Understanding the role of these receptors has led to the development of effective anticholinergic therapies, underscoring their significance in both the pathophysiology and treatment of asthma-related bronchoconstriction.
Can PMS Cause Muscle Weakness? Understanding the Link and Symptoms
You may want to see also
Explore related products






![]()
Contribution of leukotrienes to airway smooth muscle narrowing
Leukotrienes are potent lipid mediators derived from arachidonic acid metabolism, primarily through the 5-lipoxygenase pathway. They play a significant role in the pathophysiology of asthma, particularly in the context of airway smooth muscle (ASM) narrowing. Among the various leukotrienes, cysteinyl leukotrienes (CysLTs), including LTC4, LTD4, and LTE4, are the most implicated in asthma. These mediators are released by activated inflammatory cells such as mast cells, eosinophils, and macrophages in response to allergic or inflammatory stimuli. Once released, CysLTs bind to specific receptors (CysLT1 and CysLT2) expressed on ASM cells, triggering a cascade of intracellular events that lead to muscle contraction.
The binding of CysLTs to their receptors activates G-protein-coupled signaling pathways, which in turn stimulate the phosphorylation of myosin light chains (MLC) via the calcium-calmodulin-dependent pathway. This phosphorylation is a critical step in the contraction of ASM, as it allows actin and myosin filaments to interact, generating force and shortening the muscle fibers. Additionally, leukotrienes enhance calcium influx into ASM cells, further promoting contraction. The sustained activation of these pathways by leukotrienes contributes to the excessive and prolonged ASM narrowing observed in asthma, leading to bronchoconstriction and airway hyperresponsiveness.
Beyond their direct effects on ASM contraction, leukotrienes also contribute to airway narrowing indirectly by promoting inflammation and remodeling. CysLTs increase vascular permeability, leading to plasma exudation and mucous secretion, which further narrow the airway lumen. They also stimulate the proliferation of ASM cells and the deposition of extracellular matrix proteins, contributing to airway wall thickening and remodeling over time. This dual role of leukotrienes—both as direct bronchoconstrictors and as promoters of airway inflammation and remodeling—makes them key contributors to the chronicity and severity of asthma.
Pharmacological interventions targeting leukotrienes have been developed to mitigate their effects on ASM narrowing. Leukotriene receptor antagonists (e.g., montelukast, zafirlukast) and 5-lipoxygenase inhibitors (e.g., zileuton) are commonly used in asthma management. These medications reduce ASM contraction by blocking the binding of CysLTs to their receptors or by inhibiting their synthesis, respectively. Clinical studies have demonstrated their efficacy in improving lung function, reducing asthma symptoms, and preventing exercise-induced bronchoconstriction, highlighting the critical role of leukotrienes in ASM narrowing.
In summary, leukotrienes, particularly cysteinyl leukotrienes, are major contributors to airway smooth muscle narrowing in asthma. Their direct effects on ASM contraction, mediated through receptor-activated signaling pathways, and their indirect effects on airway inflammation and remodeling, collectively exacerbate bronchoconstriction and airway hyperresponsiveness. Targeting leukotrienes with specific antagonists or inhibitors has proven to be an effective therapeutic strategy in asthma management, underscoring their central role in the disease’s pathophysiology. Understanding the mechanisms by which leukotrienes contribute to ASM narrowing is essential for developing more effective treatments for asthma.
Sore Abdominal Muscles and Nausea: Understanding the Surprising Connection
You may want to see also
Frequently asked questions
The primary cause is the release of inflammatory mediators, such as histamine, leukotrienes, and prostaglandins, which activate receptors on smooth muscle cells, leading to bronchoconstriction.
Allergens stimulate the release of IgE antibodies, which bind to mast cells. This triggers the release of inflammatory mediators like histamine, causing smooth muscle contraction and airway narrowing.
The parasympathetic nervous system releases acetylcholine, which binds to muscarinic receptors on smooth muscle cells, leading to increased intracellular calcium and subsequent muscle contraction.
Yes, airway inflammation releases cytokines and chemokines that enhance smooth muscle responsiveness to contractile stimuli, making it more prone to bronchoconstriction even with minimal triggers.































