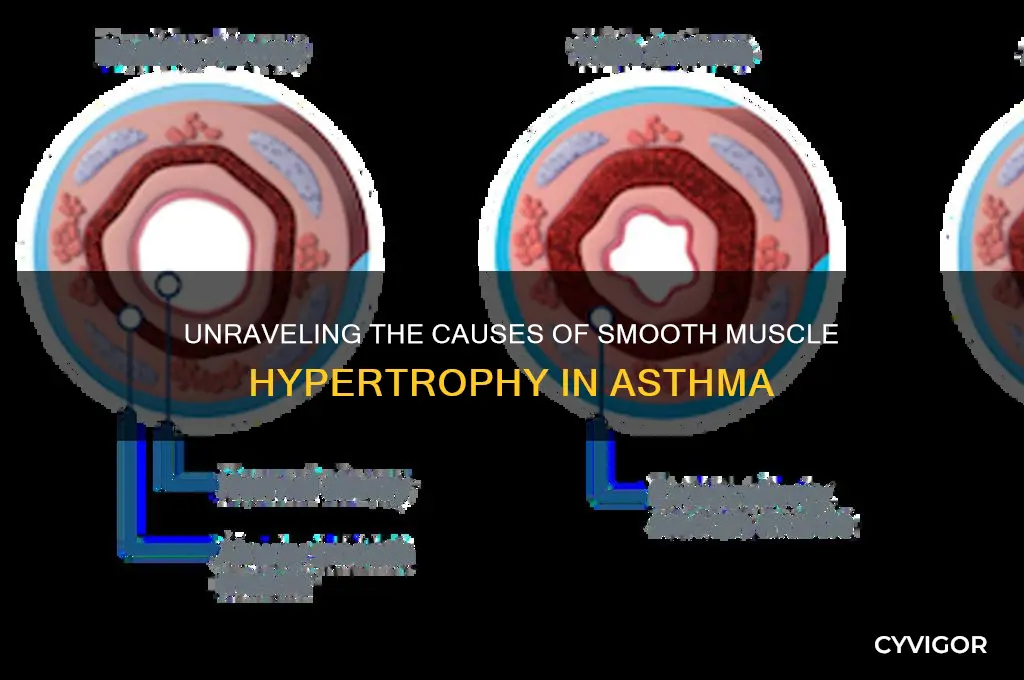
Smooth muscle hypertrophy in asthma is primarily driven by chronic airway inflammation and remodeling, which are hallmark features of the disease. Inflammatory mediators, such as cytokines (e.g., IL-4, IL-5, IL-13) and growth factors (e.g., TGF-β, PDGF), released by immune cells and structural cells in the airways, stimulate smooth muscle cell proliferation and enlargement. Additionally, repeated exposure to allergens, irritants, and bronchoconstrictors leads to sustained smooth muscle contraction, which over time contributes to muscle cell hypertrophy. Oxidative stress and mechanical stress from airway hyperresponsiveness further exacerbate this process, promoting the accumulation of contractile proteins and extracellular matrix components. These mechanisms collectively result in thickened airway walls, increased smooth muscle mass, and impaired lung function, contributing to the severity and persistence of asthma symptoms.
| Characteristics | Values |
|---|---|
| Inflammatory Mediators | Cytokines (e.g., IL-4, IL-5, IL-13), chemokines, and growth factors promote smooth muscle cell proliferation and hypertrophy. |
| Airway Hyperresponsiveness | Increased sensitivity of smooth muscle to contractile agonists (e.g., histamine, acetylcholine). |
| Oxidative Stress | Elevated levels of reactive oxygen species (ROS) contribute to muscle cell growth and remodeling. |
| Growth Factors | Transforming growth factor-β (TGF-β), platelet-derived growth factor (PDGF), and fibroblast growth factor (FGF) stimulate hypertrophy. |
| Mechanical Stress | Chronic airway obstruction and increased wall tension lead to muscle cell adaptation and growth. |
| Genetic Predisposition | Polymorphisms in genes related to muscle contraction and inflammation (e.g., ADAM33, MMPs) may increase susceptibility. |
| Chronic Airway Inflammation | Persistent inflammation leads to remodeling, including smooth muscle hypertrophy. |
| Airway Remodeling | Structural changes in the airway wall, including smooth muscle thickening, are hallmarks of severe asthma. |
| Neurogenic Factors | Increased neural activity and neuropeptides (e.g., substance P) contribute to muscle cell proliferation. |
| Matrix Metalloproteinases (MMPs) | Elevated MMP activity is associated with airway remodeling and smooth muscle hypertrophy. |
| Epithelial-Mesenchymal Transition (EMT) | EMT contributes to the accumulation of mesenchymal cells, including smooth muscle cells. |
| Corticosteroid Resistance | In some cases, smooth muscle cells become resistant to anti-inflammatory effects of corticosteroids, promoting hypertrophy. |
Explore related products






What You'll Learn
- Airway inflammation role: Chronic inflammation triggers smooth muscle growth in asthma
- Cytokine influence: Pro-inflammatory cytokines like IL-13 promote muscle hypertrophy
- Mechanical stress effect: Repeated bronchoconstriction induces muscle cell enlargement
- Remodeling process: Asthma-related airway remodeling includes smooth muscle thickening
- Genetic predisposition: Certain genes may increase susceptibility to muscle hypertrophy
![]()
Airway inflammation role: Chronic inflammation triggers smooth muscle growth in asthma
Chronic airway inflammation plays a pivotal role in the development and progression of smooth muscle hypertrophy in asthma. In asthmatic individuals, the airways are persistently inflamed due to an aberrant immune response to allergens, irritants, or other triggers. This inflammation is characterized by the infiltration of immune cells, such as eosinophils, lymphocytes, and mast cells, which release a cascade of pro-inflammatory cytokines, chemokines, and growth factors. These mediators create a microenvironment that not only sustains inflammation but also directly and indirectly promotes the growth and remodeling of airway smooth muscle (ASM) cells. Key cytokines like interleukin-4 (IL-4), IL-5, IL-13, and tumor necrosis factor-alpha (TNF-α) are particularly implicated in this process, as they activate signaling pathways that drive ASM cell proliferation and hypertrophy.
One of the primary mechanisms by which chronic inflammation triggers smooth muscle growth is through the activation of growth factors and receptors. Transforming growth factor-beta (TGF-β), for instance, is upregulated in the inflamed asthmatic airway and is a potent stimulator of ASM cell proliferation and extracellular matrix deposition. TGF-β binds to its receptors on ASM cells, initiating intracellular signaling cascades such as the Smad pathway, which promotes cell growth and protein synthesis. Similarly, platelet-derived growth factor (PDGF) and epidermal growth factor (EGF) are also elevated in asthmatic airways and contribute to ASM hypertrophy by enhancing cell division and survival. These growth factors are often overexpressed in response to chronic inflammation, creating a feedback loop that exacerbates smooth muscle remodeling.
Inflammatory mediators also induce oxidative stress and airway hyperresponsiveness, which further contribute to ASM hypertrophy. Reactive oxygen species (ROS) produced during inflammation can activate transcription factors like nuclear factor-kappa B (NF-κB) and activator protein-1 (AP-1), which upregulate genes involved in cell growth and inflammation. Additionally, chronic inflammation leads to the release of thrombin and endothelin-1, which bind to specific receptors on ASM cells and stimulate hypertrophic responses. This interplay between inflammation and oxidative stress creates a milieu that fosters abnormal smooth muscle growth, leading to airway wall thickening and reduced lung function in asthma.
Another critical aspect of airway inflammation in ASM hypertrophy is the role of cytokines in altering the phenotype of ASM cells. Under the influence of inflammatory mediators, ASM cells undergo a phenotypic shift, becoming more proliferative, synthetic, and contractile. This change is marked by increased expression of contractile proteins like α-smooth muscle actin and enhanced synthesis of cytokines and chemokines, further perpetuating inflammation. The cross-talk between inflammatory cells and ASM cells amplifies the remodeling process, as ASM cells themselves contribute to the inflammatory environment by secreting cytokines and recruiting immune cells. This bidirectional relationship underscores the central role of chronic inflammation in driving smooth muscle hypertrophy.
Finally, the chronicity of inflammation in asthma ensures a sustained stimulus for ASM growth and remodeling. Unlike acute inflammation, which resolves over time, chronic inflammation in asthma persists due to ongoing exposure to triggers and an imbalanced immune response. This prolonged inflammatory state leads to irreversible structural changes in the airways, including ASM hypertrophy, hyperplasia, and fibrosis. These changes not only increase airway resistance and bronchial hyperresponsiveness but also reduce the efficacy of bronchodilators, making asthma more difficult to control. Thus, targeting airway inflammation remains a cornerstone in preventing and managing smooth muscle hypertrophy in asthma, highlighting its critical role in disease pathogenesis.
Eggs and Muscle Aches: What's the Connection?
You may want to see also
Explore related products






![]()
Cytokine influence: Pro-inflammatory cytokines like IL-13 promote muscle hypertrophy
In the context of asthma, smooth muscle hypertrophy is a significant contributor to airway remodeling and hyperresponsiveness. Among the various factors implicated in this process, cytokine influence plays a pivotal role, particularly pro-inflammatory cytokines like interleukin-13 (IL-13). IL-13 is a key mediator in the Th2-driven immune response, which is characteristic of allergic asthma. This cytokine is produced by activated T lymphocytes, mast cells, and innate lymphoid cells (ILC2s) in response to allergen exposure. Once released, IL-13 binds to its receptors on airway smooth muscle (ASM) cells, initiating a cascade of intracellular signaling events that ultimately lead to muscle hypertrophy.
The mechanism by which IL-13 promotes ASM hypertrophy involves the activation of signal transducer and activator of transcription 6 (STAT6) and subsequent upregulation of genes associated with muscle growth. Upon binding to its receptor complex, IL-13 triggers phosphorylation of STAT6, which then dimerizes and translocates to the nucleus. Here, STAT6 binds to specific DNA response elements, promoting the transcription of genes such as *Clca1* and *Gob5*, as well as those involved in muscle cell proliferation and differentiation. Additionally, IL-13 stimulates the production of extracellular matrix (ECM) components, further contributing to the structural changes observed in hypertrophic ASM.
Another critical aspect of IL-13’s influence is its ability to enhance the expression of mitogens and growth factors, such as transforming growth factor-β (TGF-β) and fibroblast growth factor (FGF). These factors create a pro-proliferative microenvironment, encouraging ASM cells to enter the cell cycle and increase in size and number. IL-13 also suppresses the expression of muscle-specific proteins that maintain ASM contractility, leading to a phenotype characterized by increased mass and reduced functionality. This imbalance between muscle growth and contractile efficiency exacerbates airway narrowing and hyperresponsiveness, hallmark features of asthma.
Furthermore, IL-13-induced ASM hypertrophy is closely linked to epithelial-mesenchymal trophic unit (EMT) dysregulation. In asthmatic airways, IL-13 disrupts the normal epithelial barrier, leading to the release of alarmins like IL-25, IL-33, and thymic stromal lymphopoietin (TSLP). These alarmins, in turn, amplify the Th2 immune response, creating a feed-forward loop that sustains IL-13 production and perpetuates ASM hypertrophy. This interplay between epithelial damage, cytokine release, and smooth muscle remodeling underscores the complexity of IL-13’s role in asthma pathogenesis.
Therapeutically, targeting IL-13 signaling has emerged as a promising strategy to mitigate ASM hypertrophy in asthma. Monoclonal antibodies such as lebrikizumab and tralokinumab, which specifically neutralize IL-13, have shown potential in reducing airway inflammation and remodeling in clinical trials. By inhibiting IL-13-mediated STAT6 activation and downstream effects, these biologics aim to restore normal ASM function and alleviate asthma symptoms. Understanding the precise mechanisms by which IL-13 drives muscle hypertrophy not only advances our knowledge of asthma pathobiology but also informs the development of more effective treatments for this chronic respiratory condition.
Plaquenil Side Effects: Understanding Muscle Weakness and Potential Risks
You may want to see also
Explore related products





![]()
Mechanical stress effect: Repeated bronchoconstriction induces muscle cell enlargement
In the context of asthma, smooth muscle hypertrophy is a significant contributor to airway remodeling and hyperresponsiveness. One of the primary mechanisms driving this process is the mechanical stress effect, where repeated episodes of bronchoconstriction lead to muscle cell enlargement. During an asthma exacerbation, the bronchial smooth muscles contract excessively, causing narrowing of the airways. This repeated contraction, or bronchoconstriction, imposes mechanical stress on the muscle cells, triggering a cascade of cellular responses that ultimately result in hypertrophy. The stress is not merely a consequence of the contraction itself but also stems from the increased resistance and friction within the airway lumen during these episodes.
Mechanical stress activates various intracellular signaling pathways that promote muscle cell growth. One key pathway involves the mechanosensitive ion channels and integrins on the cell membrane, which detect changes in mechanical tension. When activated, these channels initiate signaling cascades, including the mitogen-activated protein kinase (MAPK) and phosphatidylinositol 3-kinase (PI3K) pathways. These pathways stimulate protein synthesis and inhibit protein degradation, leading to an increase in cell size and mass. Additionally, mechanical stress enhances the expression of growth factors such as transforming growth factor-β (TGF-β) and platelet-derived growth factor (PDGF), which further contribute to muscle cell proliferation and hypertrophy.
Repeated bronchoconstriction also induces inflammation, which synergistically amplifies the mechanical stress effect. Inflammatory cells release cytokines and chemokines that activate smooth muscle cells, making them more responsive to mechanical stimuli. For instance, interleukin-13 (IL-13) and interleukin-4 (IL-4), which are elevated in asthmatic airways, promote smooth muscle cell hypertrophy by upregulating the expression of contractile proteins and enhancing cell survival. This interplay between mechanical stress and inflammation creates a vicious cycle, where each exacerbation further predisposes the airways to future episodes of bronchoconstriction and muscle hypertrophy.
Another critical aspect of the mechanical stress effect is the role of extracellular matrix (ECM) remodeling. Repeated bronchoconstriction alters the composition and stiffness of the ECM surrounding the smooth muscle cells. This increased stiffness provides a chronic mechanical stimulus, even in the absence of active contraction, perpetuating the hypertrophic response. Furthermore, ECM proteins such as fibronectin and collagen interact with integrins on the muscle cell surface, activating signaling pathways that drive cell growth and differentiation. Thus, ECM remodeling acts as both a consequence and a driver of smooth muscle hypertrophy in asthma.
In summary, the mechanical stress effect resulting from repeated bronchoconstriction is a major driver of smooth muscle hypertrophy in asthma. This process involves the activation of mechanosensitive signaling pathways, the release of growth factors, the interplay with airway inflammation, and ECM remodeling. Understanding these mechanisms is crucial for developing targeted therapies aimed at preventing or reversing airway smooth muscle hypertrophy, thereby improving asthma management and outcomes.
Understanding Underarm and Muscle Knots: Causes and Effective Remedies
You may want to see also
Explore related products






![]()
Remodeling process: Asthma-related airway remodeling includes smooth muscle thickening
The remodeling process in asthma is a complex and dynamic phenomenon, characterized by structural changes in the airways that contribute to the chronic nature of the disease. One of the key features of asthma-related airway remodeling is smooth muscle thickening, which plays a significant role in the development of airway hyperresponsiveness and fixed airflow obstruction. This process is driven by a combination of factors, including inflammation, oxidative stress, and growth factor activation, ultimately leading to smooth muscle cell hypertrophy and hyperplasia.
In asthma, chronic inflammation leads to the release of various cytokines and chemokines, such as interleukin-4 (IL-4), IL-5, IL-13, and tumor necrosis factor-alpha (TNF-α), which stimulate the proliferation and differentiation of smooth muscle cells. These inflammatory mediators activate signaling pathways, including the mitogen-activated protein kinase (MAPK) and phosphoinositide 3-kinase (PI3K) pathways, promoting cell growth and survival. Additionally, oxidative stress, resulting from an imbalance between reactive oxygen species (ROS) production and antioxidant defenses, further contributes to smooth muscle cell hypertrophy by inducing DNA damage, cellular senescence, and altered gene expression.
Growth factors, such as transforming growth factor-beta (TGF-β), platelet-derived growth factor (PDGF), and fibroblast growth factor (FGF), also play a crucial role in asthma-related smooth muscle thickening. These factors stimulate smooth muscle cell proliferation, migration, and extracellular matrix (ECM) production, leading to increased airway wall thickness and reduced airway caliber. TGF-β, in particular, has been implicated in the development of airway fibrosis, a hallmark of severe asthma, by promoting the differentiation of fibroblasts into myofibroblasts and increasing ECM deposition.
The process of smooth muscle thickening in asthma is further exacerbated by the interaction between smooth muscle cells and other airway structural cells, including epithelial cells, fibroblasts, and immune cells. Epithelial-mesenchymal interactions, mediated by gap junctions and paracrine signaling, contribute to the coordinated response of airway cells to inflammatory stimuli, leading to altered smooth muscle cell behavior and increased contractility. Moreover, the release of matricellular proteins, such as osteopontin and tenascin-C, by smooth muscle cells and other airway cells, modulates cell-matrix interactions and influences smooth muscle cell proliferation and migration.
As smooth muscle thickening progresses, it leads to a range of functional and structural consequences, including increased airway resistance, reduced lung function, and fixed airflow obstruction. The thickened smooth muscle layer contributes to airway hyperresponsiveness, a hallmark of asthma, by increasing the sensitivity of the airways to various stimuli, such as allergens, irritants, and cholinergic agonists. Furthermore, the altered mechanical properties of the airway wall, resulting from smooth muscle thickening and ECM remodeling, impair airway distensibility and contribute to the development of irreversible airflow obstruction in severe asthma. Understanding the complex interplay between inflammation, growth factor activation, and cellular interactions in the remodeling process is essential for developing targeted therapies to prevent or reverse smooth muscle thickening in asthma.
The development of novel therapeutic strategies aimed at modulating smooth muscle cell behavior and reducing airway remodeling is an active area of research in asthma. Targeting specific signaling pathways, such as TGF-β or PDGF signaling, or inhibiting matricellular protein function may offer promising approaches to attenuate smooth muscle thickening and improve asthma outcomes. Additionally, interventions aimed at reducing oxidative stress, inflammation, or epithelial-mesenchymal interactions may help to preserve airway structure and function in asthmatic individuals. By elucidating the underlying mechanisms driving smooth muscle hypertrophy in asthma, researchers can identify new targets for therapeutic intervention and ultimately improve the management of this complex and debilitating disease.
Leg Muscle Pain: Causes and Triggers
You may want to see also
Explore related products





![]()
Genetic predisposition: Certain genes may increase susceptibility to muscle hypertrophy
Genetic predisposition plays a significant role in the development of smooth muscle hypertrophy in asthma, as certain genetic variations can increase an individual’s susceptibility to this condition. Research has identified specific genes associated with airway smooth muscle (ASM) remodeling, a key feature of asthma pathophysiology. For instance, polymorphisms in genes encoding cytokines, growth factors, and receptors involved in muscle cell proliferation and contraction have been linked to ASM hypertrophy. These genetic variants can alter the expression or function of proteins critical for maintaining ASM homeostasis, leading to excessive muscle growth and airway hyperresponsiveness. Understanding these genetic factors is essential for identifying individuals at higher risk and developing targeted therapies.
One of the most studied genetic factors in asthma-related smooth muscle hypertrophy is the role of transforming growth factor-beta (TGF-β) and its signaling pathway. TGF-β is a potent stimulator of ASM cell proliferation and extracellular matrix deposition, both of which contribute to muscle hypertrophy. Genetic variations in the *TGFB1* gene, which encodes TGF-β, have been associated with increased ASM mass in asthmatic patients. Additionally, mutations in genes involved in the TGF-β signaling cascade, such as *SMAD3*, can enhance the responsiveness of ASM cells to TGF-β, further promoting hypertrophy. These genetic predispositions highlight the importance of growth factor pathways in the development of ASM remodeling.
Another genetic factor contributing to smooth muscle hypertrophy in asthma is the involvement of genes regulating contractile proteins and airway responsiveness. For example, variations in the *ADRB2* gene, which encodes the beta-2 adrenergic receptor, have been linked to impaired bronchodilation and increased ASM contraction. This genetic predisposition can lead to chronic airway narrowing and subsequent muscle hypertrophy as the ASM cells adapt to sustained mechanical stress. Similarly, mutations in genes encoding actin and myosin, the primary components of muscle contraction machinery, can alter ASM function and contribute to hypertrophic remodeling.
Epigenetic modifications influenced by genetic predisposition also play a role in ASM hypertrophy. Certain genetic variants can affect DNA methylation patterns or microRNA expression, which in turn regulate genes involved in muscle cell proliferation and survival. For instance, hypermethylation of genes that suppress ASM growth, such as *PTEN*, has been observed in asthmatic patients with significant muscle hypertrophy. These epigenetic changes, driven by underlying genetic susceptibility, can exacerbate ASM remodeling and contribute to the severity of asthma.
In conclusion, genetic predisposition is a critical determinant of smooth muscle hypertrophy in asthma, with specific genes and pathways influencing ASM cell behavior and airway structure. Variations in genes related to growth factors, contractile proteins, and epigenetic regulators can increase susceptibility to hypertrophy, providing insights into the molecular mechanisms underlying asthma pathogenesis. Identifying these genetic factors not only aids in risk assessment but also opens avenues for personalized medicine, where therapies can be tailored to address the unique genetic profiles of asthmatic individuals. Further research into these genetic predispositions is vital for advancing our understanding and treatment of asthma-related ASM hypertrophy.
Pulled Muscle Pain: From Back to Belly
You may want to see also
Frequently asked questions
Smooth muscle hypertrophy in asthma refers to the abnormal thickening and enlargement of the smooth muscle cells in the airways, which contributes to airway hyperresponsiveness and obstruction, key features of asthma.
Smooth muscle hypertrophy in asthma is primarily caused by chronic inflammation, exposure to allergens, irritants, and inflammatory cytokines, which stimulate muscle cell proliferation and growth, leading to increased muscle mass and airway narrowing.
Inflammatory mediators, such as interleukin-4 (IL-4), IL-5, IL-13, and tumor necrosis factor-alpha (TNF-α), promote smooth muscle hypertrophy by activating signaling pathways (e.g., MAPK, PI3K) that enhance muscle cell proliferation, protein synthesis, and contraction, exacerbating airway remodeling.
While smooth muscle hypertrophy in asthma is considered a component of airway remodeling and may be difficult to reverse completely, treatments like inhaled corticosteroids, bronchodilators, and biologics can reduce inflammation, improve symptoms, and potentially slow the progression of airway remodeling.































