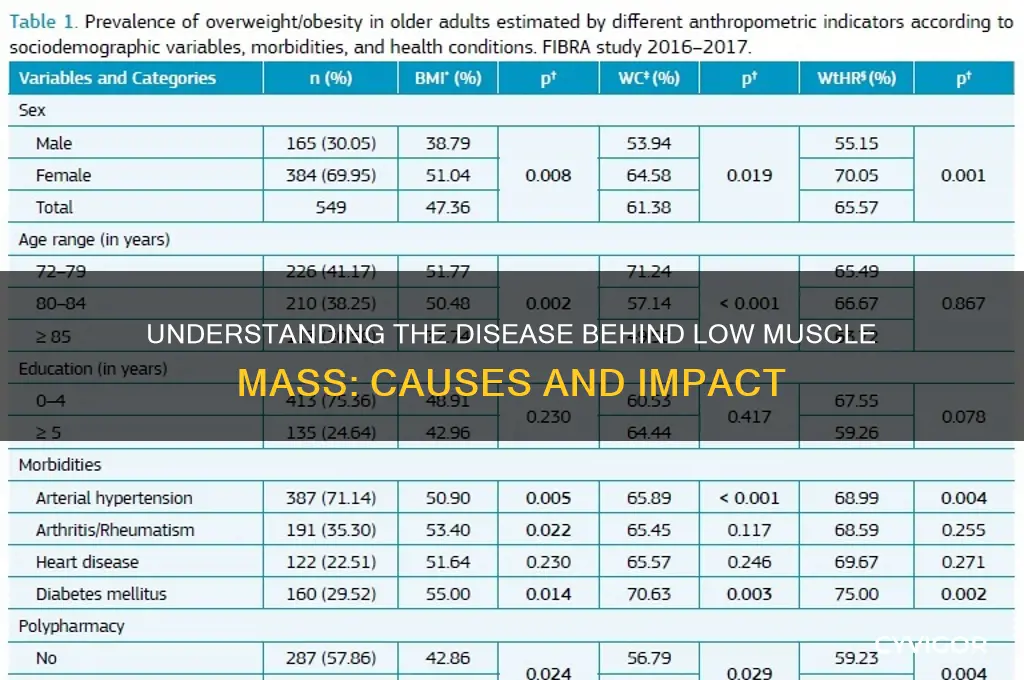
Low muscle mass, also known as sarcopenia, is primarily associated with aging but can also be caused by various underlying diseases and conditions. Chronic illnesses such as chronic kidney disease, chronic obstructive pulmonary disease (COPD), and congestive heart failure often lead to muscle wasting due to inflammation, hormonal imbalances, and reduced physical activity. Endocrine disorders like hypothyroidism, hypercortisolism (Cushing’s syndrome), and growth hormone deficiency can disrupt muscle metabolism and repair. Additionally, autoimmune diseases such as rheumatoid arthritis, systemic lupus erythematosus, and inflammatory bowel disease contribute to muscle loss through chronic inflammation and malnutrition. Cancer and its treatments, including chemotherapy and radiation, are also significant causes of muscle atrophy due to cachexia, a syndrome characterized by severe weight loss and muscle wasting. Identifying and addressing the underlying disease is crucial in managing and potentially reversing low muscle mass.
| Characteristics | Values |
|---|---|
| Disease Name | Sarcopenia, Muscular Dystrophy, Cachexia, Cushing's Syndrome, Hypothyroidism, etc. |
| Primary Cause | Age-related muscle loss, genetic mutations, chronic conditions, hormonal imbalances, malnutrition, or inactivity. |
| Symptoms | Muscle weakness, decreased muscle size, fatigue, reduced mobility, and increased risk of falls. |
| Risk Factors | Aging, sedentary lifestyle, poor nutrition, chronic diseases (e.g., cancer, COPD, heart failure), and hormonal disorders. |
| Diagnosis | Muscle strength tests, imaging (MRI, CT), dual-energy X-ray absorptiometry (DXA), and blood tests for underlying conditions. |
| Treatment | Resistance training, protein-rich diet, hormone therapy (if applicable), medication for underlying conditions, and lifestyle modifications. |
| Prevention | Regular exercise, adequate protein intake, managing chronic diseases, and maintaining a healthy weight. |
| Complications | Increased risk of falls, fractures, disability, reduced quality of life, and higher mortality rates. |
| Prevalence | Affects up to 50% of adults over 80 years; varies by disease (e.g., muscular dystrophy is rare, while sarcopenia is common in older adults). |
| Research Focus | Understanding molecular mechanisms, developing targeted therapies, and improving diagnostic tools. |
Explore related products






What You'll Learn
- Sarcopenia: Age-related muscle loss, leading to weakness and frailty in older adults
- Cancer Cachexia: Muscle wasting due to cancer, causing weight loss and fatigue
- Chronic Kidney Disease: Reduced muscle mass from kidney dysfunction and metabolic imbalances
- Cushing’s Syndrome: Excess cortisol levels result in muscle atrophy and weakness
- HIV/AIDS: Muscle loss from chronic inflammation and immune system deterioration
![]()
Sarcopenia: Age-related muscle loss, leading to weakness and frailty in older adults
Sarcopenia is a progressive and debilitating condition characterized by the gradual loss of skeletal muscle mass, strength, and function, primarily affecting older adults. This age-related muscle loss is a natural part of the aging process but can significantly impact an individual's quality of life. As people age, their bodies undergo various physiological changes, and sarcopenia is one of the key contributors to the physical decline often associated with old age. The term 'sarcopenia' originates from the Greek words 'sarx' meaning flesh and 'penia' meaning loss, aptly describing the condition. It is a major concern in geriatric health, as it leads to decreased mobility, increased risk of falls, and a loss of independence.
The onset of sarcopenia is typically gradual, making it a silent contributor to the frailty often seen in the elderly. It is estimated that after the age of 50, individuals can lose up to 1-2% of their muscle mass per year, with the rate potentially accelerating after the age of 60. This muscle loss is not merely a cosmetic issue; it has profound implications for overall health. Muscles play a crucial role in metabolism, movement, and even cognitive function. As muscle mass decreases, so does muscle strength and endurance, making daily activities more challenging. Simple tasks like climbing stairs, carrying groceries, or even rising from a chair can become arduous, impacting an individual's ability to live independently.
Several factors contribute to the development of sarcopenia. Age-related hormonal changes, such as decreased levels of growth hormone, testosterone, and insulin-like growth factor-1, play a significant role. These hormones are essential for muscle growth and repair, and their decline disrupts the body's ability to maintain muscle mass. Additionally, older adults often experience a reduction in physical activity levels, which further accelerates muscle loss. Inactivity leads to a decrease in muscle protein synthesis, causing muscles to atrophy. Poor nutrition is another critical factor, as inadequate protein intake and overall calorie deficiency can exacerbate muscle wasting.
The consequences of sarcopenia extend beyond physical weakness. It is associated with an increased risk of falls and fractures, which can have severe implications for older adults. Hip fractures, in particular, are a significant concern, often leading to hospitalization and a decline in overall health. Moreover, sarcopenia is linked to metabolic abnormalities, including insulin resistance and type 2 diabetes. The condition also contributes to a decreased basal metabolic rate, making weight management more challenging. As muscle tissue is metabolically active, its loss can lead to an increased risk of obesity and related health issues.
Managing and preventing sarcopenia involves a multi-faceted approach. Regular resistance exercise is paramount, as it stimulates muscle growth and strength. Older adults should engage in activities like weight lifting, bodyweight exercises, or resistance band workouts to counteract muscle loss. Adequate nutrition is equally vital, with a focus on sufficient protein intake to support muscle health. Healthcare professionals often recommend a diet rich in lean proteins, combined with regular exercise, to mitigate the effects of sarcopenia. Early intervention is key, as it can help slow down the progression of muscle loss and maintain functional independence in older adults.
Tramadol and Gabapentin: Understanding Neck Twitching
You may want to see also
Explore related products






![]()
Cancer Cachexia: Muscle wasting due to cancer, causing weight loss and fatigue
Cancer cachexia is a complex and debilitating syndrome characterized by significant muscle wasting, weight loss, and fatigue in cancer patients. Unlike typical weight loss resulting from reduced food intake, cachexia involves the rapid breakdown of muscle tissue, even when nutritional intake is adequate. This condition is driven by a combination of factors, including the body’s inflammatory response to cancer, metabolic changes, and the release of cytokines and other molecules by tumors. These factors disrupt normal muscle protein synthesis and increase protein degradation, leading to progressive muscle loss. Cachexia is particularly prevalent in cancers of the lung, pancreas, stomach, and esophagus but can occur in any type of cancer, especially in advanced stages.
The muscle wasting associated with cancer cachexia has profound effects on a patient’s quality of life and prognosis. As muscle mass decreases, patients experience weakness, reduced physical function, and increased fatigue, making it difficult to perform daily activities or tolerate cancer treatments. The loss of muscle also compromises the body’s ability to recover from surgery, chemotherapy, or radiation therapy, often leading to poorer treatment outcomes. Additionally, cachexia contributes to a decline in immune function, further exacerbating the patient’s vulnerability to infections and complications. Despite its significant impact, cachexia is often underrecognized and undertreated, highlighting the need for greater awareness and targeted interventions.
Weight loss is a hallmark of cancer cachexia, but it differs from weight loss caused by simple malnutrition or dieting. In cachexia, the body preferentially loses muscle mass rather than fat, even when fat stores remain intact. This selective muscle wasting is accompanied by a loss of appetite (anorexia), which further compounds the problem by reducing nutrient intake. The combination of muscle loss and anorexia creates a vicious cycle, as decreased muscle mass lowers metabolic rate, while reduced food intake fails to meet the body’s energy demands. This metabolic imbalance accelerates the progression of cachexia, making it a challenging condition to manage.
Fatigue is another debilitating symptom of cancer cachexia, often described by patients as overwhelming and unrelenting. Unlike ordinary tiredness, cachexia-related fatigue is not alleviated by rest and can severely impair a patient’s ability to function. The fatigue is multifactorial, stemming from muscle wasting, inflammation, anemia, and the psychological burden of cancer. It also contributes to social isolation and depression, as patients struggle to engage in activities they once enjoyed. Addressing fatigue in cachexia requires a multifaceted approach, including nutritional support, physical activity, and psychological interventions, though these measures often provide limited relief.
Managing cancer cachexia involves a combination of strategies aimed at preserving muscle mass, improving nutritional status, and alleviating symptoms. Nutritional interventions, such as high-protein, high-calorie diets or specialized supplements, can help slow muscle loss, but they are often insufficient on their own. Pharmacological treatments, including appetite stimulants, anti-inflammatory drugs, and anabolic agents, are being explored, though none have proven universally effective. Physical activity, particularly resistance exercise, has shown promise in maintaining muscle strength and function, but it must be tailored to the patient’s capabilities. Ultimately, addressing cachexia requires early recognition, a multidisciplinary approach, and ongoing research to develop more effective therapies for this devastating complication of cancer.
Understanding Head Muscle Tension: Causes and Triggers Explained
You may want to see also
Explore related products






![]()
Chronic Kidney Disease: Reduced muscle mass from kidney dysfunction and metabolic imbalances
Chronic Kidney Disease (CKD) is a progressive condition where the kidneys gradually lose their function over time. As the kidneys fail to effectively filter waste and maintain fluid balance, a cascade of metabolic imbalances ensues, significantly impacting muscle health. One of the most notable consequences of CKD is the reduction in muscle mass, a condition often referred to as sarcopenia. This muscle wasting is not merely a cosmetic concern but a critical health issue that affects mobility, strength, and overall quality of life. The kidneys play a vital role in regulating electrolytes, acid-base balance, and hormone production, all of which are essential for muscle maintenance and growth. When kidney function declines, these regulatory mechanisms are disrupted, leading to an environment that is detrimental to muscle tissue.
The primary mechanisms linking CKD to reduced muscle mass involve metabolic acidosis, electrolyte imbalances, and altered hormone levels. Metabolic acidosis, a common complication of CKD, occurs when the kidneys fail to excrete enough acid, leading to an accumulation of hydrogen ions in the blood. This acidic environment impairs protein synthesis and accelerates protein breakdown in muscle cells, resulting in net muscle loss. Additionally, imbalances in electrolytes such as calcium, phosphorus, and potassium can further exacerbate muscle dysfunction. For instance, elevated phosphorus levels, often seen in CKD, contribute to vascular calcification and reduce the bioavailability of calcium, both of which are crucial for muscle contraction and repair.
Hormonal imbalances also play a significant role in muscle wasting associated with CKD. The kidneys are involved in the production of erythropoietin (EPO), a hormone that stimulates red blood cell production, and the activation of vitamin D. In CKD, decreased EPO levels lead to anemia, reducing oxygen delivery to muscles and impairing their function. Similarly, impaired vitamin D activation results in insufficient calcium absorption and secondary hyperparathyroidism, which negatively affects muscle strength and bone health. Moreover, CKD is often accompanied by insulin resistance and decreased levels of insulin-like growth factor-1 (IGF-1), both of which are critical for muscle growth and repair.
Nutritional deficiencies and inflammation further compound the problem of muscle wasting in CKD patients. Dietary restrictions imposed to manage CKD, such as limiting protein intake to reduce the workload on the kidneys, can inadvertently lead to inadequate protein consumption, a key nutrient for muscle maintenance. Chronic inflammation, another hallmark of CKD, promotes the release of pro-inflammatory cytokines that accelerate muscle breakdown and inhibit muscle regeneration. This inflammatory state, combined with oxidative stress, creates a hostile environment for muscle cells, making it difficult for them to repair and grow.
Managing muscle mass loss in CKD requires a multifaceted approach. Dietary interventions, such as optimizing protein intake within safe limits and ensuring adequate calorie consumption, are essential. Supplementation with essential amino acids, particularly leucine, can stimulate muscle protein synthesis. Additionally, addressing metabolic acidosis through bicarbonate supplementation or dietary modifications can help mitigate muscle breakdown. Exercise, particularly resistance training, is crucial for preserving and building muscle mass, though it must be tailored to the individual’s functional capacity and disease stage. Pharmacological interventions, such as anabolic agents or medications to manage hormonal imbalances, may also be considered under medical supervision. Early detection and management of CKD are vital to prevent or slow the progression of muscle wasting, ultimately improving patients’ functional outcomes and quality of life.
Understanding Muscle Fatigue: Causes Behind Sustained Contraction Exhaustion
You may want to see also
Explore related products





![]()
Cushing’s Syndrome: Excess cortisol levels result in muscle atrophy and weakness
Cushing's Syndrome is a rare but significant condition that leads to low muscle mass, primarily due to excess cortisol levels in the body. Cortisol, often referred to as the stress hormone, plays a crucial role in metabolism, immune response, and stress management. However, when cortisol levels are chronically elevated, as in Cushing's Syndrome, it can have detrimental effects on muscle tissue. This condition is typically caused by prolonged exposure to high levels of cortisol, either due to the body producing too much of it or from long-term use of corticosteroid medications. The excessive cortisol breaks down proteins in muscle cells, leading to muscle atrophy and weakness, which are hallmark symptoms of this syndrome.
The mechanism behind muscle atrophy in Cushing's Syndrome involves cortisol's catabolic effects on muscle tissue. Cortisol increases protein breakdown and decreases protein synthesis, tipping the balance toward muscle loss. Additionally, it interferes with insulin function, reducing glucose uptake by muscle cells and further impairing their ability to maintain mass and strength. Patients with Cushing's Syndrome often experience progressive muscle weakness, particularly in the proximal muscles of the limbs, making everyday activities like climbing stairs or lifting objects increasingly difficult. This muscle wasting is not only a physical burden but also contributes to a reduced quality of life.
Diagnosing Cushing's Syndrome involves a series of tests to measure cortisol levels in the blood, urine, and saliva, as well as imaging studies to identify the source of excess cortisol production, such as a tumor in the pituitary or adrenal glands. Early detection is crucial, as prolonged exposure to high cortisol levels can lead to irreversible muscle damage. Treatment focuses on addressing the underlying cause, which may involve surgery to remove tumors, medication to reduce cortisol production, or, in some cases, radiation therapy. Managing cortisol levels effectively can slow or halt muscle atrophy and improve muscle strength over time.
Preventing further muscle loss in Cushing's Syndrome also requires a multidisciplinary approach, including physical therapy and nutritional interventions. Resistance training, under professional guidance, can help stimulate muscle growth and counteract atrophy. A diet rich in high-quality protein is essential to support muscle repair and synthesis. Patients are also advised to monitor their activity levels to avoid overexertion, which can exacerbate muscle weakness. Education about the condition and its management empowers individuals to take proactive steps in preserving muscle mass and function.
In summary, Cushing's Syndrome is a critical condition causing low muscle mass due to excess cortisol levels, leading to muscle atrophy and weakness. Understanding its mechanisms, early diagnosis, and comprehensive treatment are key to managing this condition effectively. By addressing the root cause, implementing targeted therapies, and adopting supportive lifestyle measures, individuals with Cushing's Syndrome can mitigate muscle loss and improve their overall well-being. Awareness and timely intervention are vital in combating the debilitating effects of this disease on muscle health.
Pinched Nerves and Muscle Pain: Understanding the Surprising Connection
You may want to see also
Explore related products





![]()
HIV/AIDS: Muscle loss from chronic inflammation and immune system deterioration
HIV/AIDS is a significant cause of low muscle mass, primarily due to chronic inflammation and progressive immune system deterioration. As the virus attacks and weakens the immune system, it triggers persistent inflammation throughout the body. This chronic inflammatory state disrupts normal muscle metabolism, leading to increased protein breakdown and reduced protein synthesis. Over time, this imbalance results in muscle wasting, a condition known as HIV-associated muscle atrophy or myopathy. The inflammation also interferes with muscle repair mechanisms, further exacerbating muscle loss.
The immune system’s decline in HIV/AIDS plays a critical role in muscle wasting. CD4+ T cells, which are crucial for immune function, are progressively destroyed by the virus. This depletion impairs the body’s ability to combat infections and maintain tissue integrity, including muscle tissue. Additionally, the release of pro-inflammatory cytokines, such as TNF-alpha and IL-6, during immune activation contributes to muscle catabolism. These cytokines signal pathways that promote muscle breakdown while inhibiting muscle growth, accelerating the loss of lean body mass.
Nutritional deficiencies often accompany HIV/AIDS, compounding the problem of muscle loss. The chronic inflammation and metabolic changes associated with the disease can lead to increased energy expenditure and malabsorption of nutrients, making it difficult for individuals to maintain adequate caloric and protein intake. This nutritional deficit further hinders muscle maintenance and repair. Moreover, opportunistic infections and side effects of antiretroviral therapy (ART) can worsen appetite loss and gastrointestinal issues, exacerbating muscle wasting.
Despite the challenges, effective management of HIV/AIDS can mitigate muscle loss. Antiretroviral therapy is pivotal in suppressing viral replication, reducing chronic inflammation, and preserving immune function, which indirectly supports muscle health. Additionally, targeted nutritional interventions, such as high-protein diets and supplementation with branched-chain amino acids (BCAAs), can help counteract muscle breakdown. Resistance exercise, when feasible, has also been shown to stimulate muscle protein synthesis and improve muscle mass in individuals with HIV/AIDS.
In summary, HIV/AIDS-induced muscle loss is a multifaceted issue stemming from chronic inflammation, immune system deterioration, and associated nutritional challenges. Addressing these factors through comprehensive care, including ART, nutritional support, and physical activity, is essential for preserving muscle mass and improving quality of life in affected individuals. Understanding the mechanisms behind this muscle wasting is crucial for developing effective strategies to combat this debilitating aspect of the disease.
Sunburn and Muscle Cramps: What's the Connection?
You may want to see also
Frequently asked questions
Several diseases can cause low muscle mass, including sarcopenia (age-related muscle loss), muscular dystrophy, and cachexia (often associated with chronic illnesses like cancer or heart failure).
Sarcopenia is a progressive loss of muscle mass, strength, and function that occurs with aging. It is primarily caused by decreased physical activity, hormonal changes, and inadequate nutrition, leading to reduced muscle mass over time.
Yes, chronic conditions such as cancer, chronic kidney disease, and COPD can lead to low muscle mass through a condition called cachexia. Cachexia involves muscle wasting due to inflammation, metabolic changes, and reduced nutrient intake associated with these illnesses.































