The process of muscle contraction is a complex interplay of neural signals and biochemical reactions, with neurotransmitters playing a crucial role in initiating this process. At the neuromuscular junction, the neurotransmitter acetylcholine is released from motor neurons, binding to receptors on muscle fibers and triggering a cascade of events that ultimately lead to muscle contraction. Acetylcholine is synthesized in the nerve terminal and stored in synaptic vesicles, ready to be released upon neural stimulation. Once released, it diffuses across the synaptic cleft and binds to nicotinic acetylcholine receptors on the muscle fiber, causing ion channels to open and initiate an action potential that propagates along the muscle fiber, leading to the release of calcium ions and the subsequent contraction of the muscle. Understanding the role of acetylcholine in muscle contraction is essential for comprehending the underlying mechanisms of movement and motor control.
| Characteristics | Values |
|---|---|
| Neurotransmitter | Acetylcholine (ACh) |
| Function | Triggers muscle contraction by activating nicotinic acetylcholine receptors (nAChRs) at the neuromuscular junction |
| Receptor Type | Nicotinic acetylcholine receptors (nAChRs), specifically the α1β1δγ or α1β1δε subunit composition in adult skeletal muscle |
| Release Site | Motor neuron terminal (presynaptic) |
| Target Cells | Skeletal muscle fibers (postsynaptic) |
| Mechanism | Binds to nAChRs, causing ion channel opening, influx of Na+ and Ca2+, depolarization, and muscle fiber contraction via excitation-contraction coupling |
| Inactivation | Rapid hydrolysis by acetylcholinesterase (AChE) in the synaptic cleft |
| Role in Disease | Myasthenia gravis (autoimmune disorder affecting ACh receptors), Botulism (toxin blocks ACh release) |
| Pharmacological Target | Neuromuscular blocking agents (e.g., succinylcholine, tubocurarine) act on ACh receptors or inhibit ACh release |
| Other Functions | Also involved in autonomic nervous system functions, cognition, and other physiological processes, but not directly related to muscle contraction |
Explore related products






What You'll Learn
![]()
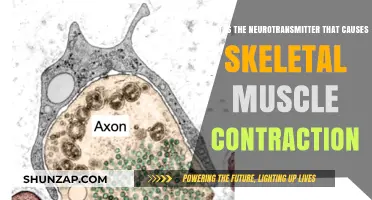
Acetylcholine's Role in Neuromuscular Junction
Acetylcholine (ACh) is the primary neurotransmitter responsible for muscle contraction at the neuromuscular junction (NMJ), the specialized synapse where motor neurons communicate with skeletal muscle fibers. When an action potential reaches the terminal end of a motor neuron, it triggers the release of ACh into the synaptic cleft. This process is crucial for initiating muscle movement, as ACh acts as the chemical messenger that bridges the gap between the nervous system and the muscular system. Without ACh, the signal from the neuron would not be transmitted to the muscle, and contraction would not occur.
At the neuromuscular junction, ACh binds to nicotinic acetylcholine receptors (nAChRs) located on the motor end plate of the muscle fiber. These receptors are ligand-gated ion channels that, upon activation, allow sodium ions (Na⁺) to flow into the muscle cell. The influx of Na⁺ depolarizes the muscle fiber, creating an end-plate potential. If this potential reaches the threshold, it triggers an action potential that propagates along the muscle fiber, leading to the release of calcium ions (Ca²⁺) from the sarcoplasmic reticulum. Calcium then initiates the sliding filament mechanism, resulting in muscle contraction.
The role of ACh in this process is transient but essential. Once ACh has activated the nAChRs, it is rapidly broken down by the enzyme acetylcholinesterase (AChE) in the synaptic cleft. This degradation ensures that ACh does not continuously stimulate the muscle, allowing for precise control over the duration and intensity of muscle contraction. The breakdown products, choline and acetate, are recycled back into the neuron to synthesize more ACh, maintaining the efficiency of the neuromuscular junction.
Dysfunction in ACh signaling at the neuromuscular junction can lead to severe muscular disorders. For example, myasthenia gravis is an autoimmune condition where antibodies attack nAChRs, impairing ACh binding and causing muscle weakness. Conversely, inhibitors of AChE, such as neostigmine, are used therapeutically to increase ACh levels and improve muscle function in certain conditions. Understanding ACh’s role at the NMJ is therefore critical for both physiological insight and clinical applications.
In summary, acetylcholine plays a central and irreplaceable role at the neuromuscular junction by transmitting the neural signal that initiates muscle contraction. Its interaction with nAChRs, subsequent degradation by AChE, and the resulting depolarization of the muscle fiber are fundamental steps in the process of voluntary movement. The precision and efficiency of ACh signaling underscore its importance in maintaining proper muscular function and highlight its significance in both health and disease.
Trigger Point Release Therapy: Does It Weaken Muscles?
You may want to see also
Explore related products






![]()
Nicotinic Receptors and Muscle Contraction
The neurotransmitter primarily responsible for muscle contraction is acetylcholine (ACh), which acts on nicotinic acetylcholine receptors (nAChRs) at the neuromuscular junction (NMJ). These receptors are ligand-gated ion channels that play a critical role in transmitting signals from motor neurons to skeletal muscle fibers, initiating muscle contraction. Nicotinic receptors are named for their sensitivity to nicotine, which mimics the action of acetylcholine, but their primary physiological function is mediated by ACh. At the NMJ, the release of ACh from the presynaptic terminal binds to nAChRs on the postsynaptic muscle fiber, triggering a cascade of events that lead to muscle contraction.
Nicotinic receptors at the NMJ are pentameric complexes composed of five subunits arranged around a central pore. In skeletal muscle, the most common subunit composition is two α1 subunits, one β subunit, one δ subunit, and one ε subunit (α1)2βδε). When ACh binds to the α1 subunits, it causes a conformational change in the receptor, opening the ion channel and allowing the influx of sodium ions (Na⁺) and the efflux of potassium ions (K⁺). This rapid ion flux depolarizes the muscle fiber membrane, generating an end-plate potential (EPP). If the EPP reaches the threshold, it triggers the opening of voltage-gated sodium channels, propagating an action potential along the muscle fiber.
The action potential then travels to the sarcoplasmic reticulum (SR), where it releases calcium ions (Ca²⁺) into the cytoplasm via ryanodine receptors. Calcium binds to troponin, causing a conformational change in the troponin-tropomyosin complex, which exposes the myosin-binding sites on actin filaments. This interaction between myosin and actin, powered by ATP hydrolysis, results in muscle contraction through the sliding filament mechanism. Thus, the activation of nicotinic receptors by ACh is the critical first step in this sequence of events.
Nicotinic receptors are highly selective for ACh, ensuring precise control over muscle contraction. Their rapid activation and desensitization properties allow for quick and coordinated muscle responses. After ACh binds and triggers the opening of the ion channel, the receptor quickly desensitizes, even in the continued presence of ACh. This desensitization is important for preventing prolonged muscle contraction and ensuring that the muscle can relax once ACh is hydrolyzed by acetylcholinesterase (AChE) in the synaptic cleft. The transient nature of nAChR activation is essential for the fine control of muscle movement.
In summary, nicotinic receptors are indispensable for muscle contraction, serving as the primary interface between motor neurons and skeletal muscle fibers. Their activation by acetylcholine initiates a series of events that ultimately lead to the sliding of actin and myosin filaments and muscle contraction. Understanding the role of nAChRs in this process highlights their significance in neuromuscular physiology and provides insights into disorders such as myasthenia gravis, where nAChR dysfunction impairs muscle function. The precise mechanisms of nAChR activation and desensitization underscore the elegance and efficiency of the neuromuscular system.
Unraveling the Root Causes of Muscle Diseases: A Comprehensive Overview
You may want to see also
Explore related products






![]()
Synaptic Vesicle Release Mechanism
The neurotransmitter primarily responsible for causing muscle contraction is acetylcholine (ACh). At the neuromuscular junction, motor neurons release acetylcholine into the synaptic cleft, where it binds to nicotinic acetylcholine receptors on the muscle fiber, initiating a cascade of events leading to muscle contraction. This process is fundamentally dependent on the precise and rapid release of acetylcholine from synaptic vesicles within the presynaptic terminal. The synaptic vesicle release mechanism is a highly regulated process that ensures the timely and efficient delivery of neurotransmitters to the synaptic cleft, enabling muscle contraction and other neural functions.
The synaptic vesicle release mechanism begins with the docking of synaptic vesicles to the presynaptic membrane. This docking is facilitated by SNARE proteins (Soluble N-ethylmaleimide-sensitive factor Attachment protein REceptors), which include synaptobrevin (on the vesicle), syntaxin, and SNAP-25 (on the plasma membrane). These proteins form a complex that brings the vesicle membrane into close apposition with the presynaptic membrane, priming the vesicle for fusion. Calcium ions (Ca²⁺) play a critical role in this process, as they are required to trigger the final steps of vesicle fusion. When an action potential reaches the presynaptic terminal, voltage-gated calcium channels open, allowing Ca²⁺ to influx into the terminal.
Calcium ions bind to synaptotagmin, a calcium sensor protein located on the synaptic vesicle. This binding induces a conformational change in the SNARE complex, leading to the fusion of the vesicle membrane with the presynaptic membrane. The fusion pore that forms allows the contents of the vesicle, including acetylcholine, to be released into the synaptic cleft. This release is rapid and occurs within milliseconds of calcium influx, ensuring the immediate availability of neurotransmitter for binding to postsynaptic receptors. The precision of this mechanism is essential for the coordination of muscle contraction, as it ensures that acetylcholine is released in the correct quantity and at the appropriate time.
Following release, the fusion pore may either dilate fully, allowing complete vesicle collapse and incorporation of its membrane into the presynaptic membrane, or it may close, allowing the vesicle to be retrieved through endocytosis for recycling. The retrieval process involves the reformation of synaptic vesicles from the endosomal membrane, a step regulated by proteins such as clathrin and dynamin. This recycling mechanism is crucial for sustaining repeated rounds of neurotransmitter release, particularly during sustained muscle activity. Without efficient vesicle recycling, the presynaptic terminal would quickly deplete its supply of synaptic vesicles, impairing the ability to maintain muscle contraction.
In summary, the synaptic vesicle release mechanism is a tightly orchestrated process involving vesicle docking, priming, calcium-triggered fusion, and recycling. For muscle contraction, this mechanism ensures the rapid and reliable release of acetylcholine at the neuromuscular junction. The interplay of SNARE proteins, calcium ions, and synaptotagmin is central to this process, highlighting the molecular precision required for effective neurotransmission. Understanding this mechanism not only sheds light on the fundamental biology of muscle control but also provides insights into disorders related to synaptic dysfunction, such as myasthenia gravis, where acetylcholine release or signaling is impaired.
Muscle Imbalances: Causes and Factors to Consider
You may want to see also
Explore related products

$16.95 $17.88




![]()
Acetylcholinesterase Enzyme Function
The neurotransmitter primarily responsible for causing muscle contraction is acetylcholine (ACh). Acetylcholine is released at the neuromuscular junction, where it binds to receptors on muscle fibers, initiating a cascade of events that lead to muscle contraction. However, to ensure precise control over muscle activity, acetylcholine must be rapidly broken down after it has performed its function. This is where the acetylcholinesterase (AChE) enzyme plays a critical role. Acetylcholinesterase is a key enzyme in the nervous system that terminates the action of acetylcholine by hydrolyzing it into acetic acid and choline, effectively stopping muscle contraction and preparing the system for the next signal.
The primary function of acetylcholinesterase is to rapidly degrade acetylcholine in the synaptic cleft, the small gap between neurons and muscle cells. This degradation is essential for preventing continuous stimulation of the muscle, which could lead to prolonged or uncontrolled contractions. AChE acts almost immediately after acetylcholine has bound to its receptors, ensuring that the signal is transient and that the muscle can relax. This rapid breakdown allows for precise control over muscle movements, whether they are voluntary (e.g., lifting an arm) or involuntary (e.g., heartbeat).
Acetylcholinesterase is highly efficient, capable of breaking down thousands of acetylcholine molecules per second. Its active site is specifically designed to bind acetylcholine, facilitating the hydrolysis reaction. This efficiency is crucial in the neuromuscular junction, where timing and precision are vital for coordinated muscle function. Without AChE, acetylcholine would remain in the synaptic cleft, leading to overstimulation of muscle fibers and potential paralysis or spasms.
Inhibitors of acetylcholinesterase, such as neostigmine or organophosphates, are used medically to treat conditions like myasthenia gravis, where muscle weakness occurs due to impaired acetylcholine signaling. However, excessive inhibition of AChE can lead to acetylcholine accumulation, causing symptoms like muscle cramps, respiratory distress, and even death. This highlights the critical balance that AChE maintains in the nervous system.
In summary, the acetylcholinesterase enzyme is indispensable for regulating muscle contraction by ensuring the prompt termination of acetylcholine’s action. Its function is vital for maintaining the delicate balance between muscle activation and relaxation, enabling smooth and controlled movements. Understanding AChE’s role not only sheds light on normal muscle physiology but also provides insights into disorders related to acetylcholine dysregulation and the mechanisms of certain toxins and drugs.
Muscle Weakness and Shortness of Breath: What's the Link?
You may want to see also
Explore related products






![]()
Excitation-Contraction Coupling Process
The process of muscle contraction begins with a signal from the nervous system, where the neurotransmitter acetylcholine plays a crucial role. Acetylcholine is released at the neuromuscular junction, the interface between a motor neuron and a muscle fiber. When an action potential reaches the terminal of the motor neuron, it triggers the release of acetylcholine into the synaptic cleft. This neurotransmitter binds to nicotinic acetylcholine receptors on the muscle fiber's motor end plate, initiating the excitation-contraction coupling process. This process is essential for converting the electrical signal from the neuron into a mechanical muscle contraction.
The binding of acetylcholine to its receptors causes these ion channels to open, allowing sodium ions (Na⁺) to flow into the muscle fiber. This influx of sodium ions depolarizes the muscle cell membrane, creating an action potential that propagates along the sarcolemma (the muscle cell membrane) and into the transverse tubules (T-tubules). The T-tubules are invaginations of the sarcolemma that extend deep into the muscle fiber, ensuring the action potential reaches the interior of the cell. This depolarization is the first step in the excitation-contraction coupling process, setting the stage for calcium release and muscle contraction.
As the action potential travels through the T-tubules, it triggers the opening of voltage-gated L-type calcium channels (dihydropyridine receptors) located on the T-tubule membrane. These channels are physically coupled to ryanodine receptors (RyR) on the sarcoplasmic reticulum (SR), the muscle cell's calcium store. When the L-type calcium channels open, a small amount of calcium ions (Ca²⁺) enters the cytoplasm. This calcium binds to the RyR, causing it to open and release a large amount of calcium from the SR into the cytoplasm. This rapid increase in cytoplasmic calcium concentration is critical for muscle contraction.
The released calcium ions bind to troponin, a protein complex located on the thin (actin) filaments of the muscle fiber. Troponin, in turn, moves tropomyosin, another protein that blocks the active sites on actin. With tropomyosin shifted, the active sites on actin are exposed, allowing myosin heads (on the thick filaments) to bind to actin. This binding and subsequent power stroke of the myosin heads pull the actin filaments toward the center of the sarcomere, causing the muscle to contract. This mechanism is known as the sliding filament theory and is directly dependent on the calcium release initiated by the excitation-contraction coupling process.
Finally, to relax the muscle, calcium ions are actively pumped back into the sarcoplasmic reticulum by SERCA pumps (sarcoplasmic/endoplasmic reticulum Ca²⁺ ATPase). As calcium levels in the cytoplasm decrease, troponin and tropomyosin return to their resting positions, blocking the actin-myosin binding sites and halting contraction. Simultaneously, acetylcholine in the synaptic cleft is broken down by acetylcholinesterase, terminating its signal and allowing the muscle to return to its resting state. This precise regulation ensures that muscle contraction is both rapid and reversible, enabling coordinated movement. The excitation-contraction coupling process thus bridges the gap between neural signaling and muscular action, highlighting the intricate interplay between electrical, chemical, and mechanical events in muscle physiology.
Understanding Mixed Connective Tissue Disease's Impact on Muscles
You may want to see also
Frequently asked questions
The neurotransmitter responsible for muscle contraction is acetylcholine (ACh).
Acetylcholine binds to nicotinic receptors on the motor end plate of muscle fibers, initiating an action potential that leads to the release of calcium ions, ultimately causing muscle contraction.
No, acetylcholine is the primary neurotransmitter at the neuromuscular junction for skeletal muscle contraction, but other neurotransmitters like norepinephrine and dopamine play roles in smooth muscle contraction.
Blocking acetylcholine release or its action (e.g., by toxins like botulinum toxin) prevents muscle contraction, leading to paralysis or muscle weakness.
Yes, disorders like myasthenia gravis involve impaired acetylcholine signaling, resulting in muscle fatigue and weakness due to reduced muscle contraction.