Strabismus, a condition characterized by misaligned eyes, is often caused by an imbalance in the extraocular muscles responsible for eye movement. These muscles, which include the medial rectus, lateral rectus, superior rectus, inferior rectus, superior oblique, and inferior oblique, work in coordination to ensure both eyes focus on the same point. When one or more of these muscles become weaker, stronger, or otherwise imbalanced—due to factors like congenital issues, nerve dysfunction, or trauma—it can lead to strabismus. For example, overaction of the medial rectus muscle can cause an esotropia (inward turning of the eye), while weakness in the lateral rectus muscle may result in exotropia (outward turning). Understanding which specific muscle is involved is crucial for determining the appropriate treatment, which may include corrective lenses, prism glasses, vision therapy, or surgical intervention to realign the eyes.
| Characteristics | Values |
|---|---|
| Muscles Involved | Extraocular muscles (EOMs), specifically the rectus and oblique muscles |
| Primary Muscles Causing Strabismus | Superior rectus, inferior rectus, medial rectus, lateral rectus, superior oblique, inferior oblique |
| Type of Strabismus | Depends on the affected muscle(s): esotropia (inward turn), exotropia (outward turn), hypertropia (upward turn), hypotropia (downward turn) |
| Muscle Imbalance | Overaction or underaction of one or more EOMs leads to misalignment |
| Common Causes | Congenital (e.g., infantile esotropia), acquired (e.g., trauma, thyroid eye disease, myasthenia gravis) |
| Neurological Control | Oculomotor nerve (CN III), trochlear nerve (CN IV), abducens nerve (CN VI) |
| Treatment Options | Prism glasses, patching, botulinum toxin injections, strabismus surgery (e.g., recession, resection, tenotomy) |
| Associated Conditions | Amblyopia (lazy eye), double vision (diplopia), reduced binocular vision |
| Prevalence | Approximately 2-4% of the population, with higher rates in children |
| Diagnosis | Cover test, prism and alternate cover test, Hirschberg test, imaging (e.g., MRI, CT) |
| Prognosis | Varies; early intervention improves outcomes, especially in children |
Explore related products






What You'll Learn
![]()
Superior rectus muscle overaction
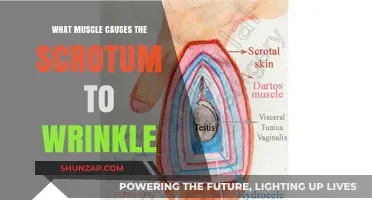
The superior rectus muscle plays a crucial role in eye movement, primarily responsible for elevating the eye and contributing to inward rotation (adduction) and outward rotation (intorsion). However, when this muscle exhibits overaction, it can lead to a specific type of strabismus, a condition characterized by misaligned eyes. Superior rectus muscle overaction occurs when the muscle contracts excessively, pulling the eye upward more than necessary, resulting in a vertical misalignment. This condition is often observed in patients with congenital or acquired strabismus, where the balance between the extraocular muscles is disrupted.
In a normally functioning eye, the superior rectus works in coordination with other extraocular muscles to ensure smooth and precise eye movements. For instance, when looking upward, the superior rectus contracts while the inferior rectus of the same eye relaxes, allowing for controlled elevation. However, in cases of overaction, this delicate balance is compromised. The excessive force exerted by the superior rectus can cause the eye to deviate upward, leading to a condition known as hypertropia, where one eye appears higher than the other. This misalignment can be constant or intermittent, depending on the severity of the muscle overaction.
Several factors can contribute to superior rectus muscle overaction. Congenital conditions, such as infantile esotropia, often involve an overactive superior rectus, leading to inward turning of the eye (esotropia) along with vertical deviation. Acquired causes may include thyroid eye disease, where inflammation and swelling of the extraocular muscles can result in overaction. Additionally, mechanical restrictions or scarring of the inferior rectus muscle, which normally counteracts the superior rectus, can lead to a relative overaction of the superior rectus, causing vertical strabismus.
Diagnosing superior rectus muscle overaction involves a comprehensive eye examination, including assessment of eye alignment, measurement of deviation in different gaze positions, and evaluation of muscle function. The Hirschberg test, cover test, and prism cover test are commonly used to quantify the degree of vertical deviation. In some cases, imaging studies like MRI or CT scans may be employed to identify underlying structural abnormalities or masses affecting muscle function. Understanding the specific pattern of overaction is crucial for determining the appropriate treatment approach.
Treatment for superior rectus muscle overaction aims to restore proper eye alignment and improve binocular vision. Non-surgical interventions, such as prism glasses, may be used to compensate for the vertical deviation and alleviate symptoms like double vision. However, surgical correction is often necessary to address the underlying muscle imbalance. The surgical procedure typically involves weakening the overacting superior rectus muscle through recession or, in some cases, strengthening the antagonist muscle (inferior rectus) through resection. The choice of technique depends on the individual case, considering factors like the degree of overaction, presence of other muscle abnormalities, and patient age. Postoperative care and follow-up are essential to monitor alignment and ensure optimal outcomes.
Thyroid Nodules: Understanding the Link to Muscle Pain
You may want to see also
Explore related products






![]()
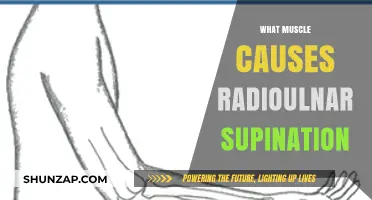
Inferior rectus muscle underaction
The inferior rectus muscle plays a crucial role in eye movement, specifically in depressing (looking downward) and adducting (turning inward) the eye. When this muscle underacts or functions inadequately, it can contribute to strabismus, a condition characterized by misaligned eyes. Inferior rectus underaction typically results in a specific type of strabismus known as hypertropia or vertical strabismus, where one eye deviates upward relative to the other. This misalignment occurs because the underacting inferior rectus muscle fails to adequately pull the eye downward, allowing the opposing muscle, the superior rectus, to overpower it and cause the eye to drift upward.
Inferior rectus underaction can arise from various causes, including congenital factors, trauma, neurological disorders, or systemic conditions affecting muscle function. For instance, Brown syndrome, a mechanical restriction of the superior oblique tendon, can lead to compensatory inferior rectus underaction. Additionally, thyroid eye disease (Graves' ophthalmopathy) can cause inflammation and fibrosis of the extraocular muscles, including the inferior rectus, leading to underaction. Neurological conditions such as myasthenia gravis or third nerve palsy can also impair inferior rectus function, resulting in vertical strabismus.
Diagnosing inferior rectus underaction involves a comprehensive eye examination, including assessment of ocular alignment, range of motion, and muscle function. The Hess screen or Lancaster red-green test may be used to evaluate vertical deviations and identify muscle underaction. Prism cover testing helps quantify the degree of hypertropia, while imaging studies like MRI or CT scans may be employed to investigate underlying structural abnormalities. Identifying the cause of the underaction is critical for determining the appropriate treatment approach.
Treatment for inferior rectus underaction depends on the underlying etiology and severity of the strabismus. In cases of mechanical restriction or fibrosis, surgical intervention may be necessary to strengthen the inferior rectus or weaken the opposing superior rectus muscle. Procedures such as rectus muscle recession or resection can help realign the eyes and restore binocular vision. For neurological or systemic causes, addressing the primary condition—such as managing thyroid eye disease or treating myasthenia gravis—may improve muscle function. Non-surgical options, including prism glasses or botulinum toxin injections, can also be considered for milder cases or as a temporary measure.
Early intervention is key to managing inferior rectus underaction and preventing complications such as double vision, amblyopia, or reduced quality of life. Patients with vertical strabismus should be monitored regularly to assess for progression and adjust treatment as needed. Collaboration between ophthalmologists, strabismus specialists, and other healthcare providers ensures a multidisciplinary approach to care, optimizing outcomes for individuals with this specific form of strabismus. Understanding the role of the inferior rectus muscle and its underaction is essential for effective diagnosis and treatment of this complex condition.
Understanding Causes of Muscle Pain at the Base of Your Head
You may want to see also
Explore related products






![]()
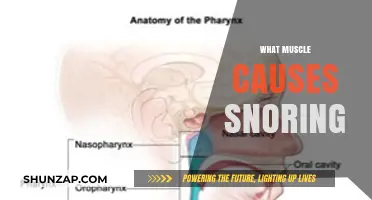
Lateral rectus muscle imbalance
Strabismus, a condition where the eyes are misaligned, can be caused by imbalances in the extraocular muscles responsible for eye movement. Among these muscles, the lateral rectus muscle plays a significant role, particularly in cases of lateral rectus muscle imbalance. This muscle, one of the six extraocular muscles, is primarily responsible for abducting the eye, meaning it moves the eye outward, away from the nose. When there is an imbalance in the function or strength of the lateral rectus muscle, it can lead to specific types of strabismus, such as abducting strabismus or exotropia, where one or both eyes deviate outward.
Diagnosing lateral rectus muscle imbalance involves a comprehensive eye examination, including assessments of eye alignment, muscle function, and visual acuity. Tools such as the Hirschberg test, cover-uncover test, and prism cover test are commonly used to evaluate the degree and direction of eye misalignment. Additionally, imaging studies or neurological evaluations may be necessary to identify underlying causes, such as nerve palsy or myopathy, that could contribute to the imbalance. Early detection is key, as untreated strabismus can lead to complications like amblyopia (lazy eye) or double vision.
Treatment for lateral rectus muscle imbalance depends on the severity and underlying cause of the condition. Non-surgical interventions may include prism glasses to correct visual misalignment or vision therapy to strengthen eye muscles and improve coordination. In cases where the imbalance is significant or progressive, surgical intervention may be required. Strabismus surgery involves adjusting the tension or position of the lateral rectus muscle to restore proper eye alignment. For example, a lateral rectus recession weakens the muscle by moving its attachment point farther back on the eye, while a lateral rectus resection shortens the muscle to strengthen its effect.
Post-treatment care is essential to ensure long-term success and stability of the eye alignment. Patients may require follow-up appointments to monitor progress and make adjustments as needed. In some cases, additional interventions, such as patching or further vision therapy, may be recommended to optimize visual outcomes. Educating patients and caregivers about the importance of adherence to treatment plans and regular eye check-ups is critical for managing lateral rectus muscle imbalance effectively. By addressing the imbalance directly, individuals with strabismus can achieve improved visual function, aesthetic alignment, and overall quality of life.
Smoking Cigarettes and Muscle Spasms: Uncovering the Hidden Connection
You may want to see also
Explore related products






![]()
Medial rectus muscle weakness
Weakness in the medial rectus muscle can arise from various causes, including congenital factors, neurological disorders, or trauma. Congenital medial rectus weakness is often present at birth and may be associated with other developmental abnormalities. Acquired weakness can result from conditions such as myasthenia gravis, a neuromuscular disorder that affects muscle strength, or from damage to the oculomotor nerve (cranial nerve III), which innervates the medial rectus muscle. In cases of trauma, direct injury to the muscle or its nerve supply can lead to weakness and subsequent strabismus. Identifying the underlying cause is essential for determining the appropriate treatment approach.
Clinically, medial rectus muscle weakness is diagnosed through a comprehensive eye examination, including assessments of eye alignment, visual acuity, and ocular motility. The Hirschberg test, which evaluates corneal light reflex, and the cover-uncover test are commonly used to detect esotropia caused by medial rectus weakness. Additionally, prism and alternate cover testing can quantify the degree of misalignment. In some cases, imaging studies or electromyography may be necessary to evaluate the muscle or nerve function further. Early diagnosis is critical to prevent complications such as amblyopia (lazy eye) and to improve the chances of successful treatment.
Treatment for medial rectus muscle weakness depends on the severity and underlying cause of the condition. Non-surgical interventions may include vision therapy to strengthen eye muscles, the use of prism glasses to alleviate double vision, or patching to address amblyopia. In cases of significant misalignment, surgical correction is often recommended. Strabismus surgery involves adjusting the position or tension of the medial rectus muscle to improve eye alignment. This can be achieved by weakening the muscle (recession) or strengthening it (resection), depending on the specific needs of the patient. Postoperative care and follow-up are essential to ensure optimal outcomes and to monitor for recurrence.
Preventive measures and early intervention play a vital role in managing medial rectus muscle weakness. Regular eye examinations, particularly in children, can help detect strabismus early and prevent long-term visual impairments. Parents and caregivers should be aware of signs such as crossed eyes, frequent blinking, or head tilting, which may indicate a problem. For individuals with known risk factors, such as a family history of strabismus or neurological conditions, proactive monitoring and consultation with an ophthalmologist or strabismus specialist are highly recommended. By addressing medial rectus weakness promptly, the impact on vision and quality of life can be significantly minimized.
Zoloft's Link to Muscle Tension: What You Need to Know
You may want to see also
Explore related products






![]()
Superior oblique muscle dysfunction
The superior oblique muscle plays a crucial role in eye movement, and its dysfunction can lead to strabismus, a condition characterized by misaligned eyes. Located in the upper part of the eye, the superior oblique muscle is responsible for intorsion (rotating the eye inward), depression (moving the eye downward), and abduction (moving the eye outward). When this muscle malfunctions, it disrupts the coordinated movement of the eyes, resulting in misalignment. Superior oblique muscle dysfunction is often associated with superior oblique palsy, a condition where the muscle weakens or becomes paralyzed, leading to vertical or torsional strabismus.
One of the primary causes of superior oblique muscle dysfunction is trauma, such as head injuries or orbital fractures, which can damage the muscle or its innervating nerve, the trochlear nerve (cranial nerve IV). Additionally, neurological conditions like stroke, multiple sclerosis, or tumors affecting the brainstem can impair trochlear nerve function, leading to muscle dysfunction. Congenital abnormalities or developmental issues may also result in a weakened or underdeveloped superior oblique muscle, contributing to strabismus from an early age. Identifying the underlying cause is essential for determining the appropriate treatment approach.
Clinically, superior oblique muscle dysfunction presents with specific symptoms. Patients often experience vertical diplopia (double vision), which worsens when looking in the direction controlled by the affected muscle. For example, a left superior oblique palsy causes worse diplopia when looking down and out with the right eye. Another hallmark is head tilt, as individuals may compensate for the misalignment by tilting their head to the opposite side. In some cases, torsional strabismus occurs, where one eye appears rotated relative to the other. A comprehensive eye examination, including a Hess screen or Lancaster red-green test, can confirm the diagnosis by assessing muscle function and eye alignment.
Treatment for superior oblique muscle dysfunction depends on the severity and underlying cause. Prism glasses are often prescribed to alleviate diplopia by aligning the visual images. In mild cases, vision therapy may help improve eye coordination and reduce symptoms. For more significant misalignment, surgical intervention may be necessary. Procedures such as superior oblique tendon tuck or superior oblique weakening aim to correct the muscle imbalance and restore proper eye alignment. In cases of trochlear nerve palsy, strabismus surgery on other muscles, such as the inferior oblique, may be performed to compensate for the dysfunction.
Prevention and early intervention are key in managing superior oblique muscle dysfunction. Protecting against head injuries through the use of helmets and seatbelts can reduce the risk of trauma-induced strabismus. Regular eye examinations, especially in individuals with neurological conditions, can help detect muscle dysfunction early. For children, timely evaluation and treatment of congenital strabismus can prevent long-term visual impairments, such as amblyopia (lazy eye). Understanding the role of the superior oblique muscle in strabismus highlights the importance of targeted diagnosis and treatment to restore binocular vision and improve quality of life.
Overweight, Piriformis Syndrome, and Sciatica: What's the Link?
You may want to see also
Frequently asked questions
Strabismus is not caused by a single muscle but rather by an imbalance in the extraocular muscles that control eye movement.
While no single muscle is the sole cause, certain extraocular muscles, such as the medial rectus, lateral rectus, superior rectus, inferior rectus, superior oblique, or inferior oblique, can contribute to misalignment when weakened or overactive.
Strabismus occurs when the extraocular muscles fail to work together properly, leading to one eye deviating inward (esotropia), outward (exotropia), upward (hypertropia), or downward (hypotropia).
Yes, paralysis or weakness of one or more extraocular muscles, often due to nerve damage (e.g., third, fourth, or sixth cranial nerve palsy), can result in strabismus.
Yes, strabismus surgery involves adjusting the tension or position of the extraocular muscles to improve eye alignment and coordination.