The contraction of the lungs during breathing is primarily driven by the diaphragm, a dome-shaped muscle located at the base of the chest cavity. As the diaphragm contracts, it flattens and moves downward, creating a vacuum that pulls air into the lungs. Additionally, the intercostal muscles between the ribs play a crucial role in expanding the chest cavity, further facilitating inhalation. During forced exhalation, the internal intercostal muscles and abdominal muscles contract to push air out of the lungs. Together, these muscles work in harmony to ensure efficient ventilation and gas exchange, making them essential for respiratory function.
Explore related products





What You'll Learn
- Diaphragm Function: Primary muscle for inhalation, contracts to expand chest cavity
- Intercostal Muscles: Assist breathing, elevate ribs during deep inhalation
- Accessory Muscles: Neck/shoulder muscles aid forceful breathing (e.g., scalene, sternocleidomastoid)
- Exhalation Process: Passive, but abdominal muscles assist in forced exhalation
- Bronchioles & Alveoli: Smooth muscles regulate airflow, not primary contraction drivers
![]()
Diaphragm Function: Primary muscle for inhalation, contracts to expand chest cavity
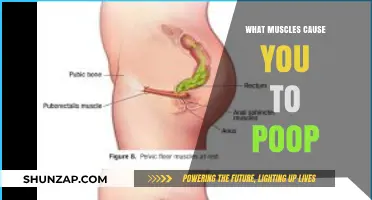
The diaphragm is the primary muscle responsible for inhalation, playing a crucial role in the respiratory process. Located at the base of the chest cavity, it is a dome-shaped muscle that separates the thoracic cavity (containing the lungs and heart) from the abdominal cavity. When the diaphragm contracts, it flattens and moves downward, creating additional space within the chest cavity. This expansion reduces the pressure inside the lungs, allowing air to flow in from the external environment, thus facilitating inhalation. This mechanism is fundamental to the act of breathing and is essential for maintaining adequate oxygen supply to the body.
The contraction of the diaphragm is initiated by signals from the brainstem, specifically the respiratory center, which sends impulses via the phrenic nerve. The phrenic nerve innervates the diaphragm, causing it to contract in a coordinated manner. This process is involuntary and occurs continuously, ensuring a steady supply of oxygen to meet the body's metabolic demands. During restful breathing, the diaphragm is the dominant muscle, accounting for approximately 75% of the air volume inhaled. Its efficiency in expanding the chest cavity makes it the most important muscle for inhalation, particularly during quiet, normal breathing.
In addition to its primary role in inhalation, the diaphragm also assists in other physiological functions. For instance, it helps in expelling air during forced exhalation, such as when coughing or sneezing, by pushing upward against the lungs. Furthermore, the diaphragm plays a role in maintaining core stability and posture, as it works in conjunction with abdominal muscles to support the spine. Its dual function in both respiration and core stability highlights the diaphragm's importance in overall bodily function.
Understanding the diaphragm's function is critical in diagnosing and treating respiratory conditions. Weakness or paralysis of the diaphragm, often due to injury, disease, or nerve damage, can lead to breathing difficulties. Conditions such as diaphragmatic paralysis or eventration (elevation of the diaphragm) can impair its ability to contract effectively, reducing lung capacity and compromising oxygen intake. In such cases, medical interventions, including physical therapy or surgical repair, may be necessary to restore proper diaphragm function and improve respiratory health.
In summary, the diaphragm is the primary muscle for inhalation, contracting to expand the chest cavity and facilitate air intake. Its role is indispensable for normal breathing and is supported by neural signals from the phrenic nerve. Beyond respiration, the diaphragm contributes to core stability and posture, underscoring its multifaceted importance. Recognizing its function is vital for understanding respiratory mechanics and addressing related disorders, ensuring optimal lung function and overall well-being.
Waking Up with Severe Stomach Muscle Pain: Causes and Remedies
You may want to see also
Explore related products






![]()
Intercostal Muscles: Assist breathing, elevate ribs during deep inhalation
The intercostal muscles play a crucial role in the mechanics of breathing, particularly during deep inhalation. These muscles are located between the ribs and are divided into three layers: the external intercostal muscles, the internal intercostal muscles, and the innermost intercostal muscles. When it comes to assisting breathing and elevating the ribs during deep inhalation, the external intercostal muscles are the primary contributors. As these muscles contract, they pull the ribs upward and outward, expanding the thoracic cavity and creating a larger space for the lungs to fill with air. This action is essential for increasing lung volume and facilitating efficient oxygen intake.
During deep inhalation, the contraction of the external intercostal muscles is coordinated with the diaphragm, the primary muscle of respiration. While the diaphragm descends to increase vertical space in the chest cavity, the external intercostal muscles work to expand the rib cage laterally. This dual action ensures maximal lung expansion, allowing for a greater volume of air to enter the lungs. The intercostal muscles are particularly active during forced or deep breathing, such as during exercise or when taking a deliberate deep breath, as they provide the necessary force to overcome the elastic recoil of the lungs and chest wall.
The anatomy of the intercostal muscles is uniquely suited to their function in breathing. The fibers of the external intercostal muscles run obliquely downward and forward from one rib to the next, which allows them to effectively elevate the ribs when they contract. This elevation not only increases the anteroposterior and lateral dimensions of the thoracic cavity but also helps maintain the structural integrity of the rib cage during the breathing cycle. Without the intercostal muscles, the rib cage would be less stable, and the efficiency of breathing, especially during deep inhalation, would be significantly compromised.
Training and maintaining the strength of the intercostal muscles can enhance respiratory function, particularly in individuals with respiratory conditions or athletes requiring optimal lung capacity. Exercises such as deep breathing techniques, playing wind instruments, or practicing activities that require controlled breathing (like yoga or swimming) can help strengthen these muscles. Additionally, awareness of proper breathing mechanics, such as engaging the intercostal muscles during inhalation, can improve overall respiratory efficiency and reduce the risk of fatigue or strain on the diaphragm.
In summary, the intercostal muscles, particularly the external intercostal muscles, are vital for assisting breathing and elevating the ribs during deep inhalation. Their coordinated contraction with the diaphragm ensures maximal lung expansion, enabling efficient air intake. Understanding their function and importance can lead to better respiratory health and performance, especially in scenarios requiring increased lung capacity. By focusing on exercises that engage these muscles, individuals can enhance their breathing mechanics and overall lung function.
Understanding Severe Torso Muscle Cramps: Causes and Triggers Explained
You may want to see also
Explore related products





![]()
Accessory Muscles: Neck/shoulder muscles aid forceful breathing (e.g., scalene, sternocleidomastoid)
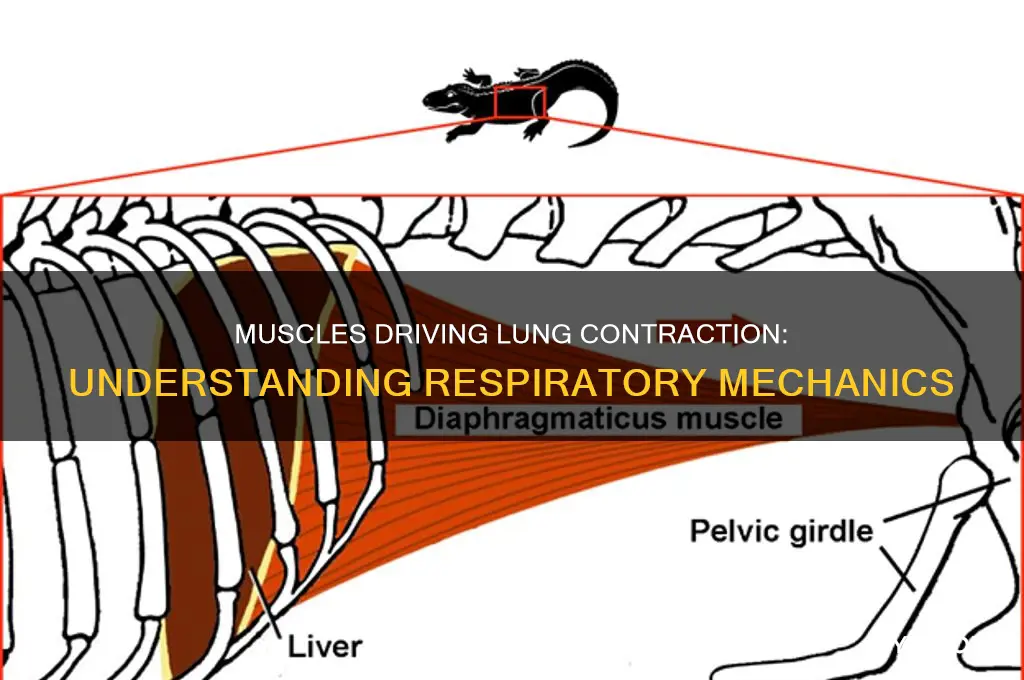
The accessory muscles of respiration, particularly those in the neck and shoulder region, play a crucial role in aiding forceful breathing. These muscles are not primarily responsible for normal, quiet breathing, which is primarily driven by the diaphragm and intercostal muscles. However, during activities that require increased ventilation, such as heavy exercise, coughing, or breathing against resistance, the accessory muscles are recruited to assist in expanding the thoracic cavity and facilitating greater air movement. Among these, the scalene muscles and the sternocleidomastoid (SCM) are the most prominent.
The scalene muscles, located in the lateral aspect of the neck, are divided into three groups: the scalenus anterior, scalenus medius, and scalenus posterior. During inhalation, these muscles contract to elevate the upper ribs, which helps expand the chest cavity and increase lung volume. The scalenus anterior and medius are particularly active during deep or forced inspiration. Their contraction lifts the first and second ribs, creating additional space for the lungs to expand. This action is especially important when the primary muscles of respiration are insufficient to meet the body’s oxygen demands, such as during intense physical activity or respiratory distress.
The sternocleidomastoid (SCM) muscle, another key accessory muscle, runs from the sternum and clavicle to the mastoid process of the skull. While its primary function is to rotate and flex the neck, it also assists in forceful inspiration. When both SCM muscles contract bilaterally, they elevate the sternum, contributing to the expansion of the thoracic cavity. This action is particularly noticeable during deep inhalation, such as when taking a deep breath before exertion or when breathing is labored. The SCM’s role in breathing is more pronounced in situations where the diaphragm and intercostal muscles are compromised or overworked.
It is important to note that while these accessory muscles are essential for forceful breathing, their prolonged or excessive use can indicate respiratory distress or underlying conditions such as chronic obstructive pulmonary disease (COPD) or asthma. In healthy individuals, these muscles are only minimally active during rest or light activity. However, in individuals with respiratory challenges, the accessory muscles may become visibly active, with movements like shoulder elevation or neck muscle contraction observed during breathing. This is often referred to as "accessory muscle use" and is a clinical sign of increased work of breathing.
In summary, the accessory muscles of the neck and shoulder, particularly the scalene muscles and the sternocleidomastoid, are vital for aiding forceful breathing. Their primary role is to assist the primary muscles of respiration by expanding the thoracic cavity during deep or labored inhalation. While their activation is normal during activities requiring increased ventilation, their excessive use can signal respiratory distress. Understanding the function of these muscles provides insight into the body’s adaptive mechanisms for meeting heightened respiratory demands.
Fever and Muscle Loss: Is There a Link?
You may want to see also
Explore related products





![]()
Exhalation Process: Passive, but abdominal muscles assist in forced exhalation
The exhalation process, often considered passive, relies primarily on the natural recoil of the lungs and chest wall after inhalation. During quiet breathing, the diaphragm and intercostal muscles relax, allowing the elastic tissues of the lungs and thoracic cage to return to their resting position. This recoil expels air from the lungs without requiring active muscular effort. However, during forced exhalation, such as when blowing out candles or exhaling vigorously, additional muscles are recruited to assist in emptying the lungs more completely and rapidly.
The abdominal muscles play a crucial role in forced exhalation. When these muscles contract, they increase the pressure within the abdominal cavity, pushing the diaphragm upward into the thoracic cavity. This upward movement of the diaphragm compresses the lungs further, aiding in the expulsion of air. The primary abdominal muscles involved in this process are the rectus abdominis, transverse abdominis, and the internal and external oblique muscles. Their coordinated contraction ensures a more forceful and controlled exhalation, which is essential in activities like singing, playing wind instruments, or engaging in physical exertion.
In addition to the abdominal muscles, the internal intercostal muscles also contribute to forced exhalation. These muscles, located between the ribs, depress the rib cage when activated, reducing the volume of the thoracic cavity. This reduction in volume increases the pressure within the lungs, facilitating the expulsion of air. While the external intercostal muscles are primarily involved in inhalation, the internal intercostal muscles work in tandem with the abdominal muscles during forced exhalation to enhance the efficiency of the process.
It is important to note that while the abdominal and internal intercostal muscles assist in forced exhalation, the process remains fundamentally passive during normal breathing. The elastic properties of the lungs and chest wall are sufficient for air expulsion under resting conditions. Forced exhalation, however, demonstrates the body's ability to adapt and engage additional musculature to meet increased demands, such as those encountered during physical activity or specific tasks requiring controlled breathing.
Understanding the role of the abdominal muscles in forced exhalation highlights the intricate coordination between different muscle groups in respiratory function. This knowledge is particularly valuable in fields like physiology, sports science, and respiratory therapy, where optimizing breathing mechanics can significantly impact performance and health. By recognizing the passive nature of exhalation and the active assistance provided by the abdominal muscles during forced exhalation, individuals can better appreciate the complexity and adaptability of the respiratory system.
Heart Rate, Muscle Spasms, and Their Connection
You may want to see also
Explore related products






![]()
Bronchioles & Alveoli: Smooth muscles regulate airflow, not primary contraction drivers
The respiratory system is a complex network where various muscles and structures work in harmony to facilitate breathing. When discussing the muscles responsible for lung contraction, it's essential to differentiate between the roles of different muscular components. While the diaphragm and intercostal muscles are the primary drivers of lung expansion and contraction, the bronchioles and alveoli have a distinct function in this process, primarily regulated by smooth muscles.
Bronchioles and Airflow Regulation:
Bronchioles, the smaller branches of the bronchial tree, play a crucial role in controlling airflow within the lungs. These tiny tubes are surrounded by smooth muscles, which are involuntary muscles not under conscious control. When these smooth muscles contract, they narrow the bronchioles, restricting airflow to specific areas of the lungs. This mechanism is vital for directing air to different regions, ensuring efficient gas exchange. Conversely, relaxation of these muscles allows the bronchioles to dilate, increasing airflow. This process is particularly important in response to the body's changing oxygen demands during activities like exercise.
Smooth Muscles and Alveoli:
Alveoli, the microscopic air sacs at the terminal ends of the respiratory tree, are also influenced by smooth muscles. These muscles are not directly responsible for the contraction and expansion of the alveoli but rather play a regulatory role. The smooth muscles surrounding the alveoli can adjust the tension and recoil of the alveolar walls, thereby affecting the overall lung compliance. This mechanism helps maintain the stability of the alveoli, preventing collapse during expiration and ensuring they remain open for gas exchange.
In the context of lung contraction, it is important to emphasize that the primary drivers are the diaphragm and the intercostal muscles. These skeletal muscles actively contract and relax to change the volume of the thoracic cavity, causing the lungs to expand and contract. The smooth muscles in the bronchioles and around the alveoli do not contribute to this volumetric change but rather fine-tune the airflow and maintain alveolar integrity. This distinction is crucial in understanding the intricate coordination of muscles in respiratory physiology.
The regulation of airflow by smooth muscles in the bronchioles is a critical aspect of respiratory function, especially in response to various physiological demands. For instance, during exercise, the body requires increased oxygen intake, prompting the relaxation of bronchiolar smooth muscles to maximize airflow. Conversely, in conditions like asthma, the hyper-responsiveness of these smooth muscles can lead to bronchoconstriction, causing breathing difficulties. Thus, while not directly causing lung contraction, the smooth muscles in the bronchioles and alveoli are essential for optimizing respiratory efficiency and adapting to the body's dynamic needs.
In summary, the bronchioles and alveoli, with their surrounding smooth muscles, are integral to respiratory physiology, but their role is distinct from the primary contraction of the lungs. These smooth muscles act as regulators, ensuring proper airflow distribution and alveolar stability, while the actual contraction and expansion of the lungs are primarily driven by skeletal muscles like the diaphragm. Understanding this differentiation is key to comprehending the intricate mechanics of breathing.
Leg Muscle Pull: Why the Testicular Pain?
You may want to see also
Frequently asked questions
The diaphragm, a dome-shaped muscle located at the base of the lungs, is the primary muscle responsible for contraction during inhalation. It flattens and moves downward, creating a vacuum that pulls air into the lungs.
Yes, the external intercostal muscles, located between the ribs, assist in lung contraction during inhalation. They elevate the ribs and expand the chest cavity, helping to increase lung volume and facilitate air intake.
Yes, during forced exhalation, the internal intercostal muscles and abdominal muscles contract. The internal intercostal muscles lower the ribs, while the abdominal muscles push upward on the diaphragm, forcing air out of the lungs.