Muscle relaxants are essential in various medical settings, from anesthesia to the treatment of muscle spasms and spasticity. Among the different types of muscle relaxants, those acting as receptor agonists are particularly noteworthy. One prominent example is the use of GABAA receptor agonists, such as baclofen, which mimic the action of gamma-aminobutyric acid (GABA), the primary inhibitory neurotransmitter in the central nervous system. By activating GABAA receptors, these agonists enhance inhibitory signaling, leading to reduced neuronal excitability and subsequent muscle relaxation. Another example is the use of glycine receptor agonists, such as dantrolene, which acts directly on skeletal muscle to inhibit calcium release, thereby reducing muscle contraction. Understanding the specific receptor agonists used for muscle relaxation is crucial for optimizing therapeutic outcomes and minimizing side effects in clinical practice.
| Characteristics | Values |
|---|---|
| Receptor Type | GABAA (Gamma-Aminobutyric Acid Type A) |
| Agonist Class | Benzodiazepines, Barbiturates, Non-benzodiazepines (e.g., Z-drugs), and others |
| Mechanism | Enhances the inhibitory effects of GABA, increasing chloride conductance and hyperpolarizing neurons |
| Clinical Use | Muscle relaxation, anxiolysis, sedation, anticonvulsant, and anesthesia |
| Examples | Diazepam, Lorazepam, Midazolam, Baclofen, Tizanidine, and others |
| Onset of Action | Rapid (minutes to hours, depending on route of administration) |
| Duration | Short to intermediate (hours, depending on the specific drug) |
| Side Effects | Drowsiness, dizziness, respiratory depression, dependence, and tolerance |
| Contraindications | Severe respiratory insufficiency, acute alcoholism, and hypersensitivity |
| Metabolism | Hepatic (CYP450 enzymes, primarily CYP3A4) |
| Excretion | Renal (primary route for metabolites) |
| Pregnancy Category | Varies (e.g., Diazepam: D; Baclofen: C) |
| Special Populations | Caution in elderly, hepatic/renal impairment, and pediatric patients |
| Drug Interactions | Enhanced effects with other CNS depressants (e.g., opioids, alcohol) |
| Overdose Management | Supportive care, flumazenil (for benzodiazepine overdose, if indicated) |
| Storage | Room temperature, protected from light and moisture |
| Legal Status | Prescription-only (controlled substance in many regions) |
Explore related products






What You'll Learn
- GABA Receptor Agonists (e.g., baclofen) for spasticity and muscle relaxation
- Glycine Receptor Agonists (e.g., strychnine antagonists) for neuromuscular blockade
- Nicotinic Receptor Antagonists (e.g., succinylcholine) for skeletal muscle relaxation
- Benzodiazepine Receptor Agonists (e.g., diazepam) for central muscle relaxation
- Muscarinic Receptor Antagonists (e.g., atropine) for smooth muscle relaxation
![]()
GABA Receptor Agonists (e.g., baclofen) for spasticity and muscle relaxation
GABA receptor agonists, such as baclofen, are a cornerstone in managing spasticity and promoting muscle relaxation, particularly in conditions like multiple sclerosis, spinal cord injuries, or cerebral palsy. These drugs mimic the action of gamma-aminobutyric acid (GABA), the primary inhibitory neurotransmitter in the central nervous system, to reduce excessive neuronal activity that leads to muscle stiffness and spasms. Baclofen, for instance, acts on GABAB receptors in the spinal cord, dampening the release of excitatory neurotransmitters and thereby decreasing muscle tone.
When prescribing baclofen for spasticity, dosage titration is critical to balance efficacy and side effects. Initial oral doses typically start at 5 mg three times daily, gradually increasing by 5–10 mg every 3–7 days until the desired effect is achieved or side effects become limiting. The maximum daily dose is usually 80 mg, but individual responses vary. For severe cases, intrathecal baclofen delivery via a pump may be considered, offering higher efficacy with lower systemic side effects. Patients should be monitored for drowsiness, dizziness, and weakness, especially during dose adjustments.
Comparatively, baclofen stands out among muscle relaxants for its specificity to spasticity rather than general muscle relaxation. Unlike benzodiazepines or tizanidine, which act more broadly on the nervous system, baclofen’s mechanism is localized to the spinal cord, making it particularly effective for neurologic conditions. However, its side effect profile—including sedation, confusion, and potential withdrawal symptoms with abrupt discontinuation—requires careful patient education and monitoring.
Practical tips for patients include taking baclofen with food to minimize gastrointestinal discomfort and avoiding alcohol, as it can exacerbate sedation. For those on long-term therapy, regular follow-ups are essential to assess spasticity levels, adjust dosages, and screen for tolerance or dependence. Physical therapy should complement pharmacotherapy to maximize functional outcomes, as baclofen alone does not address muscle weakness or atrophy.
In summary, GABA receptor agonists like baclofen are invaluable for managing spasticity, offering targeted relief with careful dosing and monitoring. While not without limitations, their role in improving quality of life for patients with neurologic disorders is undeniable, making them a key tool in the clinician’s arsenal.
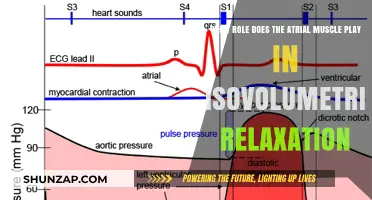
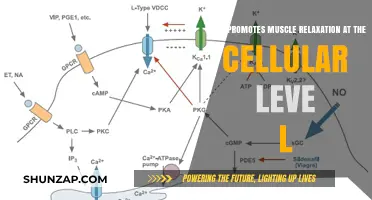
How Relaxing Smooth Muscle Enhances Circulation, Digestion, and Overall Health
You may want to see also
Explore related products






![]()
Glycine Receptor Agonists (e.g., strychnine antagonists) for neuromuscular blockade
Glycine receptor agonists, particularly those acting as strychnine antagonists, offer a unique approach to neuromuscular blockade, leveraging the inhibitory role of glycine in the central nervous system. Unlike traditional muscle relaxants that target nicotinic acetylcholine receptors, these agents enhance glycinergic neurotransmission, leading to hyperpolarization of motor neurons and subsequent muscle relaxation. This mechanism is distinct and holds potential for both therapeutic and anesthetic applications, especially in cases where conventional agents may be contraindicated.
Consider the pharmacological profile of strychnine antagonists, such as d-tubocurarine or its derivatives, which indirectly act as glycine receptor agonists by blocking strychnine’s antagonistic effects. Strychnine itself is a potent glycine receptor antagonist, causing muscle rigidity and convulsions. By administering agents that counteract strychnine’s action, clinicians can induce controlled muscle relaxation. For instance, in surgical settings, a bolus dose of 0.5–1.0 mg/kg of a strychnine antagonist can be titrated to achieve adequate neuromuscular blockade, with careful monitoring of respiratory function due to the drug’s central effects.
One critical advantage of glycine receptor agonists is their potential to minimize cardiovascular side effects, a common limitation of non-depolarizing muscle relaxants. However, their use requires precision, as excessive glycinergic activation can lead to profound central nervous system depression. Pediatric and elderly patients, in particular, may exhibit heightened sensitivity, necessitating dose adjustments—typically 20–30% reductions in children under 12 and cautious titration in patients over 65. Continuous neuromuscular monitoring, such as train-of-four (TOF) stimulation, is essential to avoid over-relaxation and ensure timely reversal.
In practice, combining glycine receptor agonists with adjunctive agents, such as GABA modulators or opioids, can enhance their efficacy while mitigating risks. For example, a low-dose infusion of propofol (50–100 mcg/kg/min) alongside a glycine agonist can provide synergistic sedation and muscle relaxation, reducing the need for higher doses of either agent. Post-procedure, reversal agents like neostigmine or sugammadex should be readily available, though their compatibility with glycinergic blockade requires careful consideration to avoid antagonistic interactions.
While glycine receptor agonists are not yet mainstream in clinical practice, their unique mechanism positions them as a valuable alternative in specific scenarios, such as patients with myasthenia gravis or those resistant to conventional neuromuscular blockers. Ongoing research into selective glycine receptor modulators may further refine their safety and efficacy, paving the way for broader adoption in anesthesia and critical care. For now, their use demands a nuanced understanding of neuropharmacology and vigilant patient monitoring, making them a specialized tool in the muscle relaxant arsenal.
Understanding Muscle Contraction and Relaxation: A Comprehensive Guide
You may want to see also
Explore related products






![]()
Nicotinic Receptor Antagonists (e.g., succinylcholine) for skeletal muscle relaxation
Skeletal muscle relaxation is a critical component of many medical procedures, from intubation to surgery, and nicotinic receptor antagonists like succinylcholine play a pivotal role in achieving this effect. Unlike agonists that activate receptors, antagonists block them, disrupting the neurotransmission necessary for muscle contraction. Succinylcholine, a depolarizing neuromuscular blocking agent, binds to nicotinic acetylcholine receptors at the neuromuscular junction, causing prolonged depolarization that prevents further muscle activation. This mechanism results in rapid, profound muscle relaxation, making it indispensable in emergency and surgical settings.
The administration of succinylcholine requires precision due to its narrow therapeutic window. Typically, a dose of 1–2 mg/kg is given intravenously to induce paralysis within 30–60 seconds, with effects lasting 5–10 minutes. This short duration is both an advantage and a limitation—ideal for brief procedures like rapid sequence intubation but impractical for longer surgeries. Clinicians must also consider contraindications, such as hyperkalemia, burns, or neuromuscular disorders, where succinylcholine can exacerbate potassium release from skeletal muscle, leading to potentially life-threatening arrhythmias.
Comparatively, non-depolarizing nicotinic receptor antagonists like rocuronium and vecuronium offer longer-lasting effects but slower onset times. Succinylcholine’s rapid action, however, remains unmatched for scenarios requiring immediate muscle relaxation. Its use is particularly valuable in emergency medicine, where securing an airway swiftly can be lifesaving. For instance, in cases of severe trauma or status asthmaticus, succinylcholine enables intubation before respiratory compromise becomes irreversible.
Practical considerations for succinylcholine use include monitoring for adverse effects, such as muscle fasciculations, which occur in up to 50% of patients and can be mitigated with pretreatment using small doses of non-depolarizing agents or opioids. Additionally, its use in pediatric patients is generally safe but requires careful dosing adjustments based on age and weight. For adults, the standard dose is well-tolerated, but postoperative myalgia may occur in up to 80% of patients, though it is typically mild and transient.
In conclusion, nicotinic receptor antagonists like succinylcholine are indispensable tools for achieving skeletal muscle relaxation in critical and surgical contexts. Their unique mechanism of action, rapid onset, and short duration make them ideal for specific applications, despite limitations and potential side effects. Understanding their pharmacology, dosing, and contraindications ensures safe and effective use, underscoring their importance in modern anesthesia and emergency medicine.
Mixing Muscle Relaxers and Adderall: Safe or Risky Combination?
You may want to see also
![]()
Benzodiazepine Receptor Agonists (e.g., diazepam) for central muscle relaxation
Benzodiazepine receptor agonists, such as diazepam, are widely recognized for their central muscle relaxant properties, primarily mediated through their interaction with GABA-A receptors in the central nervous system. By enhancing the inhibitory effects of GABA, these agents reduce neuronal excitability, leading to muscle relaxation. This mechanism distinguishes them from peripheral muscle relaxants, which act directly on skeletal muscle or neuromuscular junctions. Diazepam, in particular, is a versatile option, often prescribed for conditions like muscle spasms, spasticity, and anxiety-related muscle tension. Its efficacy stems from its ability to modulate spinal and supraspinal pathways, offering systemic relief without directly affecting muscle fibers.
When considering benzodiazepine receptor agonists for muscle relaxation, dosage and administration are critical. For adults, diazepam is typically initiated at 2–10 mg orally, 2–4 times daily, depending on the severity of symptoms. Elderly patients or those with hepatic impairment may require lower doses, such as 2–5 mg, to minimize sedative effects and risk of accumulation. Intravenous administration (0.1–0.3 mg/kg) is reserved for acute conditions like tetanus or severe muscle spasms, but this route demands careful monitoring due to its rapid onset and potential for respiratory depression. Pediatric dosing is weight-based, generally ranging from 0.1–0.3 mg/kg/day, divided into multiple doses. Always titrate the dose to achieve the minimum effective level, balancing relaxation with functional impairment.
A key advantage of benzodiazepines like diazepam is their dual action as anxiolytics and muscle relaxants, making them particularly useful for patients whose muscle tension is exacerbated by stress or anxiety. For instance, individuals with chronic back pain or fibromyalgia often experience symptom improvement due to diazepam’s ability to alleviate both physical and psychological components of discomfort. However, this benefit must be weighed against potential side effects, including drowsiness, dizziness, and cognitive impairment, which can limit daily activities. Patients should avoid alcohol and other CNS depressants while on therapy, as these combinations potentiate sedation and respiratory risks.
Comparatively, benzodiazepines offer a broader therapeutic profile than other central muscle relaxants, such as baclofen or tizanidine, which primarily target spasticity. However, their long-term use is more contentious due to risks of tolerance, dependence, and withdrawal. For acute or short-term management, diazepam remains a first-line option, especially in cases where muscle relaxation needs to be accompanied by anxiolysis. In chronic settings, clinicians often prefer alternatives or adjunctive therapies to mitigate the risks associated with prolonged benzodiazepine use. Patient education is essential, emphasizing the importance of adhering to prescribed durations and tapering protocols to minimize withdrawal symptoms.
In practice, optimizing the use of diazepam for muscle relaxation involves individualized assessment and monitoring. Start with the lowest effective dose, reassess symptoms regularly, and adjust as needed. Encourage non-pharmacological strategies, such as physical therapy or stress management techniques, to complement pharmacotherapy. For patients with comorbid anxiety, diazepam’s dual action can be particularly advantageous, but prioritize non-benzodiazepine options if anxiety is the primary concern. Finally, maintain open communication with patients about expectations, risks, and alternatives, ensuring informed decision-making in the pursuit of effective muscle relaxation.
Muscle Relaxation Unveiled: The Fascinating Process of Calcium Ion Release
You may want to see also
![]()
Muscarinic Receptor Antagonists (e.g., atropine) for smooth muscle relaxation
Muscarinic receptor antagonists, such as atropine, are pivotal in achieving smooth muscle relaxation by blocking acetylcholine’s action on muscarinic receptors. These receptors, prevalent in the parasympathetic nervous system, mediate involuntary muscle contractions in organs like the gastrointestinal tract, bladder, and airways. By inhibiting these receptors, atropine reduces cholinergic tone, leading to decreased smooth muscle activity. This mechanism is particularly useful in clinical scenarios where excessive muscle spasms or secretions need to be controlled, such as during anesthesia or in gastrointestinal obstructions.
Consider the administration of atropine in preoperative settings. A typical adult dose ranges from 0.5 to 2 mg intravenously, depending on the desired effect and patient response. For pediatric patients, the dosage is weight-based, often calculated as 0.01 to 0.02 mg/kg. It’s crucial to monitor heart rate post-administration, as atropine can cause tachycardia due to its anticholinergic effects. In cases of bradycardia or vagal stimulation, atropine acts as both a therapeutic agent and a diagnostic tool, confirming the cholinergic origin of the condition.
While atropine is effective, its side effects warrant caution. Dry mouth, blurred vision, and urinary retention are common due to widespread muscarinic receptor blockade. In elderly patients, cognitive impairment or delirium may occur, necessitating careful dose titration. Alternatives like glycopyrrolate or ipratropium may be preferred in specific cases, as they have reduced central nervous system penetration and fewer systemic side effects. Always assess the patient’s medical history, particularly for conditions like glaucoma or prostatic hypertrophy, where atropine could exacerbate symptoms.
The comparative advantage of muscarinic antagonists lies in their specificity for smooth muscle relaxation without directly affecting skeletal muscle. Unlike neuromuscular blocking agents, which act at the neuromuscular junction, atropine targets visceral smooth muscle, making it ideal for conditions like irritable bowel syndrome or biliary colic. However, it’s not suitable for skeletal muscle relaxation, highlighting the importance of selecting the right agent for the right muscle type. This distinction underscores the need for precise pharmacological targeting in clinical practice.
In summary, muscarinic receptor antagonists like atropine are indispensable tools for smooth muscle relaxation, particularly in managing cholinergically mediated spasms. Their efficacy, coupled with a clear understanding of dosage, side effects, and contraindications, ensures optimal patient outcomes. Whether in the operating room or outpatient setting, these agents exemplify the intersection of pharmacology and physiology, offering targeted relief with careful consideration of their unique mechanisms and limitations.
Muscle Relaxants for Tight Muscles: Effective Relief or Risky Choice?
You may want to see also
Frequently asked questions
A muscarinic receptor agonist, specifically a cholinergic agonist like acetylcholine, is not used for muscle relaxation. Instead, GABA-A receptor agonists, such as benzodiazepines (e.g., diazepam) or non-benzodiazepines (e.g., zolpidem), and glycine receptor agonists, like baclofen, are used as muscle relaxants.
GABA-A receptor agonists enhance the inhibitory effects of GABA (gamma-aminobutyric acid) in the central nervous system, reducing neuronal excitability. This leads to decreased motor neuron activity, resulting in muscle relaxation.
Glycine receptor agonists, such as baclofen, mimic the action of glycine, an inhibitory neurotransmitter in the spinal cord. By activating glycine receptors, they reduce the transmission of signals from motor neurons to muscles, causing relaxation.
Yes, nicotinic acetylcholine receptor agonists like succinylcholine are used as depolarizing muscle relaxants. They cause prolonged depolarization of the motor endplate, leading to temporary muscle paralysis, commonly used in anesthesia for surgery.