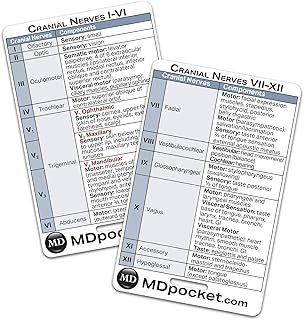
Cranial nerve 11, also known as the accessory nerve, plays a crucial role in controlling specific somatic muscles essential for head and shoulder movements. Primarily, it innervates the sternocleidomastoid muscle, which enables head rotation and tilting, and the trapezius muscle, responsible for shoulder elevation, depression, and scapular stabilization. While the accessory nerve is traditionally associated with these muscles, its function is sometimes shared with the vagus nerve (cranial nerve 10) in certain anatomical variations. Understanding the somatic muscles associated with cranial nerve 11 is vital for diagnosing and treating conditions affecting neck and shoulder mobility, such as nerve injuries or muscular disorders.
| Characteristics | Values |
|---|---|
| Cranial Nerve | XI (Spinal Accessory Nerve) |
| Somatic Muscles Innervated | Sternocleidomastoid (SCM), Trapezius |
| Function of SCM | Rotates head to the opposite side, flexes neck (ipsilateral rotation and flexion) |
| Function of Trapezius | Scapular elevation, depression, upward rotation, and adduction; supports shoulder girdle |
| Origin of Nerve Fibers | Motor fibers originate in the spinal cord (C1-C5) and travel via the cranium |
| Course of Nerve | Exits skull through jugular foramen, travels through the neck to innervate target muscles |
| Clinical Significance | Damage can result in shoulder droop, weakness in head rotation, and scapular winging |
| Embryological Origin | Derived from the basal plate of the embryonic spinal cord |
| Sensory Function | None (purely motor nerve for these muscles) |
| Alternative Names | Accessory nerve, nervus accessorius |
Explore related products





What You'll Learn
- Accessory Nerve Function: CN XI primarily innervates sternocleidomastoid and trapezius muscles for head and shoulder movement
- Sternocleidomastoid Role: Rotates and flexes the head, working with CN XI for lateral neck motion
- Trapezius Function: CN XI controls upper fibers, aiding shoulder elevation and scapular movement
- CN XI Pathway: Originates in spinal cord, travels through jugular foramen to reach muscles
- Clinical Significance: Damage to CN XI causes weakness in head tilt and shoulder shrug
![]()
Accessory Nerve Function: CN XI primarily innervates sternocleidomastoid and trapezius muscles for head and shoulder movement
The accessory nerve, or cranial nerve XI, plays a pivotal role in enabling precise movements of the head and shoulders. Its primary function is to innervate two key muscles: the sternocleidomastoid and the trapezius. These muscles are essential for actions like rotating the head, shrugging the shoulders, and maintaining posture. Understanding their interplay with CN XI is crucial for diagnosing and treating conditions such as nerve damage or muscle weakness.
Anatomical Insight: The sternocleidomastoid muscle, originating from the sternum and clavicle, inserts on the mastoid process of the skull. It acts unilaterally to rotate the head to the opposite side and bilaterally to flex the neck. The trapezius, a broad, flat muscle extending from the occipital bone to the lower thoracic spine, is responsible for shoulder elevation, depression, and scapular stabilization. CN XI’s motor fibers supply these muscles, ensuring coordinated movement. Interestingly, the nerve’s trajectory is unique—it exits the skull through the jugular foramen but also has spinal roots, making it both cranial and spinal in origin.
Practical Implications: For clinicians, assessing CN XI function involves testing these muscles’ strength and symmetry. A simple test for the sternocleidomastoid is to ask the patient to turn their head against resistance. Trapezius function can be evaluated by instructing the patient to shrug their shoulders or resist downward pressure. Weakness or atrophy in these muscles may indicate accessory nerve damage, often seen in trauma cases, such as brachial plexus injuries or surgical complications. Early detection is key, as rehabilitation strategies, including physical therapy and targeted exercises, can improve outcomes.
Comparative Perspective: Unlike other cranial nerves that innervate multiple muscle groups or sensory functions, CN XI is almost exclusively motor-focused. This specialization underscores its importance in gross motor control. While cranial nerves like V (trigeminal) and VII (facial) have both sensory and motor components, CN XI’s role is singular yet indispensable. Its vulnerability in certain medical procedures, such as neck surgeries, highlights the need for precision to avoid long-term deficits.
Takeaway for Daily Life: Awareness of CN XI’s function can benefit not just medical professionals but also individuals seeking to maintain neck and shoulder health. Incorporating exercises like neck rotations, shoulder shrugs, and scapular squeezes into daily routines can strengthen the sternocleidomastoid and trapezius. For those experiencing persistent pain or weakness in these areas, consulting a healthcare provider for a thorough neurological evaluation is advisable. By understanding CN XI’s role, one can better appreciate the intricate balance of the nervous and muscular systems in everyday movement.
Cable Chest Fly Muscles: Targeted Workout for Upper Body Strength
You may want to see also
Explore related products






![]()
Sternocleidomastoid Role: Rotates and flexes the head, working with CN XI for lateral neck motion
The sternocleidomastoid muscle, a robust strap-like structure, plays a pivotal role in head and neck movement, particularly in conjunction with cranial nerve XI (CN XI), also known as the accessory nerve. This muscle's function is both precise and essential, allowing for a range of motions that are fundamental to our daily activities.
Understanding the Mechanism:
When CN XI stimulates the sternocleidomastoid, it initiates a series of actions. Primarily, it facilitates the rotation of the head, enabling us to turn our faces from side to side. This movement is crucial for activities like checking blind spots while driving or simply looking over one's shoulder. Additionally, the muscle contributes to head flexion, the action of nodding, which is integral to various physical tasks and non-verbal communication.
Practical Implications:
For individuals experiencing neck pain or stiffness, understanding the sternocleidomastoid's role can be beneficial. Stretching and strengthening exercises targeting this muscle can provide relief and improve mobility. A simple stretch involves gently tilting the head to the side, using the sternocleidomastoid to initiate the movement, and holding for 15–30 seconds. This can be repeated several times daily to alleviate tension.
A Comparative Perspective:
Interestingly, the sternocleidomastoid's function contrasts with other neck muscles. While it primarily rotates and flexes, muscles like the scalene group are more involved in lateral flexion and assisting in breathing. This differentiation highlights the specialized roles of various muscles in the neck, each contributing uniquely to overall head and neck mobility.
Clinical Relevance:
In medical practice, assessing the sternocleidomastoid's function is vital. Weakness or atrophy of this muscle can indicate potential issues with CN XI, which may arise from trauma or neurological disorders. Healthcare professionals often test its strength by asking patients to resist head rotation, providing valuable insights into the nerve's integrity. This simple yet effective examination underscores the muscle's significance in clinical diagnostics.
Explosive Push Ups: Targeted Muscles for Power and Strength
You may want to see also
Explore related products






![]()
Trapezius Function: CN XI controls upper fibers, aiding shoulder elevation and scapular movement
Cranial nerve XI, also known as the accessory nerve, plays a pivotal role in controlling specific muscles essential for upper body movement. Among these, the trapezius muscle stands out, particularly its upper fibers, which are directly innervated by CN XI. This relationship is crucial for functions like shoulder elevation and scapular movement, which are fundamental to daily activities such as lifting, reaching, and maintaining posture. Understanding this interplay between nerve and muscle not only highlights the precision of the nervous system but also underscores the importance of CN XI in upper body mechanics.
Analyzing the trapezius function reveals a nuanced division of labor within the muscle itself. The upper fibers, under CN XI’s control, are primarily responsible for elevating the scapula and rotating it laterally, movements essential for overhead activities. In contrast, the middle and lower fibers, innervated by the spinal accessory nerve, focus on scapular adduction and depression. This specialization allows for coordinated, efficient motion, demonstrating how CN XI’s role is both specific and indispensable. For instance, during a shoulder press, the upper trapezius fibers contract to stabilize and elevate the scapula, ensuring smooth and controlled movement.
From a practical standpoint, maintaining the health of CN XI and the upper trapezius fibers is vital for athletes, manual laborers, and anyone engaged in repetitive upper body tasks. Strengthening exercises like shrugs, upright rows, and scapular retractions can enhance muscle function and prevent injury. However, caution must be exercised to avoid overloading the muscle, as excessive strain can lead to conditions like trapezius strain or impingement. Incorporating stretching routines post-activity can also alleviate tension and improve flexibility, ensuring longevity in muscle performance.
Comparatively, the role of CN XI in trapezius function contrasts with its involvement in the sternocleidomastoid muscle, which primarily controls head rotation and tilt. This distinction highlights the accessory nerve’s dual responsibilities and its adaptability in managing diverse muscular functions. While the sternocleidomastoid’s actions are more localized, the trapezius’s upper fibers contribute to broader, more dynamic movements, emphasizing CN XI’s versatility in supporting both fine and gross motor skills.
In conclusion, the upper fibers of the trapezius, controlled by CN XI, are integral to shoulder elevation and scapular movement, enabling essential daily and specialized activities. By understanding this relationship, individuals can better target their training, prevent injuries, and appreciate the intricate coordination between nerves and muscles. Whether through targeted exercises or mindful movement practices, optimizing CN XI and trapezius function ensures a stronger, more resilient upper body.
Horse Stance Benefits: Targeted Muscles and Strength Training Explained
You may want to see also
Explore related products






![]()
CN XI Pathway: Originates in spinal cord, travels through jugular foramen to reach muscles
Cranial nerve XI, also known as the accessory nerve, plays a pivotal role in controlling specific somatic muscles essential for head and shoulder movement. Its pathway is unique among cranial nerves, originating in the spinal cord and traversing through the jugular foramen to innervate its target muscles. This distinct route underscores its dual spinal and cranial nature, making it a fascinating subject of anatomical study.
To understand the CN XI pathway, begin by visualizing the spinal cord, where the nerve’s motor nucleus resides in the upper cervical segments (C1-C5). From here, the nerve fibers ascend and exit the spinal cord, merging with the cranial component of the accessory nerve. This combined nerve then travels cranially, passing through the jugular foramen—a bony opening at the base of the skull—to reach its destination. This journey highlights the nerve’s critical role in bridging the spinal and cranial regions, a feature that sets it apart from other cranial nerves.
The muscles innervated by CN XI are primarily the sternocleidomastoid (SCM) and trapezius. The SCM, responsible for rotating and flexing the head, receives its motor supply from the spinal component of CN XI. The trapezius, which stabilizes and moves the scapula, is also innervated by this nerve, though its function can be compromised in cases of CN XI damage. Clinicians often assess these muscles to diagnose accessory nerve injuries, which may result from trauma to the jugular foramen or neck region.
Practical tips for evaluating CN XI function include observing shoulder shrug strength (trapezius) and head tilt resistance (SCM). Weakness in these actions may indicate nerve damage, warranting further investigation. For patients with suspected CN XI injury, imaging studies like MRI or CT scans can confirm structural abnormalities in the jugular foramen or surrounding tissues. Early detection and targeted rehabilitation, such as physical therapy focusing on scapular stabilization, can improve outcomes for affected individuals.
In summary, the CN XI pathway exemplifies the intricate interplay between the spinal cord and cranial structures. Its route through the jugular foramen to innervate the SCM and trapezius underscores its functional significance in head and shoulder movement. Understanding this pathway not only enriches anatomical knowledge but also equips practitioners with the tools to diagnose and manage related conditions effectively.
Magnesium as a Muscle Relaxer: Fact or Fiction?
You may want to see also
Explore related products






![]()
Clinical Significance: Damage to CN XI causes weakness in head tilt and shoulder shrug
Cranial nerve XI, also known as the accessory nerve, plays a pivotal role in controlling specific somatic muscles essential for head and shoulder movements. Damage to this nerve can lead to noticeable deficits, particularly in the ability to tilt the head and shrug the shoulders. These seemingly simple actions are underpinned by the intricate innervation of the sternocleidomastoid and trapezius muscles, which are primarily supplied by CN XI. Understanding the clinical significance of CN XI damage requires a closer look at the functional anatomy and the practical implications of its impairment.
Consider the sternocleidomastoid muscle, a paired structure running from the sternum and clavicle to the mastoid process of the skull. It is responsible for rotating and flexing the head, enabling actions like tilting the head sideways. When CN XI is damaged, the sternocleidomastoid’s function is compromised, leading to weakness or inability to perform these movements. For instance, a patient with CN XI injury may struggle to turn their head to look over their shoulder, a task critical for activities like driving or scanning surroundings. This deficit can be assessed clinically by asking the patient to rotate their head against resistance, where weakness or asymmetry becomes apparent.
The trapezius muscle, another key player innervated by CN XI, is crucial for shoulder shrugging and scapular stabilization. Damage to the nerve results in trapezius weakness, manifesting as difficulty lifting the shoulders or maintaining proper scapular position. This impairment is not merely cosmetic; it affects functional activities like carrying objects, reaching overhead, or even maintaining posture. Clinicians often test trapezius function by instructing patients to shrug their shoulders against resistance, noting any asymmetry or weakness. Early identification of trapezius involvement is vital, as it may indicate more extensive nerve damage or underlying pathology.
From a practical standpoint, managing CN XI damage requires a multidisciplinary approach. Physical therapy plays a central role, focusing on strengthening compensatory muscles and improving range of motion. For example, exercises like isometric neck rotations or scapular retractions can help maintain function. In severe cases, surgical intervention may be considered to repair nerve damage, though outcomes vary based on the extent and location of the injury. Patients should also be educated on ergonomic adjustments, such as using supportive neck rests or modifying activities to minimize strain on weakened muscles.
In summary, damage to CN XI has profound clinical implications, particularly in the context of head tilt and shoulder shrug weakness. Recognizing these deficits early allows for targeted interventions, from therapeutic exercises to surgical options. By understanding the specific roles of the sternocleidomastoid and trapezius muscles, clinicians can tailor treatment plans to restore function and improve quality of life for affected individuals. This nuanced approach underscores the importance of CN XI in daily activities and the need for precise assessment and management.
Quad Stretch Benefits: Targeted Muscles and Flexibility Explained
You may want to see also
Frequently asked questions
Cranial Nerve 11, also known as the accessory nerve, primarily innervates the sternocleidomastoid (SCM) and trapezius muscles, which are somatic muscles responsible for neck and shoulder movements.
The sternocleidomastoid (SCM) muscle, innervated by Cranial Nerve 11, is responsible for rotating and flexing the head, as well as stabilizing the neck during movement.
The trapezius muscle, also innervated by Cranial Nerve 11, is involved in shoulder elevation, scapular retraction, and head extension, playing a key role in upper back and neck movements.
No, Cranial Nerve 11 primarily innervates only the sternocleidomastoid and trapezius muscles. Other cranial nerves, such as Cranial Nerve 10 (vagus nerve), have additional functions but do not innervate somatic muscles.
Damage to Cranial Nerve 11 can result in weakness or paralysis of the sternocleidomastoid and trapezius muscles, leading to difficulty in moving the head, neck, and shoulders, as well as potential shoulder drooping.