Breast implants are a popular cosmetic procedure designed to enhance the size, shape, or symmetry of the breasts. While the implants themselves are placed beneath the breast tissue or chest muscle, the procedure primarily involves the pectoralis major muscle in cases where the implant is positioned subpectorally (under the muscle). This muscle group, which includes the pectoralis major and sometimes the serratus anterior for optimal contouring, plays a crucial role in achieving a natural appearance and stability of the implant. Understanding the interaction between breast implants and these muscle groups is essential for both surgeons and patients, as it influences the surgical approach, recovery process, and final aesthetic outcome.
Explore related products






What You'll Learn
- Pectoral Muscle Anatomy: Understanding the chest muscles' role in breast implant placement and positioning
- Submuscular vs. Subglandular: Comparing implant placement under or over the pectoral muscle
- Muscle Recovery Post-Surgery: Healing and strengthening the pectoral muscles after breast augmentation
- Implant Rippling Risk: How muscle coverage affects visibility of breast implant rippling
- Exercise Restrictions: Guidelines for pectoral muscle workouts post-breast implant surgery
![]()
Pectoral Muscle Anatomy: Understanding the chest muscles' role in breast implant placement and positioning
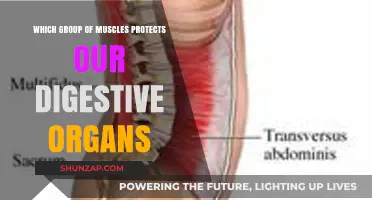
The pectoral muscles, specifically the pectoralis major, play a pivotal role in breast implant surgery, influencing both the aesthetic outcome and the structural integrity of the procedure. Understanding the anatomy of these muscles is crucial for surgeons to determine the optimal placement and positioning of implants. The pectoralis major, a fan-shaped muscle covering the upper chest, is divided into two heads: the clavicular (upper) and the sternal (lower). During implant placement, surgeons often consider whether to position the implant above (subglandular) or below (submuscular) this muscle, a decision that significantly affects the final appearance and feel of the breasts.
From an analytical perspective, submuscular placement, where the implant is positioned beneath the pectoralis major, offers several advantages. This technique provides better coverage for the implant, reducing the risk of visible rippling or edges, especially in patients with thin tissue. It also tends to result in a more natural contour, as the muscle helps to shape and support the implant. However, this approach can lead to increased postoperative pain and animation deformity, where the breast moves or changes shape with certain chest movements. Surgeons must carefully assess the patient’s anatomy, lifestyle, and desired outcome to determine if submuscular placement is the best choice.
Instructively, patients considering breast implants should be aware of how their pectoral muscles may impact recovery and long-term results. For instance, individuals with well-developed pectoral muscles, such as athletes or fitness enthusiasts, may experience more pronounced animation deformity with submuscular placement. In such cases, subglandular placement might be recommended, though this carries its own risks, including higher visibility of the implant and increased capsular contracture rates. Engaging in open discussions with a board-certified plastic surgeon can help patients make informed decisions tailored to their unique anatomy and goals.
Comparatively, the role of the pectoral muscles in breast implant surgery highlights the importance of personalized surgical planning. While submuscular placement often yields more natural results, it may not be suitable for everyone. Subglandular placement, on the other hand, offers a quicker recovery and less postoperative discomfort but may lack the same level of naturalness. Additionally, partial submuscular placement, where only the upper portion of the implant is covered by the pectoralis major, has emerged as a compromise, minimizing animation deformity while maintaining adequate coverage. This technique underscores the need for surgeons to adapt their approach based on individual patient factors.
Practically, patients can take steps to optimize their outcomes by understanding their pectoral muscle anatomy. For example, those with significant pectoral development may benefit from preoperative consultations focused on minimizing animation deformity. Postoperatively, avoiding strenuous chest exercises for 4–6 weeks can help ensure proper healing and reduce the risk of complications. Additionally, wearing a supportive surgical bra and following the surgeon’s specific aftercare instructions are essential for achieving the best possible results. By recognizing the interplay between pectoral muscle anatomy and implant placement, patients can approach breast augmentation with greater confidence and clarity.
Master Muscle Groups with Fun and Engaging Learning Games
You may want to see also
Explore related products

$19.99 $27.99





![]()
Submuscular vs. Subglandular: Comparing implant placement under or over the pectoral muscle
Breast implant placement is a critical decision that influences not only the aesthetic outcome but also the recovery process and long-term comfort. The two primary options—submuscular (under the pectoral muscle) and subglandular (over the muscle)—each offer distinct advantages and drawbacks. Understanding these differences is essential for anyone considering breast augmentation.
Submuscular placement involves positioning the implant beneath the pectoral muscle, which can provide a more natural contour, especially in individuals with minimal breast tissue. This method is often recommended for athletes or those with active lifestyles, as it reduces the risk of visible implant edges and rippling. However, the trade-off is a potentially longer and more painful recovery period, as the muscle must heal around the implant. For instance, patients may experience discomfort during upper body movements for several weeks post-surgery. To manage pain, surgeons often prescribe a combination of opioids and anti-inflammatory medications, though patients should be cautious of dosage to avoid dependency.
In contrast, subglandular placement positions the implant directly behind the breast tissue but above the pectoral muscle. This approach typically results in a quicker recovery, as the muscle remains undisturbed. It’s ideal for those seeking a more pronounced augmentation, as the implant sits closer to the surface, enhancing projection. However, this method carries a higher risk of visible rippling, particularly in thin patients or those with low body fat. Additionally, subglandular implants may interfere with mammography readings, requiring specialized imaging techniques to ensure accurate breast cancer screening.
The choice between submuscular and subglandular placement often hinges on individual anatomy, lifestyle, and aesthetic goals. For example, a 25-year-old marathon runner with minimal breast tissue might opt for submuscular placement to maintain a natural look and avoid implant visibility during physical activity. Conversely, a 40-year-old patient seeking a dramatic enhancement with sufficient breast tissue might prefer subglandular placement for its immediate results and shorter recovery time.
Ultimately, consulting with a board-certified plastic surgeon is crucial to determine the most suitable option. Factors such as skin elasticity, existing breast tissue, and personal preferences play a significant role in this decision. While submuscular placement offers a more natural appearance and reduced rippling, subglandular placement provides quicker recovery and enhanced projection. Both methods have their merits, and the right choice depends on balancing individual priorities with professional guidance.
Is Weekly Muscle Group Training Enough for Optimal Growth?
You may want to see also
Explore related products






![]()
Muscle Recovery Post-Surgery: Healing and strengthening the pectoral muscles after breast augmentation
Breast augmentation often involves the pectoral muscles, particularly when implants are placed beneath them. Post-surgery, these muscles require targeted care to heal and regain strength. The pectoral muscles, essential for arm movement and chest stability, can experience strain or atrophy after being manipulated during the procedure. Understanding their role and recovery process is crucial for optimal healing and long-term functionality.
Phase 1: Immediate Post-Surgical Care (0–2 Weeks)
In the first two weeks, focus on minimizing strain and promoting blood flow to the pectorals. Avoid lifting anything heavier than 5–10 pounds, as this can disrupt healing. Gentle arm swings and shoulder rolls, performed 3–4 times daily, help maintain mobility without engaging the pectorals directly. Ice packs applied for 15–20 minutes, 3–4 times daily, reduce swelling and discomfort. Over-the-counter anti-inflammatory medications, such as ibuprofen (200–400 mg every 6–8 hours), can alleviate pain but should be used cautiously to avoid prolonged healing delays.
Phase 2: Gradual Strengthening (2–6 Weeks)
As pain subsides, introduce light resistance exercises to reactivate the pectorals. Wall pushes, performed 2–3 times daily for 10–15 repetitions, gently engage the muscles without overexertion. Use a resistance band for horizontal chest presses, starting with 1–2 sets of 8–10 reps. Gradually increase resistance as tolerated. Avoid traditional push-ups or bench presses during this phase, as they can strain the healing muscles. Consistency is key; aim for daily movement to prevent stiffness and promote muscle memory.
Phase 3: Advanced Strengthening (6–12 Weeks)
By week six, most patients can begin more targeted pectoral exercises. Incline dumbbell presses, starting with light weights (5–10 pounds), help rebuild strength. Incorporate eccentric exercises, such as slow lowering during presses, to enhance muscle repair. Yoga or Pilates movements like modified planks or cat-cow stretches improve flexibility and stability. Always prioritize form over intensity to avoid injury. Consult a physical therapist or trainer for personalized guidance, especially if asymmetry or weakness persists.
Long-Term Maintenance (12+ Weeks)
After three months, the pectorals should be sufficiently healed to handle regular strength training. Incorporate compound exercises like push-ups, bench presses, and chest flies into your routine, gradually increasing weight and reps. Maintain a balanced approach by including back and shoulder exercises to prevent muscle imbalances. Regular massage or foam rolling can alleviate scar tissue buildup and improve muscle function. Listen to your body—persistent pain or discomfort warrants a medical evaluation.
Practical Tips for Success
Stay hydrated and consume a protein-rich diet (aim for 1.2–1.6 g/kg of body weight daily) to support muscle repair. Wear a supportive surgical bra as recommended by your surgeon to minimize pectoral strain. Track progress with weekly photos or strength measurements to stay motivated. Patience is paramount; full recovery can take up to six months, depending on individual factors like age, fitness level, and surgical technique. With consistent care, the pectorals will regain their strength, ensuring both aesthetic and functional success post-augmentation.
Understanding Muscle Group Separation: Anatomy, Function, and Training Insights
You may want to see also
Explore related products






![]()
Implant Rippling Risk: How muscle coverage affects visibility of breast implant rippling
Breast implant rippling occurs when the implant’s edges or folds become visible or palpable through the skin, often resembling waves or ridges. This phenomenon is more common with saline implants but can also occur with silicone, particularly in thin patients or those with minimal tissue coverage. The primary factor influencing visibility is the degree of muscle coverage over the implant. Submuscular placement, where the implant is positioned beneath the pectoralis major muscle, provides a thicker barrier that reduces rippling compared to subglandular placement, where the implant sits directly behind breast tissue. However, even with submuscular placement, inadequate muscle thickness or tension can leave areas vulnerable to rippling, especially in the upper pole or along the sides of the breast.
To minimize rippling risk, surgeons often assess muscle anatomy and patient characteristics preoperatively. For instance, women with well-developed pectoralis muscles and sufficient subcutaneous fat are less likely to experience visible rippling. In contrast, athletes or individuals with low body fat may require additional measures, such as using textured implants or adding acellular dermal matrix (ADM) to increase tissue coverage. Textured implants adhere to surrounding tissues, reducing movement that can cause rippling, while ADM acts as a scaffold to support and thicken the overlying tissue. However, these solutions are not foolproof and must be tailored to the patient’s anatomy and lifestyle.
Patients considering breast augmentation should be educated about the trade-offs between implant placement options. Submuscular placement, though reducing rippling, can distort implant shape during muscle contraction, particularly in active individuals. Subglandular placement preserves natural movement but increases rippling risk, especially with saline implants. Hybrid techniques, such as partial submuscular placement, offer a compromise by covering the upper pole with muscle while allowing the lower implant to move freely. Postoperative care, including avoiding excessive muscle strain during healing, can also mitigate rippling by ensuring proper tissue settling and scar maturation.
For those already experiencing rippling, revision surgery may be necessary. Options include switching to a higher-profile implant to stretch the tissue, converting from saline to silicone implants, or adding fat grafting to increase soft tissue coverage. Fat grafting, in particular, can address localized rippling by providing a natural, long-lasting layer of tissue over the implant. However, this approach requires sufficient donor fat and may involve multiple sessions for optimal results. Patients should discuss their concerns with a board-certified plastic surgeon to explore the most effective solution based on their unique anatomy and goals.
Ultimately, understanding the relationship between muscle coverage and implant rippling is crucial for both surgeons and patients. While submuscular placement remains the gold standard for reducing rippling, it is not a one-size-fits-all solution. Factors such as muscle thickness, implant type, and patient lifestyle must be considered to achieve the best outcome. By combining careful preoperative planning with advanced techniques and patient education, the risk of visible rippling can be significantly minimized, ensuring a more natural and satisfying result.
Is the Chest a Major Muscle Group? Unveiling the Truth
You may want to see also
Explore related products






![]()
Exercise Restrictions: Guidelines for pectoral muscle workouts post-breast implant surgery
Breast implant surgery, whether for augmentation or reconstruction, significantly impacts the pectoral muscles, which are integral to chest movement and stability. Post-surgery, these muscles require careful management to ensure proper healing and to avoid complications. Pectoral muscle workouts, in particular, must be approached with caution to prevent implant displacement, muscle strain, or capsular contracture. Understanding the timeline and types of exercises permissible is crucial for a safe recovery.
Initial Recovery Phase (0–6 Weeks): During the first six weeks post-surgery, the focus should be on minimizing strain on the pectoral muscles. Avoid any exercises that involve pushing, pulling, or lifting weights, as these actions directly engage the pectoralis major and minor. Even activities like push-ups, bench presses, or chest flies can compromise the surgical site. Instead, prioritize gentle movements that maintain mobility without exerting pressure on the chest. Light walking and upper-body stretches (excluding the chest area) are recommended to promote blood flow and prevent stiffness. Patients should also wear a supportive surgical bra to stabilize the implants and reduce muscle tension.
Gradual Reintroduction (6–12 Weeks): After the initial six weeks, patients can begin reintroducing light pectoral exercises, but with strict modifications. Start with isometric contractions, such as wall presses or gentle chest squeezes using a soft ball, to activate the muscles without causing strain. Avoid adding resistance or weights during this phase. Range-of-motion exercises, like arm circles or shoulder rolls, can also help restore flexibility. It’s essential to monitor for pain, swelling, or unusual sensations, as these may indicate overexertion. Consult with a surgeon or physical therapist before advancing to ensure the healing process is on track.
Advanced Strengthening (12+ Weeks): Beyond 12 weeks, patients may gradually incorporate more traditional pectoral exercises, but with caution. Begin with bodyweight exercises like modified push-ups (on an incline or against a wall) before progressing to light dumbbell presses or machine-based chest workouts. Avoid heavy lifting or high-intensity activities until at least 16 weeks post-surgery, as the implants and surrounding tissues need ample time to settle. Always prioritize proper form and listen to your body’s signals. Overloading the pectoral muscles too soon can lead to long-term complications, including implant malposition or tissue damage.
Long-Term Considerations: Even after full recovery, patients should remain mindful of how pectoral workouts affect their implants. High-impact activities or exercises involving repetitive chest compression (e.g., boxing or weightlifting) may require adjustments to reduce strain. Regular check-ins with a healthcare provider can help monitor implant stability and address any concerns early. Additionally, maintaining overall upper-body strength, including the back and shoulders, can provide better support for the chest area and reduce the risk of complications.
In summary, pectoral muscle workouts post-breast implant surgery require a phased, cautious approach to ensure optimal healing and long-term results. By adhering to these guidelines and staying attuned to your body’s needs, patients can safely regain strength and mobility without compromising their surgical outcomes.
Exploring the Body's Tiniest Muscle Group: A Comprehensive Guide
You may want to see also
Frequently asked questions
The pectoral muscle, specifically the pectoralis major, is commonly used for breast implant placement, particularly in submuscular or dual plane techniques.
Placing implants under the muscle (submuscular) provides better coverage, reduces the risk of visible rippling, and can yield a more natural appearance, especially in patients with minimal breast tissue.
Yes, submuscular placement can temporarily limit chest workouts post-surgery, as the pectoral muscles need time to heal. However, most patients can resume normal exercise routines after proper recovery.
Yes, implants can be placed over the muscle (subglandular), which may result in a quicker recovery and less post-operative pain, but it’s typically recommended for patients with sufficient natural breast tissue to avoid visible rippling.
Muscle coverage can help reduce the risk of complications like capsular contracture and implant visibility, potentially increasing the longevity and aesthetic outcome of breast implants.