The question of which muscle is the prime mover of arm abduction is a fundamental topic in anatomy and kinesiology, as it involves understanding the primary muscle responsible for lifting the arm away from the body in the frontal plane. Arm abduction is a common movement in daily activities and exercises, making it essential to identify the muscle that plays the most significant role in this action. Among the various muscles involved, the deltoid muscle, particularly its middle fibers, is widely recognized as the prime mover of arm abduction, working in conjunction with other muscles like the supraspinatus to initiate and control this movement efficiently.
| Characteristics | Values |
|---|---|
| Muscle Name | Supraspinatus |
| Prime Function | Arm abduction (initiates the movement) |
| Origin | Supraspinous fossa of the scapula |
| Insertion | Greater tubercle of the humerus |
| Nerve Supply | Suprascapular nerve (C5-C6) |
| Action | Abducts the arm from 0° to 15° |
| Secondary Actions | Stabilizes the glenohumeral joint |
| Antagonist Muscle | Latissimus dorsi, teres major, pectoralis major |
| Blood Supply | Suprascapular artery |
| Common Injuries | Rotator cuff tears, impingement syndrome |
| Training Exercises | Lateral raises, empty cans, cable abduction |
| Location | Posterior shoulder region |
| Shape | Triangular |
| Fiber Direction | Horizontal |
| Synergists | Deltoid (middle fibers), trapezius |
Explore related products






What You'll Learn
![]()
Role of Supraspinatus Muscle
The supraspinatus muscle, though small in size, plays a pivotal role in the complex movement of arm abduction. Nestled within the supraspinous fossa of the scapula, it is one of the four rotator cuff muscles, but its function extends beyond mere stabilization. During the initial phase of arm abduction, the supraspinatus is the primary initiator, lifting the arm from the resting position to approximately 15 degrees. This initial movement is crucial, as it sets the stage for other muscles, such as the deltoid, to take over and continue the abduction process up to 180 degrees. Without the supraspinatus, even the simplest tasks like reaching for a shelf or waving goodbye would be significantly impaired.
To understand the supraspinatus’s role, consider its anatomical positioning and nerve supply. It originates from the supraspinous fossa and inserts on the greater tubercle of the humerus, with the suprascapular nerve providing innervation. This nerve is particularly vulnerable to compression, especially at the suprascapular notch, which can lead to supraspinatus weakness or atrophy. For individuals experiencing shoulder pain or limited range of motion, assessing the integrity of the suprascapular nerve is essential. Practical tip: If you suspect supraspinatus dysfunction, avoid repetitive overhead activities and incorporate gentle isometric exercises, such as wall pushes, to strengthen the muscle without exacerbating injury.
Comparatively, while the deltoid muscle is often credited as the main abductor of the arm, it relies on the supraspinatus to initiate the movement smoothly. This interdependence highlights the supraspinatus’s unique role as both a stabilizer and a prime mover in the early stages of abduction. For athletes or individuals engaged in activities requiring frequent arm elevation, such as swimming or weightlifting, maintaining supraspinatus health is critical. Incorporating resistance band exercises, like external rotation at 90 degrees of abduction, can help reinforce its function and prevent imbalances.
A persuasive argument for prioritizing supraspinatus care lies in its susceptibility to injury, particularly in aging populations. Studies show that supraspinatus tears are among the most common causes of shoulder pain in adults over 50, often due to degenerative changes or chronic overuse. Early intervention, such as physical therapy focusing on rotator cuff strengthening, can mitigate long-term damage. For older adults, low-impact exercises like scapular retractions or prone horizontal abduction are recommended to enhance muscle endurance without strain.
In conclusion, the supraspinatus muscle’s role in arm abduction is both specialized and indispensable. Its ability to initiate movement, stabilize the shoulder joint, and work synergistically with other muscles underscores its importance in daily function and athletic performance. By understanding its mechanics and vulnerabilities, individuals can adopt targeted strategies to preserve its health, ensuring optimal shoulder mobility and strength throughout life.
Arm Wrestling Muscles: Key Strengths for Dominating the Table
You may want to see also
Explore related products






![]()
Deltoid Muscle Function in Abduction
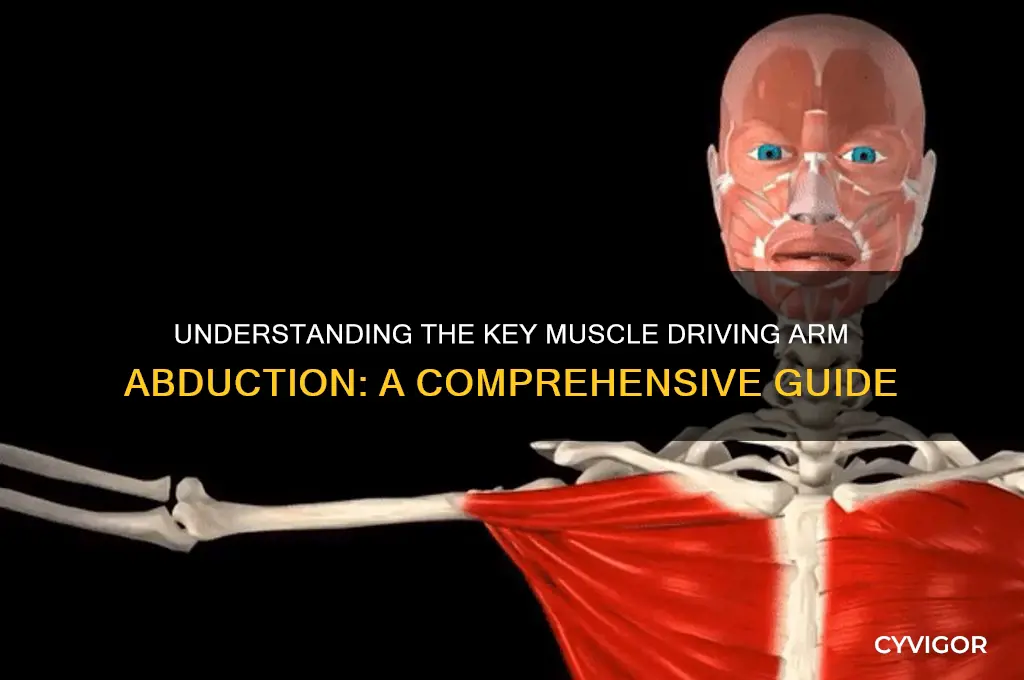
The deltoid muscle, a triangular powerhouse capping the shoulder, is the undisputed prime mover of arm abduction. This action, lifting the arm away from the body in the frontal plane, is fundamental to countless daily activities, from reaching for a shelf to waving hello.
While other muscles assist, the deltoid's unique anatomical structure and fiber orientation make it the primary driver of this movement.
Anatomically, the deltoid comprises three distinct heads: anterior (front), lateral (side), and posterior (rear). During abduction, the lateral head takes center stage. Its fibers run nearly perpendicular to the humerus, creating the ideal mechanical advantage for lifting the arm. As the deltoid contracts, it pulls the humerus outward, overcoming gravity and resistance. This action is most powerful in the initial 0-90 degrees of abduction, with the lateral head contributing the majority of the force.
Beyond 90 degrees, the supraspinatus muscle of the rotator cuff becomes more prominent, assisting in further elevation.
Understanding deltoid function in abduction has practical implications for training and rehabilitation. For athletes seeking to improve overhead pressing strength or throwing power, targeted deltoid exercises like lateral raises are essential. These exercises should focus on controlled movements through the full range of motion, emphasizing the 0-90 degree arc where the deltoid is most active. It's crucial to maintain proper form, avoiding excessive weight that could compromise shoulder stability.
For individuals recovering from shoulder injuries, gradual strengthening of the deltoid is vital for restoring functional abduction and preventing future problems.
Interestingly, the deltoid's role in abduction isn't solely about brute strength. It also contributes to shoulder stability, working in conjunction with the rotator cuff muscles to maintain the humeral head within the glenoid fossa during movement. This dynamic interplay highlights the deltoid's multifaceted role in shoulder function, going beyond simple abduction to ensure smooth and controlled arm movements in all directions.
Master Arm Wrestling: Key Muscles to Train for Strength & Power
You may want to see also
Explore related products






![]()
Scapular Stabilization During Movement
The supraspinatus muscle is widely recognized as the prime mover of arm abduction, initiating the movement by lifting the arm away from the body. However, this action is not isolated; it relies heavily on scapular stabilization to ensure efficient and safe movement. Without proper stabilization of the scapula, arm abduction can lead to compensatory patterns, decreased performance, and even injury. This interdependence highlights the critical role of the scapula as a stable base for upper extremity function.
Consider the kinetic chain during arm abduction: as the arm lifts, the scapula must upwardly rotate and posteriorly tilt to maintain optimal positioning. This movement is facilitated by the coordinated efforts of several muscles, including the serratus anterior, lower trapezius, and rhomboids. The serratus anterior, for instance, acts to protract and upwardly rotate the scapula, while the lower trapezius and rhomboids provide posterior tilt and retraction. Dysfunction in any of these muscles can disrupt scapular stability, leading to abnormal movement patterns such as scapular winging or dyskinesis.
To enhance scapular stabilization during arm abduction, targeted exercises can be incorporated into training routines. For example, the wall slide with external rotation strengthens the lower trapezius and serratus anterior while promoting proper scapular positioning. Begin by standing with your back against a wall, elbows bent at 90 degrees, and forearms against the wall. Slide your arms overhead while maintaining contact with the wall, then return to the starting position. Perform 2–3 sets of 10–15 repetitions, focusing on controlled movement and scapular engagement. Another effective exercise is the scapular push-up, which emphasizes serratus anterior activation. From a plank position, lower your body while protracting your scapula (pushing them away from your spine), then return to the starting position. Aim for 3 sets of 8–12 repetitions, ensuring proper form throughout.
It’s essential to address imbalances and weaknesses that may compromise scapular stabilization. For individuals with dominant upper trapezius activity, which often leads to elevated shoulders, incorporating lower trapezius isolation exercises like the prone Y-T-W series can be beneficial. Perform each lettered exercise for 10–12 repetitions, focusing on scapular retraction and depression. Additionally, soft tissue work, such as foam rolling the thoracic spine and chest, can improve mobility and allow for better scapular movement.
In conclusion, scapular stabilization is not merely a supporting act during arm abduction but a fundamental component of its execution. By understanding the interplay between the scapula and prime movers like the supraspinatus, individuals can optimize movement efficiency, reduce injury risk, and enhance overall upper body function. Incorporating specific exercises and addressing imbalances ensures that the scapula remains a stable foundation, enabling seamless and controlled arm abduction.
Explore related products






![]()
Range of Motion in Abduction
The prime mover of arm abduction, the supraspinatus muscle, initiates the movement but doesn’t act alone. Understanding the range of motion (ROM) in abduction reveals a complex interplay of muscles, joints, and biomechanics. Normal shoulder abduction spans approximately 180 degrees, from the side of the body to full overhead elevation. However, this range varies based on factors like age, flexibility, and joint health. For instance, athletes or individuals with consistent shoulder training may achieve greater ROM, while sedentary individuals or those with injuries often experience limitations.
Analyzing the mechanics, abduction occurs in three phases: initial lift (0°–30°), mid-range (30°–90°), and late phase (90°–180°). The supraspinatus dominates the initial phase, lifting the arm from rest. As the arm rises further, the deltoid muscle takes over, particularly its middle fibers, to sustain the movement. Beyond 90 degrees, the serratus anterior and upper fibers of the trapezius assist in stabilizing the scapula, allowing the arm to reach full overhead position. This phased muscle recruitment highlights the importance of balanced strength across the shoulder complex for optimal ROM.
To enhance abduction ROM, targeted exercises are key. External rotation exercises, such as band pull-aparts, strengthen the rotator cuff and improve stability. Scapular stabilization drills, like wall slides, ensure proper shoulder blade movement during abduction. For flexibility, doorway stretches or cross-body arm pulls can alleviate tightness in the posterior capsule, a common restriction in overhead motion. Incorporating these exercises 3–4 times weekly, with 10–15 repetitions per set, can yield noticeable improvements within 4–6 weeks.
A comparative perspective reveals that ROM in abduction is not just about muscle strength but also joint integrity. The glenohumeral joint’s shallow socket allows extensive mobility but sacrifices stability, making it prone to impingement or dislocation if ROM exceeds safe limits. Conversely, the scapulothoracic joint’s role in upward rotation during abduction underscores the importance of addressing both joints in training. For example, individuals with tight pec minor muscles often experience restricted scapular movement, indirectly limiting abduction ROM.
Practically, assessing and modifying ROM is essential for injury prevention. Active ROM tests, where the individual lifts their arm unassisted, reveal functional strength and flexibility. Passive ROM tests, where a therapist moves the arm, isolate joint restrictions. For older adults or post-injury populations, starting with gentle pendulum exercises or assisted stretches can gradually restore mobility without strain. Always avoid forceful stretching or lifting weights beyond 70% of one’s capacity during recovery phases to prevent setbacks.
In conclusion, mastering abduction ROM requires a holistic approach—strengthening key muscles, improving flexibility, and respecting joint mechanics. By understanding the phases of movement and implementing targeted strategies, individuals can achieve and maintain full, pain-free shoulder function. Whether for daily activities or athletic performance, optimizing abduction ROM is a cornerstone of upper body health.
Explore related products





![]()
Injury Risks and Prevention Tips
The prime mover of arm abduction is the supraspinatus muscle, a key component of the rotator cuff. While this muscle is essential for lifting the arm away from the body, its relatively small size and high demand make it susceptible to injury, particularly in athletes and individuals performing repetitive overhead activities. Understanding the risks and implementing preventive measures can significantly reduce the likelihood of strains, tears, or chronic conditions like impingement syndrome.
Analyzing the Risks:
Overuse is the primary culprit behind supraspinatus injuries. Activities such as swimming, tennis, weightlifting, or even painting ceilings place repeated stress on this muscle, leading to microtears and inflammation. Age also plays a role, as the muscle’s blood supply diminishes over time, impairing its ability to heal. Poor posture, especially rounded shoulders, further compromises the muscle’s function by altering shoulder mechanics. Ignoring early warning signs, like dull aches during overhead movements or weakness in abduction, can escalate the issue into a full-thickness tear requiring surgical intervention.
Preventive Strategies:
To safeguard the supraspinatus, incorporate targeted strengthening exercises into your routine. External rotation exercises with resistance bands (2–3 sets of 12–15 reps, 2–3 times weekly) improve muscle stability. Scapular stabilization drills, such as wall slides or prone Y-T-Ws, enhance shoulder blade control, reducing undue stress on the rotator cuff. For athletes, limit overhead training volume to 60–70% of total shoulder workload and include rest days to allow tissue recovery. Adults over 40 should prioritize flexibility; a daily door-frame stretch for the chest and anterior shoulders can counteract postural imbalances.
Practical Tips for Daily Life:
Ergonomics matter. When working at a desk, ensure your monitor is at eye level to avoid slouching. For manual tasks, alternate arms every 15 minutes to distribute load evenly. If lifting objects overhead, keep elbows slightly bent and engage the core to minimize strain. Apply ice for 15–20 minutes post-activity if you experience soreness, but avoid anti-inflammatory medications long-term, as they may delay tissue repair. Lastly, listen to your body—persistent pain warrants a consultation with a physical therapist to assess biomechanical issues.
Comparative Perspective:
Unlike larger muscles like the deltoid, the supraspinatus lacks redundancy in function, making it irreplaceable for abduction. While deltoid strains often resolve with rest, supraspinatus injuries can lead to chronic dysfunction if untreated. Prevention here is not just about strength but also about movement quality. For instance, a study in *Journal of Orthopaedic & Sports Physical Therapy* found that athletes with better scapular control had a 60% lower risk of rotator cuff injuries. This highlights the importance of holistic training over isolated muscle focus.
Protecting the supraspinatus requires a blend of awareness, targeted exercise, and lifestyle adjustments. By addressing risk factors proactively—whether through posture correction, balanced training, or ergonomic modifications—individuals can maintain shoulder health and sustain their active lifestyles. Remember, prevention is not just about avoiding injury; it’s about optimizing performance and longevity in every movement.
Frequently asked questions
The prime mover of arm abduction is the deltoid muscle, specifically its middle (lateral) fibers.
The supraspinatus muscle initiates arm abduction and assists the deltoid, but it is not the prime mover; it primarily stabilizes the shoulder joint.
Arm abduction is significantly impaired without the deltoid, as it is the primary muscle responsible for this movement, though other muscles like the supraspinatus and trapezius may assist.
The deltoid's middle fibers contract to lift the arm away from the body, making it the prime mover for abduction in the frontal plane.
Yes, the supraspinatus, trapezius, and serratus anterior assist in arm abduction, but the deltoid remains the primary muscle driving the movement.



























