The control of neck, shoulder, and upper arm muscles is primarily governed by the corticospinal tract, a major neural pathway originating in the motor cortex of the brain. This tract descends through the brainstem and spinal cord, transmitting signals that enable precise voluntary movements of these regions. Additionally, the lateral corticospinal tract plays a crucial role in fine motor control, while the ventral corticospinal tract contributes to more proximal muscle movements, including those in the shoulders and upper arms. These pathways work in conjunction with upper motor neurons and lower motor neurons to ensure coordinated and efficient muscle function in the neck and upper extremities.
Explore related products






What You'll Learn
- Cervical Spinal Cord Segments: C5-C6 control shoulder and arm muscles, enabling movement and stability
- Phrenic Nerve Function: Originates from C3-C5, innervates diaphragm, indirectly supports neck posture
- Brachial Plexus Role: Network of nerves from C5-T1, supplies upper limb muscles
- Accessory Nerve (CN XI): Innervates trapezius and sternocleidomastoid, crucial for neck and shoulder movement
- Muscular Coordination: Precise nerve signaling ensures synchronized neck, shoulder, and arm muscle function
![]()
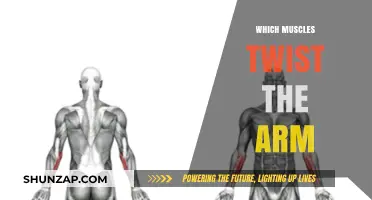
Cervical Spinal Cord Segments: C5-C6 control shoulder and arm muscles, enabling movement and stability
The cervical spinal cord segments, specifically C5 and C6, play a pivotal role in controlling the muscles of the shoulder and upper arm. These segments are responsible for transmitting nerve signals that enable both movement and stability, ensuring we can perform tasks ranging from lifting a cup to throwing a ball. Understanding their function is crucial for anyone dealing with neck or upper limb issues, as damage to these segments can result in significant motor and sensory deficits.
Analytically, the C5 and C6 segments are part of a complex network that connects the brain to the peripheral nervous system. The C5 segment primarily innervates the deltoid muscle, which is essential for shoulder abduction, and the biceps muscle, crucial for elbow flexion. Meanwhile, the C6 segment controls the wrist extensors and the muscles responsible for forearm rotation. Together, these segments ensure coordinated movement and strength in the upper limbs. For instance, a C5 injury might result in difficulty lifting the arm away from the body, while a C6 injury could impair the ability to straighten the wrist.
Instructively, maintaining the health of these spinal segments is vital for preserving upper limb function. Regular neck stretches, such as gently tilting the head from side to side, can help alleviate tension around the cervical spine. Strengthening exercises, like shoulder presses or bicep curls with light weights, can also support the muscles innervated by C5 and C6. For individuals over 40, incorporating low-impact activities like swimming or yoga can reduce strain on the cervical spine while promoting flexibility and strength.
Persuasively, recognizing the early signs of C5 or C6 dysfunction can prevent long-term complications. Symptoms like persistent shoulder pain, weakness in the arms, or difficulty gripping objects should not be ignored. Seeking prompt medical evaluation, including imaging studies like MRI or nerve conduction tests, can identify issues before they worsen. Early intervention, such as physical therapy or targeted exercises, can significantly improve outcomes and restore function.
Comparatively, while the lumbar spine is often associated with lower back pain, the cervical spine’s role in upper limb function is equally critical. Unlike lumbar segments, which primarily control leg movement, C5 and C6 directly influence fine motor skills and strength in the arms. This distinction highlights the need for tailored care when addressing cervical spine issues, as the impact on daily activities can be more immediate and debilitating.
In conclusion, the C5 and C6 cervical spinal cord segments are indispensable for shoulder and upper arm function. By understanding their role, adopting preventive measures, and addressing symptoms early, individuals can safeguard their ability to perform essential tasks with ease. Whether through targeted exercises, lifestyle adjustments, or medical intervention, prioritizing cervical spine health is key to maintaining mobility and independence.
Arm Adductor Muscles: Functions, Exercises, and Strengthening Techniques
You may want to see also
Explore related products






![]()
Phrenic Nerve Function: Originates from C3-C5, innervates diaphragm, indirectly supports neck posture
The phrenic nerve, emerging from the cervical spine at levels C3-C5, plays a pivotal role in respiratory function by innervating the diaphragm, the primary muscle of inhalation. This nerve’s pathway is critical for understanding its indirect influence on neck posture and stability. While its primary function is respiratory, the phrenic nerve’s origin in the upper cervical region ties it to the broader network of nerves controlling neck and shoulder muscles. For instance, damage to C3-C5, such as from trauma or surgical intervention, can disrupt both diaphragmatic function and neck muscle coordination, highlighting the interconnectedness of these systems.
Analyzing the phrenic nerve’s role reveals its dual significance in clinical settings. Patients with phrenic nerve palsy often experience not only respiratory distress but also altered neck posture due to compensatory muscle strain. This occurs because the diaphragm’s reduced efficiency forces accessory muscles of respiration, such as the scalene and sternocleidomastoid muscles, to work harder, indirectly affecting neck alignment. Physical therapists addressing respiratory issues must therefore consider neck posture in their treatment plans, emphasizing exercises that strengthen both diaphragmatic and cervical musculature.
From a practical standpoint, individuals with chronic neck pain or postural issues should be evaluated for underlying respiratory mechanics. Simple breathing exercises, such as diaphragmatic breathing (inhaling deeply through the nose while expanding the abdomen), can improve phrenic nerve function and reduce strain on neck muscles. For older adults or those with respiratory conditions like COPD, incorporating 10–15 minutes of diaphragmatic breathing daily can enhance both respiratory efficiency and neck stability. Caution should be taken, however, to avoid overexertion, as excessive strain on the diaphragm can exacerbate neck discomfort.
Comparatively, the phrenic nerve’s function contrasts with that of the brachial plexus, which directly innervates shoulder and upper arm muscles. While the brachial plexus originates from C5-T1 and focuses on limb movement, the phrenic nerve’s C3-C5 origin links it to both respiratory and postural systems. This distinction underscores the importance of targeted assessments: a patient with shoulder weakness may have brachial plexus involvement, whereas one with both respiratory difficulty and neck pain may have phrenic nerve dysfunction. Understanding these differences allows for more precise diagnosis and treatment.
In conclusion, the phrenic nerve’s role extends beyond respiration, subtly influencing neck posture through its cervical origin and interaction with accessory muscles. By recognizing this connection, healthcare providers and individuals can adopt holistic approaches to managing neck and respiratory health. Whether through breathing exercises, posture correction, or targeted therapy, addressing phrenic nerve function offers a unique pathway to alleviating neck discomfort and improving overall musculoskeletal balance.
Understanding the Muscle Injury That Immobilizes Your Arm: Causes and Recovery
You may want to see also
Explore related products





![]()
Brachial Plexus Role: Network of nerves from C5-T1, supplies upper limb muscles
The brachial plexus, a complex network of nerves originating from the spinal cord's cervical (C5-C8) and first thoracic (T1) roots, is the unsung hero of upper limb functionality. This intricate web of nerves is responsible for transmitting signals that control the muscles in the neck, shoulder, and upper arm, enabling a wide range of movements, from delicate finger dexterity to powerful arm lifts.
Anatomy and Functionality
Imagine the brachial plexus as a highway system, where each nerve root merges to form major "roads" (trunks, divisions, cords) that eventually branch into smaller "streets" (peripheral nerves). These nerves supply specific muscles: the musculocutaneous nerve powers elbow flexion (e.g., biceps), the radial nerve controls elbow extension and wrist/finger movement, and the axillary nerve activates shoulder abduction. For instance, lifting a cup to your mouth involves coordinated signals from C5-C7 roots via the brachial plexus to engage deltoid and biceps muscles.
Clinical Relevance and Injury Risks
Damage to the brachial plexus, often from trauma (e.g., car accidents, sports injuries), can result in severe functional deficits. Erb’s palsy, affecting C5-C6 roots, leads to a characteristic "waiter’s tip" arm posture due to shoulder and elbow weakness. Klumpke’s palsy, involving T1 and occasionally C8, causes hand and wrist paralysis. Immediate diagnosis via MRI or nerve conduction studies is critical, followed by physical therapy or surgical repair within 6-12 months for optimal recovery.
Practical Tips for Prevention and Care
To safeguard the brachial plexus, avoid prolonged neck extension or compression, common in activities like weightlifting or sleeping with arms overhead. Athletes should incorporate shoulder-strengthening exercises (e.g., rotator cuff workouts) and use protective gear. For those recovering from injury, gentle range-of-motion exercises (e.g., pendulum swings for the shoulder) and nerve-gliding techniques can aid rehabilitation. Always consult a neurologist or physical therapist for personalized guidance.
Comparative Insight: Brachial Plexus vs. Other Nerve Networks
Unlike the lumbar plexus, which serves the lower limbs, the brachial plexus is uniquely adapted for fine motor control and strength in the upper limbs. Its higher spinal root origins (C5-T1) reflect the evolutionary priority of hand and arm dexterity. While both plexuses share a similar developmental structure, the brachial plexus’s role in tasks requiring precision—typing, throwing, or playing an instrument—highlights its indispensable contribution to daily life.
Effective Lower Arm Muscle Building: Tips for Strength and Definition
You may want to see also
Explore related products






![]()
Accessory Nerve (CN XI): Innervates trapezius and sternocleidomastoid, crucial for neck and shoulder movement
The accessory nerve, or Cranial Nerve XI, plays a pivotal role in our ability to move and stabilize the neck and shoulders. Unlike other cranial nerves that originate solely in the brain, CN XI has a dual origin: its cranial root emerges from the medulla, while its spinal root arises from the upper cervical spinal cord. This unique anatomy underscores its importance in bridging central and peripheral nervous system functions. Specifically, CN XI innervates two critical muscles: the trapezius and the sternocleidomastoid. The trapezius, a large, flat muscle spanning the upper back, shoulders, and neck, is responsible for movements like shrugging, rotating the shoulder blades, and stabilizing the scapula. The sternocleidomastoid, a paired muscle running from the sternum and clavicle to the mastoid process of the skull, enables head rotation and flexion. Without CN XI, these fundamental actions would be severely compromised.
To understand the practical implications of CN XI dysfunction, consider a scenario where this nerve is damaged, such as from trauma or surgical injury. Patients may experience weakness or paralysis in the trapezius, leading to a visibly drooping shoulder and difficulty lifting the arm above the head. Similarly, sternocleidomastoid impairment can result in reduced head control, particularly when turning the neck. Clinicians often assess CN XI function through specific tests: for the trapezius, the patient is asked to shrug their shoulders against resistance, while sternocleidomastoid function is evaluated by observing head rotation strength. Early detection of deficits is crucial, as physical therapy and targeted exercises can help restore some function, though recovery depends on the extent and location of the injury.
From a comparative perspective, CN XI’s role in neck and shoulder movement contrasts with other nerves involved in upper limb control, such as the brachial plexus, which innervates muscles of the arm and hand. While the brachial plexus is essential for fine motor skills and arm mobility, CN XI focuses on proximal stability and gross movements of the neck and shoulder girdle. This distinction highlights the body’s intricate division of labor among neural structures. For instance, a baseball pitcher relies on both CN XI for shoulder stability during the windup and the brachial plexus for precise ball release. Understanding these complementary functions is key for athletes, physical therapists, and anyone seeking to optimize upper body performance.
For those interested in preventive care or rehabilitation, strengthening the trapezius and sternocleidomastoid muscles can enhance CN XI’s effectiveness. Simple exercises like shoulder shrugs with light weights or resistance bands, and head-turning movements against gentle pressure, can improve muscle tone and nerve responsiveness. However, caution is advised: overexertion or improper form can lead to strain or injury. Incorporating these exercises into a balanced routine, especially for individuals with sedentary lifestyles or post-injury recovery, can mitigate the risk of CN XI-related deficits. Ultimately, CN XI’s role in neck and shoulder movement underscores the delicate interplay between nerves and muscles, emphasizing the need for both awareness and proactive care.
Tone and Trim: Effective Strategies to Reduce Underarm Muscles
You may want to see also
Explore related products



$20



![]()
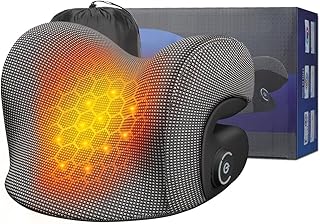
Muscular Coordination: Precise nerve signaling ensures synchronized neck, shoulder, and arm muscle function
The corticospinal tract, a major pathway in the central nervous system, plays a pivotal role in controlling the neck, shoulder, and upper arm muscles. This tract originates in the motor cortex of the brain and descends through the spinal cord, directly innervating motor neurons that govern voluntary movements. When you lift a cup to your mouth or reach for an object, the corticospinal tract ensures that the muscles in your neck, shoulder, and arm contract in a precise, synchronized manner. Without this coordination, even simple tasks would become cumbersome or impossible.
Consider the complexity of throwing a ball. This action requires seamless integration of multiple muscle groups: the neck stabilizes the head, the shoulder abducts and rotates, and the arm flexes and extends. Precise nerve signaling from the corticospinal tract ensures that each muscle fires at the correct time and with the appropriate force. For instance, a delay in shoulder muscle activation could result in a weak throw, while overactivation of neck muscles might cause unnecessary tension. This synchronization is achieved through the tract’s ability to modulate motor neuron activity, ensuring fluid, purposeful movement.
To optimize muscular coordination in these areas, targeted exercises can enhance nerve signaling efficiency. For adults aged 18–65, incorporating resistance training for the neck, shoulders, and arms twice weekly can improve neuromuscular control. Exercises like shoulder presses, lateral raises, and neck isometrics strengthen the muscles while refining the neural pathways that govern them. Caution: avoid overloading, as excessive strain can impair nerve function. Start with light weights (e.g., 2–5 lbs for neck exercises) and gradually increase resistance.
A comparative analysis highlights the difference between untrained and trained individuals. In untrained individuals, nerve signaling to these muscles may be less precise, leading to jerky or uncoordinated movements. Trained individuals, however, exhibit smoother, more efficient muscle activation due to strengthened neural pathways. For example, a study in *Journal of Neurophysiology* found that athletes demonstrated faster nerve conduction velocities in the corticospinal tract compared to non-athletes, correlating with better muscular coordination.
In practical terms, maintaining proper posture supports optimal nerve signaling. Poor posture compresses spinal nerves, disrupting signals to the neck, shoulder, and arm muscles. To counteract this, practice ergonomic alignment: keep shoulders back, chin parallel to the floor, and ears aligned with the shoulders. For desk workers, take a 5-minute break every hour to stretch and reset posture. This simple habit can significantly enhance nerve function and muscular coordination over time.
Transform Arm Flab to Muscle: Effective Workouts and Tips
You may want to see also
Frequently asked questions
The corticospinal tract (also known as the pyramidal tract) is primarily responsible for controlling voluntary movements of the neck, shoulder, and upper arm muscles. It originates in the motor cortex of the brain and sends signals through the spinal cord to innervate these muscles.
The corticospinal tract provides precise motor control by directly innervating alpha motor neurons in the spinal cord, which then activate muscles in the neck, shoulder, and upper arm. This allows for coordinated, voluntary movements like lifting, reaching, and turning the head.
While the corticospinal tract is the primary pathway, other tracts like the reticulospinal and rubrospinal tracts also contribute to motor control, particularly in posture, balance, and fine-tuning movements. However, the corticospinal tract remains the most critical for voluntary, precise actions.