Sepsis is a life-threatening condition that is mainly caused by bacterial infections and is characterized by a deregulated host response to infection, profound systemic inflammation, and disseminated intravascular coagulation, often leading to multiple organ failure and high mortality rates. Survivors of sepsis often experience long-term medical complications, including post-sepsis syndrome (PSS), which encompasses a range of physical and psychological issues such as chronic pain, fatigue, and symptoms of post-traumatic stress disorder (PTSD). One of the most prevalent and concerning complications of sepsis is muscle pain and weakness, formally known as sepsis-associated muscle wasting (SAMW) or sepsis-induced myopathy. This condition is characterized by decreased muscle mass, reduced muscle fiber size, and decreased muscle strength, resulting in persistent physical disability and poor health-related quality of life.
| Characteristics | Values |
|---|---|
| Mortality rate | 20-30% |
| Mortality rate after complications | 40-50% |
| Common causes | Bacterial infections |
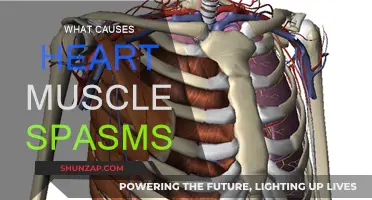
| Common symptoms | Muscle weakness, fatigue, hair loss, PTSD |
| Muscle weakness causes | Mitochondrial abnormalities, decreased muscle membrane excitability, sarcolemmal injury, atrophy, altered bioenergetics, decreased muscle mass, reduced muscle fibre size, decreased muscle strength, decreased titin gene expression, altered myofibre integrity |
| Muscle weakness prevention | Pharmacological protection of mitochondria, electrical muscular stimulation, physiotherapy, early mobilization, nutritional support, improving muscle quality |
Explore related products






What You'll Learn
![]()
Sepsis causes muscle weakness
Sepsis is a life-threatening condition caused by a deregulated host response to infection. It is mainly caused by bacterial infections and is the leading cause of inpatient hospitalizations. It is characterized by profound systemic inflammation and disseminated intravascular coagulation, which often lead to multiple organ failure and a high mortality rate.
Sepsis survivors often suffer from long-term medical complications, one of the most common being chronic skeletal muscle weakness. This muscle weakness can affect both peripheral nerves and skeletal muscles, resulting in a reduced capacity for physical activity and a poor health-related quality of life. It is characterized by decreased muscle mass, reduced muscle fiber size, and decreased muscle strength.
There are several factors that contribute to sepsis-induced muscle weakness. One factor is the development of acquired weakness syndromes, which affect both the respiratory muscles and the limb muscles. These syndromes can result in prolonged mechanical ventilation, functional impairment, and exercise limitation. Additionally, sepsis induces derangements at multiple subcellular sites involved in excitation-contraction coupling, such as decreased membrane excitability, sarcolemmal membrane injury, altered calcium homeostasis, and disrupted contractile protein interactions.
Another factor contributing to muscle weakness in sepsis survivors is mitochondrial dysfunction. Studies have shown that mitochondrial abnormalities are present in the skeletal muscle of sepsis survivors, and these abnormalities are believed to play a causal role in chronic post-sepsis muscle weakness. Pharmacological protection of mitochondria during acute sepsis has been proposed as a potential clinical treatment strategy to prevent post-sepsis muscle weakness.
Furthermore, muscle wasting is commonly observed in sepsis patients, which contributes to muscle weakness. This muscle wasting is characterized by profound muscle wasting and reduced muscle fiber size, which can be diagnosed through muscle biopsy or imaging techniques such as CT and MRI scans. Electrical muscular stimulation, physiotherapy, early mobilization, and nutritional support are currently used to prevent or treat sepsis-associated muscle wasting. However, there are still no pharmacological treatments available, and the underlying mechanisms are not yet fully understood.
Posture and Intercostal Pain: Is There a Link?
You may want to see also
Explore related products






![]()
Sepsis-associated muscle wasting
Sepsis is a life-threatening condition caused by a deregulated host response to infection. It is mainly caused by bacterial infections and is the leading cause of inpatient hospitalizations. It is characterized by profound systemic inflammation and disseminated intravascular coagulation, which often lead to multiple organ failure and subsequent mortality. The incidence of sepsis has risen by 9% to 13% annually, largely due to an expansion of the elderly population, more frequent invasive surgical procedures, and increased antibiotic resistance.
Sepsis survivors often suffer from long-term medical complications, particularly sepsis-associated muscle wasting (SAMW), which occurs in 40-70% of patients with sepsis. SAMW is characterized by decreased muscle mass, reduced muscle fibre size, and decreased muscle strength, resulting in persistent physical disability. Systemic inflammatory cytokines are the main cause of SAMW. The pathways associated with the ubiquitin-proteasome and autophagy systems are particularly activated in the muscle tissues during sepsis and may lead to muscle wasting. Expression of muscle atrophy-related genes Atrogin-1 and MuRF-1 are seemingly increased via the ubiquitin-proteasome pathway.
In clinical settings, electrical muscular stimulation, physiotherapy, early mobilization, and nutritional support are used to prevent or treat SAMW. However, there are currently no pharmacological treatments for SAMW, and the underlying mechanisms are still unknown. Muscle biopsy followed by histological evaluation is considered a highly accurate method to diagnose myopathic changes of SAMW. However, the biopsy method can be accompanied by some complications such as bleeding, pain, and nerve injury. A CT scan is widely accepted as the gold standard method for skeletal muscle mass quantification. MRI is also used for diagnoses of SAMW and has a highly accurate diagnostic value for muscle mass.
Post-sepsis muscle weakness is a serious medical issue, and survivors rarely return to baseline functional status after discharge from the ICU. Nearly half of previously functionally independent individuals require nursing care or home care after discharge. Nearly a third of patients with no prior comorbidities had problems with mobility one year after discharge. Survivors continue to develop functional limitations for at least 5 years following discharge, a trend that appears to be sepsis-specific. These patients are most vulnerable to economic repercussions since post-sepsis functional limitations often prevent them from returning to work.
Methotrexate and Muscle Spasms: What's the Link?
You may want to see also
Explore related products






![]()
Post-sepsis muscle weakness
Sepsis is a life-threatening condition that is mainly caused by bacterial infections and is characterized by a deregulated host response to infection, profound systemic inflammation, and disseminated intravascular coagulation. It often leads to multiple organ failure and subsequent mortality. Even after recovery, sepsis leaves patients with many long-term medical complications, including post-sepsis muscle weakness.
Sepsis-induced muscle weakness can affect both respiratory muscles and limb muscles, with diaphragm atrophy and dysfunction being a common complication in sepsis survivors. This can lead to prolonged mechanical ventilation and difficulty weaning off respiratory support. In addition to the diaphragm, skeletal muscles are also affected, with mitochondrial abnormalities present in the skeletal muscle of sepsis survivors.
The exact mechanisms contributing to long-term muscle dysfunction in sepsis survivors are not yet fully understood. Current animal models of sepsis have limitations, either causing early death or being too mild to trigger long-term chronic dysfunction. However, studies have shown that systemic inflammatory cytokines are the main cause of sepsis-associated muscle wasting, which occurs in 40-70% of patients with sepsis. Additionally, muscle biopsy evaluations and imaging techniques such as CT scans and MRIs have provided valuable insights into the myopathic changes and muscle wasting associated with sepsis.
Pharmacological protection of mitochondria during acute sepsis has been proposed as a potential clinical treatment strategy to prevent post-sepsis muscle weakness. Antioxidant therapies that improve muscle quality, rather than just increasing muscle quantity, may also be a promising avenue for future treatment.
Cataract Surgery: Can It Weaken Eye Muscles?
You may want to see also
![]()
Sepsis-induced myopathy
Sepsis is a life-threatening condition caused by a deregulated host response to infection, often bacterial. It is a leading cause of in-patient hospitalisations and mortality in intensive care units (ICUs). The incidence of sepsis has been rising, due to an expansion of the elderly population, more frequent invasive surgical procedures, and increased antibiotic resistance.
Sepsis survivors often suffer from long-term medical complications, including chronic skeletal muscle weakness, also known as Sepsis-induced Myopathy. This condition is characterised by decreased muscle mass, reduced muscle fibre size, and decreased muscle strength, resulting in persistent physical disability. In addition, survivors may experience disabling fatigue and chronic pain, as well as other symptoms such as hair loss and post-traumatic stress disorder (PTSD).
The exact mechanisms of Sepsis-induced Myopathy are not yet fully understood. However, studies have shown that systemic inflammatory cytokines are the main cause of muscle wasting in sepsis patients. Additionally, muscle biopsies have shown myopathic changes, such as atrophy (loss of muscle mass), reduced muscle force-generating capacity, and altered bioenergetics.
Recent studies have also investigated the role of mitochondrial abnormalities in Sepsis-induced Myopathy. These studies have found that mitochondrial dysfunction contributes to chronic muscle weakness after sepsis. Furthermore, pharmacological protection of mitochondria during acute sepsis may prevent the later development of muscle weakness, suggesting a potential clinical treatment strategy.
Furthermore, prolonged sepsis has been shown to cause neural and muscular abnormalities, including axonal swelling, axonal degeneration, and neuromuscular junction denervation. These abnormalities contribute to the muscle weakness experienced by sepsis survivors, impacting their quality of life and ability to return to work.
Nutrient Deficiency: A Risk Factor for Muscle Tears?
You may want to see also
![]()
ICU-acquired weakness
Sepsis is a major cause of morbidity and mortality in critically ill patients. Survivors of sepsis often experience long-term medical complications, including skeletal muscle weakness. This muscle weakness is a result of sepsis-induced myopathy, which is characterised by a reduction in muscle force-generating capacity, atrophy (loss of muscle mass), and altered bioenergetics.
The pathophysiology of ICU-AW is not yet fully understood, but it is believed to involve complex structural and functional alterations within myofibers and neurons. Risk factors for developing ICU-AW include age, weight, comorbidities, illness severity, organ failure, exposure to certain drugs, immobility, and other intensive care-related factors. ICU-AW increases the risk of mortality, both during and after hospitalisation, and prolongs the duration of mechanical ventilation, hospital stay, and rehabilitation.
Recent studies have suggested that mitochondrial abnormalities may play a key role in the development of post-sepsis skeletal muscle weakness. In experiments using transgenic mice, it was found that overexpression of the MnSOD gene protected against mitochondrial abnormalities and subsequent muscle weakness following sepsis. This provides potential therapeutic targets for preventing and treating post-sepsis muscle weakness.
Early rehabilitation, including physiotherapy and exercise regimens, has been shown to reduce the likelihood of developing ICU-AW and improve patient outcomes. However, more research is needed to fully understand the pathogenesis of ICU-AW and develop effective treatment strategies.
Caffeine Overload: Facial Muscle Spasms Explained
You may want to see also
Frequently asked questions
Sepsis causes muscle pain due to muscle wasting, which is characterised by decreased muscle mass, reduced muscle fibre size, and decreased muscle strength. This results in persistent physical disability.
Sepsis survivors often suffer from long-term medical complications, particularly chronic skeletal muscle weakness. This weakness can last for at least 5 years following hospital discharge.
The underlying causes of muscle pain in sepsis patients are still being studied. However, it is known that systemic inflammatory cytokines are the main cause of sepsis-associated muscle wasting, which occurs in 40-70% of patients with sepsis.