Benzodiazepines are a class of medications primarily known for their anxiolytic, sedative, and hypnotic properties, but their role as muscle relaxants is a topic of interest and debate. While some benzodiazepines, such as diazepam, are commonly prescribed for their muscle-relaxing effects due to their ability to modulate GABA receptors and reduce central nervous system activity, not all benzodiazepines exhibit this property to the same extent. The muscle relaxant effects of benzodiazepines are often secondary to their primary actions and depend on factors such as dosage, specific drug characteristics, and individual patient response. Therefore, while certain benzodiazepines can effectively alleviate muscle spasms and tension, it is inaccurate to categorize all benzodiazepines as muscle relaxants, as their therapeutic profiles vary widely.
| Characteristics | Values |
|---|---|
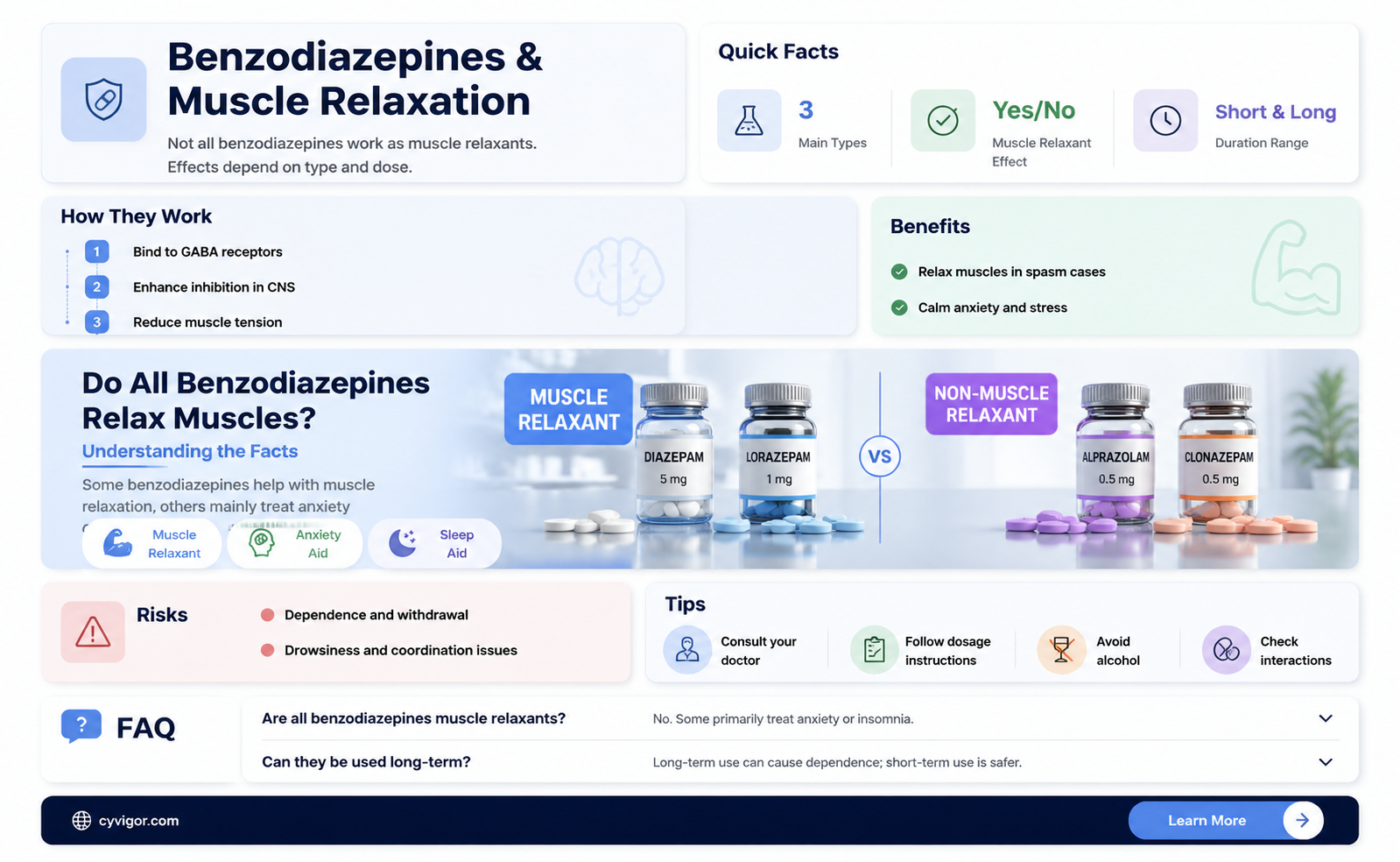
| Are all benzodiazepines muscle relaxants? | No, not all benzodiazepines are primarily muscle relaxants. While some have muscle relaxant properties, they are primarily used for their anxiolytic, sedative, hypnotic, and anticonvulsant effects. |
| Benzodiazepines with muscle relaxant properties | Diazepam, Lorazepam, Clonazepam, and Temazepam (to some extent). These drugs can reduce muscle tension and spasms due to their central nervous system depressant effects. |
| Mechanism of action | Benzodiazepines enhance the effect of the neurotransmitter gamma-aminobutyric acid (GABA) at the GABAA receptor, leading to increased inhibition of neuronal activity, which can result in muscle relaxation. |
| Primary uses | Anxiety disorders, insomnia, seizures, alcohol withdrawal, and as premedication for medical procedures. Muscle relaxation is often a secondary effect. |
| Examples of benzodiazepines without significant muscle relaxant properties | Alprazolam (Xanax), Chlordiazepoxide (Librium), and Oxazepam. These are primarily used for anxiety and related conditions. |
| Side effects related to muscle relaxation | Drowsiness, dizziness, and impaired coordination, which can be more pronounced in drugs with stronger muscle relaxant effects. |
| Clinical considerations | Muscle relaxant effects are dose-dependent and vary among individuals. Benzodiazepines are generally not first-line treatments for muscle spasms or pain; other muscle relaxants (e.g., baclofen, tizanidine) are preferred for such conditions. |
| Dependency and withdrawal | Long-term use of benzodiazepines, including those with muscle relaxant properties, can lead to physical dependence and withdrawal symptoms, including rebound anxiety and muscle tension. |
Explore related products






What You'll Learn
- Benzodiazepine Classification: Not all benzodiazepines are primarily muscle relaxants; they have varied therapeutic uses
- Muscle Relaxant Mechanism: Some benzodiazepines act on GABA receptors to reduce muscle tension indirectly
- Specific Benzodiazepines: Diazepam and clonazepam are known for muscle relaxant properties, others are not
- Primary Uses: Most benzodiazepines are prescribed for anxiety, insomnia, or seizures, not muscle relaxation
- Side Effects: Muscle relaxation is often a secondary effect, not the primary purpose of benzodiazepines
![]()
Benzodiazepine Classification: Not all benzodiazepines are primarily muscle relaxants; they have varied therapeutic uses
Benzodiazepines, a class of psychoactive drugs, are often associated with muscle relaxation due to their ability to enhance the effect of the neurotransmitter GABA, which has a calming effect on the central nervous system. However, this is just one aspect of their diverse therapeutic profile. While some benzodiazepines like diazepam (Valium) and lorazepam (Ativan) do exhibit pronounced muscle relaxant properties, others are primarily used for different indications. For instance, alprazolam (Xanax) is widely prescribed for anxiety disorders, and temazepam (Restoril) is specifically indicated for insomnia. This variation in use underscores the importance of understanding the unique pharmacological properties of each benzodiazepine.
To illustrate, consider the dosage and administration differences. Muscle relaxants like diazepam are often prescribed in doses ranging from 2 to 10 mg, taken 2 to 4 times daily, depending on the severity of muscle spasms. In contrast, alprazolam for anxiety is typically started at 0.25 to 0.5 mg, administered 3 times daily, with dosages adjusted based on patient response and tolerance. This highlights how the same class of drugs can be tailored to address distinct medical needs. It’s crucial for healthcare providers to match the benzodiazepine to the specific condition, considering factors like age, comorbidities, and potential drug interactions.
From a comparative perspective, benzodiazepines like clonazepam (Klonopin) are particularly effective for seizure disorders, while others like midazolam (Versed) are used for sedation in medical procedures. This diversity in application is rooted in their varying half-lives and affinities for GABA receptors. For example, clonazepam has a long half-life of 30 to 40 hours, making it suitable for sustained anticonvulsant effects, whereas midazolam’s short half-life of 1.5 to 2.5 hours is ideal for short-term sedation. Patients and clinicians must be aware of these differences to optimize treatment outcomes and minimize side effects, such as drowsiness or dependence.
A persuasive argument for the nuanced use of benzodiazepines lies in their potential risks and benefits. While muscle relaxants can provide immediate relief for conditions like acute back pain, their use should be limited to short durations (2 to 4 weeks) to avoid tolerance and withdrawal symptoms. Similarly, benzodiazepines for anxiety or insomnia should be prescribed judiciously, especially in older adults, who are more susceptible to cognitive impairment and falls. Practical tips include starting with the lowest effective dose, regularly reassessing the need for continued treatment, and exploring non-pharmacological alternatives like physical therapy or cognitive-behavioral therapy.
In conclusion, benzodiazepines are a versatile class of drugs with applications extending far beyond muscle relaxation. Their classification and use depend on specific pharmacological properties, patient needs, and clinical context. By understanding these distinctions, healthcare providers can prescribe benzodiazepines more effectively, ensuring that patients receive the right drug for their condition while minimizing risks. This tailored approach is essential for maximizing therapeutic benefits and improving patient outcomes.
Colchicine's Muscle Relaxation Effects: Unraveling Its Role in Pain Relief
You may want to see also
Explore related products






![]()
Muscle Relaxant Mechanism: Some benzodiazepines act on GABA receptors to reduce muscle tension indirectly
Benzodiazepines, a class of medications primarily known for their anxiolytic and sedative effects, exhibit a fascinating mechanism when it comes to muscle relaxation. Not all benzodiazepines are created equal in this regard, and understanding their action on the GABA receptors is key to unraveling this mystery. The GABA (gamma-aminobutyric acid) system, a major inhibitory pathway in the central nervous system, plays a pivotal role in this process.
The GABA Connection: Benzodiazepines' muscle relaxant properties are indirectly linked to their interaction with GABA-A receptors. When these drugs bind to specific sites on the GABA-A receptor complex, they enhance the inhibitory effects of GABA, the brain's primary calming neurotransmitter. This modulation of GABAergic transmission results in a cascade of events, ultimately leading to reduced muscle tension. For instance, diazepam, a well-known benzodiazepine, increases the frequency of chloride channel opening, causing hyperpolarization and subsequent muscle relaxation.
A Comparative Perspective: Interestingly, not all benzodiazepines exhibit pronounced muscle relaxant effects. The variation lies in their affinity for different subtypes of GABA-A receptors. Drugs like diazepam and lorazepam, with a higher propensity for the α2 and α3 subunits, tend to have more significant muscle relaxant properties. In contrast, alprazolam, primarily acting on α1 subunits, is less associated with this effect. This distinction is crucial in clinical practice, as it allows healthcare professionals to tailor prescriptions based on the desired therapeutic outcome.
Practical Implications: In a clinical setting, the muscle relaxant effect of benzodiazepines is often utilized in conjunction with their anxiolytic properties. For patients experiencing muscle spasms or tension related to anxiety disorders, a benzodiazepine with pronounced muscle relaxant qualities can provide dual relief. However, it's essential to consider the potential for tolerance and dependence, especially with long-term use. Starting with lower doses, such as 2-5 mg of diazepam, and gradually adjusting based on patient response, can help mitigate these risks.
A Word of Caution: While the muscle relaxant mechanism of certain benzodiazepines is beneficial, it's not without potential drawbacks. The indirect nature of this effect means that muscle relaxation is a secondary outcome of GABA modulation. As such, it may not be as potent or targeted as direct-acting muscle relaxants. Additionally, the sedative effects of benzodiazepines can sometimes overshadow the desired muscle relaxation, particularly in elderly patients or those with respiratory conditions. Therefore, a comprehensive patient assessment is vital before prescribing these medications for muscle-related ailments.
In summary, the muscle relaxant mechanism of select benzodiazepines is a nuanced aspect of their pharmacological profile. By understanding their interaction with GABA receptors, healthcare providers can make informed decisions when considering these drugs for muscle tension relief. This knowledge ensures a more precise and effective approach to patient care, especially when managing conditions that require both anxiety reduction and muscle relaxation.
Do Muscle Relaxers Appear in Saliva Drug Tests? Find Out Here
You may want to see also
Explore related products






![]()
Specific Benzodiazepines: Diazepam and clonazepam are known for muscle relaxant properties, others are not
Benzodiazepines, a class of medications primarily used for their sedative, anxiolytic, and anticonvulsant properties, are not uniformly muscle relaxants. While some benzodiazepines exhibit notable muscle relaxant effects, others do not. Among the former, diazepam and clonazepam stand out for their well-documented ability to alleviate muscle spasms and tension. Diazepam, for instance, is commonly prescribed at doses of 2–10 mg, taken 2–4 times daily, to manage conditions like muscle spasticity or tetanus. Clonazepam, often dosed at 0.5–2 mg daily in divided doses, is particularly effective for muscle-related conditions associated with seizures or panic disorders. These specific benzodiazepines act by enhancing the inhibitory effects of GABA, a neurotransmitter that reduces neuronal excitability, thereby relaxing muscles.
In contrast, not all benzodiazepines share this muscle relaxant property. For example, alprazolam, primarily used for anxiety disorders, and lorazepam, often prescribed for insomnia or acute seizures, have minimal to no muscle relaxant effects. Their mechanisms are more focused on reducing anxiety and inducing sedation rather than directly targeting muscle tension. This distinction is crucial for clinicians and patients, as it influences the choice of medication based on the specific symptoms being treated. Misapplication of a benzodiazepine without muscle relaxant properties for a condition requiring such effects could lead to suboptimal outcomes.
The variability in muscle relaxant properties among benzodiazepines highlights the importance of precise prescribing. For patients with conditions like multiple sclerosis, cerebral palsy, or acute back spasms, diazepam or clonazepam may be the preferred choice. However, these medications are not without risks. Prolonged use can lead to dependence, tolerance, and withdrawal symptoms, particularly in doses exceeding 10 mg daily for diazepam or 4 mg daily for clonazepam. Patients, especially those over 65 or with hepatic impairment, should start at the lowest effective dose and be monitored closely for side effects such as drowsiness, dizziness, or impaired coordination.
Practical tips for optimizing the use of diazepam and clonazepam include avoiding alcohol and other CNS depressants, as these can exacerbate sedation and respiratory depression. Patients should also be advised not to abruptly discontinue these medications, as tapering under medical supervision is essential to prevent withdrawal seizures. For acute muscle spasms, diazepam may be administered intravenously in hospital settings at doses of 5–10 mg, repeated every 10–15 minutes as needed, up to a maximum of 30 mg. Clonazepam, due to its longer half-life, is typically reserved for chronic conditions and should not be used for rapid symptom relief.
In summary, while benzodiazepines like diazepam and clonazepam are effective muscle relaxants, others in the class are not. Understanding these differences is vital for targeted treatment, ensuring patients receive the most appropriate medication for their specific needs. Careful consideration of dosage, patient characteristics, and potential risks is essential to maximize therapeutic benefits while minimizing adverse effects. This tailored approach underscores the nuanced role of benzodiazepines in modern medicine.
Effective Techniques to Release Muscle Tension and Promote Relaxation
You may want to see also
Explore related products






![]()
Primary Uses: Most benzodiazepines are prescribed for anxiety, insomnia, or seizures, not muscle relaxation
Benzodiazepines, often recognized by names like Xanax, Valium, and Ativan, are primarily prescribed for conditions such as anxiety, insomnia, and seizures. While they can have muscle relaxant effects, this is not their primary therapeutic purpose. For instance, diazepam (Valium) is sometimes used for muscle spasms, but its FDA-approved indications focus on anxiety, alcohol withdrawal, and seizure control. This distinction is crucial for patients and healthcare providers to understand, as misuse or misprescription can lead to dependency or adverse effects.
Consider the dosage and administration guidelines for benzodiazepines. For anxiety, alprazolam (Xanax) is typically prescribed at 0.25–0.5 mg three times daily, while for insomnia, temazepam (Restoril) is often given as a single 15–30 mg dose at bedtime. These regimens are tailored to address the central nervous system’s response to stress or sleep disturbances, not to target muscle tension directly. Even when muscle relaxation occurs, it is a secondary effect, often mediated by the drug’s broader action on GABA receptors, which induce sedation and calmness.
From a comparative perspective, benzodiazepines differ from dedicated muscle relaxants like cyclobenzaprine or tizanidine, which are specifically formulated to alleviate musculoskeletal pain. For example, tizanidine is prescribed at 2–4 mg every 6–8 hours for muscle spasms, with a maximum daily dose of 36 mg. In contrast, benzodiazepines are rarely first-line treatments for muscle issues unless accompanied by anxiety or sleep disorders. This highlights their role as versatile but specialized medications, best used within their approved therapeutic ranges.
Practically, patients should be aware of the potential risks when benzodiazepines are used off-label for muscle relaxation. Prolonged use can lead to tolerance, dependence, and withdrawal symptoms, particularly in older adults or those with a history of substance abuse. For acute muscle pain, combining physical therapy, heat application, and short-term use of NSAIDs may be safer and more effective. Always consult a healthcare provider to determine the most appropriate treatment, ensuring benzodiazepines are reserved for their primary indications.
In summary, while benzodiazepines may offer muscle relaxant benefits, their primary uses remain centered on anxiety, insomnia, and seizures. Understanding this distinction ensures safer prescribing practices and better patient outcomes. By adhering to recommended dosages and avoiding off-label use, individuals can maximize the therapeutic benefits of these medications while minimizing risks.
Muscle Relaxers and Drug Tests: Timing for Accurate Results
You may want to see also
Explore related products






![]()
Side Effects: Muscle relaxation is often a secondary effect, not the primary purpose of benzodiazepines
Benzodiazepines, commonly prescribed for anxiety and insomnia, are not primarily muscle relaxants, despite their ability to induce muscle relaxation as a secondary effect. This distinction is crucial for both patients and healthcare providers to understand, as it influences how these medications are prescribed and used. For instance, while diazepam (Valium) is often associated with muscle relaxation, its primary mechanism is to enhance the effect of the neurotransmitter GABA, which calms the central nervous system. Muscle relaxation occurs as a downstream consequence of this calming effect, not as its main function.
Consider the dosage and context in which benzodiazepines are used. A low dose of lorazepam (Ativan), typically 0.5–1 mg for anxiety, may not produce noticeable muscle relaxation in most patients. However, higher doses, such as 2–5 mg, prescribed for preoperative sedation or alcohol withdrawal, can lead to pronounced muscle relaxation. This variability underscores that muscle relaxation is dose-dependent and secondary to the drug’s primary action. Patients should be aware that while muscle relaxation may occur, it is not the intended therapeutic goal unless specifically prescribed for conditions like muscle spasms or spasticity.
From a comparative perspective, benzodiazepines differ from dedicated muscle relaxants like cyclobenzaprine or tizanidine, which directly target skeletal muscle. Benzodiazepines’ muscle-relaxing effects are indirect, stemming from their sedative and anxiolytic properties. For example, a patient with chronic back pain might be prescribed tizanidine (Zanaflex) 2–4 mg at bedtime for direct muscle relief, whereas a benzodiazepine like clonazepam (Klonopin) 0.5–1 mg might be used to reduce anxiety-induced muscle tension. The choice depends on whether muscle relaxation is the primary goal or a beneficial side effect.
Practical tips for patients include monitoring how benzodiazepines affect their bodies. If muscle relaxation is a desired outcome, discuss this with a healthcare provider, who may adjust the dosage or consider a combination therapy. For older adults (over 65), caution is advised, as benzodiazepines can increase the risk of falls due to excessive muscle relaxation and sedation. Starting with the lowest effective dose (e.g., 0.25 mg of alprazolam for anxiety) and gradually titrating upward can help minimize unintended effects. Always avoid alcohol and other CNS depressants when taking benzodiazepines, as these can amplify muscle relaxation and sedation, increasing the risk of accidents.
In conclusion, while muscle relaxation is a common side effect of benzodiazepines, it is not their primary purpose. Understanding this distinction ensures these medications are used appropriately, maximizing benefits while minimizing risks. Patients and providers should focus on the intended therapeutic goal and adjust treatment plans accordingly, especially when muscle relaxation is either a desired outcome or a potential concern.
Muscle Relaxers and Digestion: Can They Cause Unexpected Bowel Movements?
You may want to see also
Frequently asked questions
No, not all benzodiazepines are primarily muscle relaxants. While some benzodiazepines, like diazepam, have muscle relaxant properties, others are primarily used for anxiety, insomnia, or seizures.
Benzodiazepines such as diazepam (Valium) and lorazepam (Ativan) are known to have muscle relaxant properties in addition to their other effects.
While some benzodiazepines can help with muscle relaxation, they are typically prescribed for conditions like anxiety, insomnia, or seizures. Their use as muscle relaxants is often secondary to their primary indications.
Yes, there are non-benzodiazepine muscle relaxants, such as cyclobenzaprine (Flexeril) and tizanidine (Zanaflex), which are specifically designed to treat muscle spasms and pain without the sedative effects of benzodiazepines.