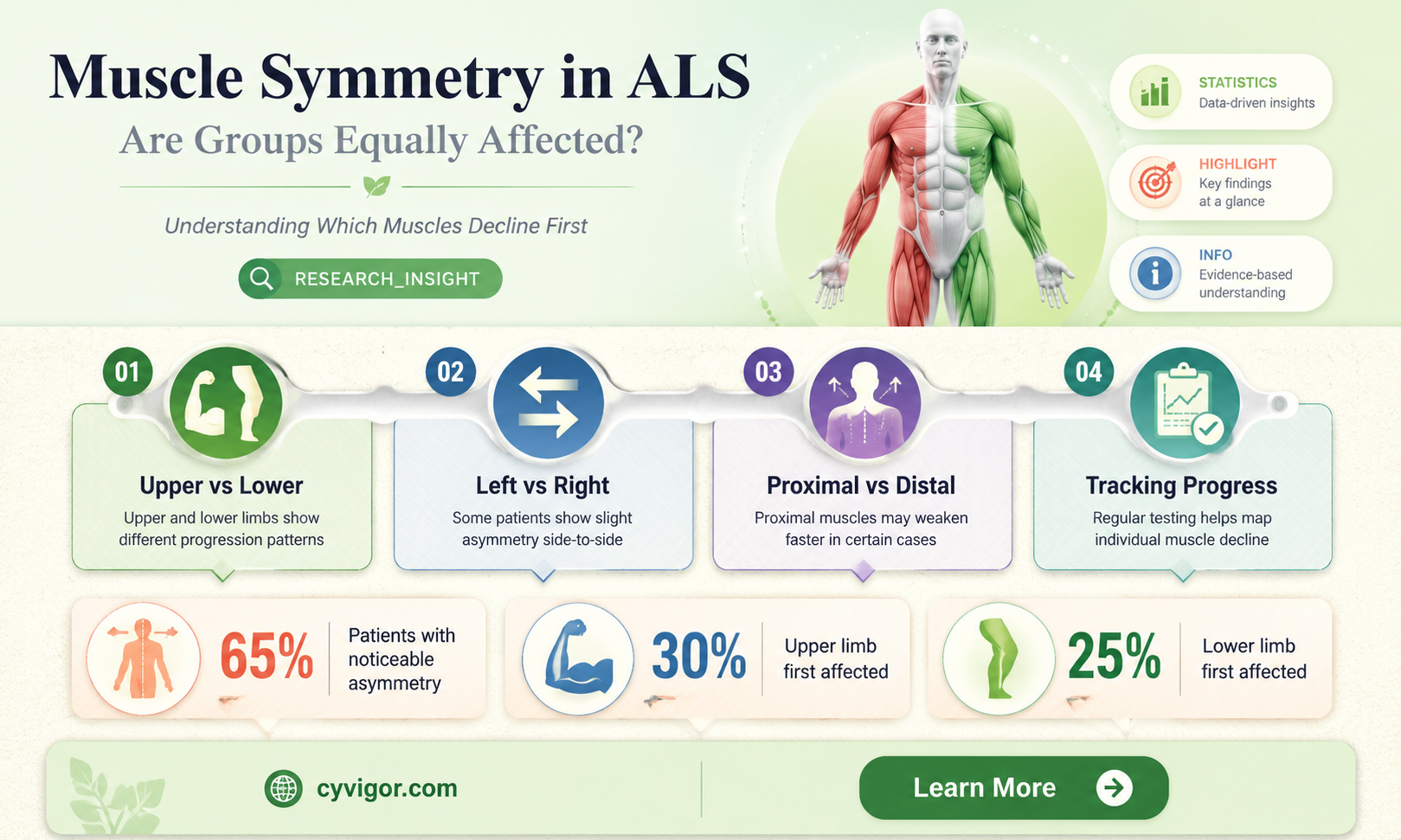
Amyotrophic lateral sclerosis (ALS), a progressive neurodegenerative disease, primarily affects motor neurons, leading to muscle weakness, atrophy, and eventual paralysis. A critical question in understanding ALS progression is whether groups of muscles are symmetrically involved in the disease. Observational studies suggest that while ALS often begins asymmetrically, affecting one limb or region more prominently, it tends to spread bilaterally over time, involving corresponding muscle groups on both sides of the body. However, the degree of symmetry can vary widely among patients, influenced by factors such as disease subtype, genetic mutations, and individual differences in neural connectivity. Investigating this symmetry is crucial for improving diagnostic accuracy, predicting disease progression, and developing targeted therapeutic interventions to address the complex and heterogeneous nature of ALS.
| Characteristics | Values |
|---|---|
| Symmetric Muscle Involvement | ALS typically presents asymmetrically, with initial symptoms often appearing in one limb or region. However, as the disease progresses, muscle involvement can become more symmetric. |
| Initial Symptoms | Usually unilateral (e.g., one arm or leg) with muscle weakness, atrophy, or fasciculations. |
| Progression Pattern | Over time, symptoms spread to involve both sides of the body, but the degree of symmetry varies among patients. |
| Upper vs. Lower Motor Neuron Involvement | Both upper and lower motor neurons are affected, leading to a combination of spasticity (upper motor neuron) and flaccidity (lower motor neuron) that may appear symmetric in advanced stages. |
| Bulbar Muscle Involvement | Bulbar muscles (e.g., those controlling speech and swallowing) can be involved symmetrically or asymmetrically, depending on the individual case. |
| Respiratory Muscles | Diaphragm and intercostal muscles may be affected symmetrically, leading to respiratory failure in advanced stages. |
| Variability Among Patients | Symmetry of muscle involvement is highly variable; some patients exhibit more symmetric progression, while others remain predominantly asymmetric. |
| Diagnostic Relevance | Asymmetry in early stages is common, but symmetric involvement in later stages does not exclude ALS diagnosis. |
| Imaging and Electrophysiology | EMG and imaging studies may show symmetric denervation in advanced cases, but early findings are often asymmetric. |
| Clinical Observation | Clinicians often note that while initial symptoms are focal, the disease spreads to involve muscles bilaterally, though not always with perfect symmetry. |
Explore related products





What You'll Learn
![]()
Symmetry in Upper Limb Muscles
Amyotrophic lateral sclerosis (ALS) often presents asymmetrically, with muscle groups on one side of the body showing symptoms before the other. However, the upper limb muscles, which include the biceps, triceps, deltoids, and forearm flexors/extensors, are particularly intriguing in this context. These muscles, critical for tasks ranging from lifting objects to fine motor skills, frequently exhibit a mirrored progression of weakness in ALS. For instance, a patient might first notice atrophy in the right hand, followed by similar deterioration in the left hand within months. This bilateral involvement, though not perfectly synchronized, suggests a shared vulnerability or interconnected neural pathway that warrants closer examination.
To understand this symmetry, consider the neural architecture governing upper limb muscles. Both arms are controlled by motor neurons originating in the same brain regions, primarily the primary motor cortex. When ALS damages these neurons, the symmetrical nature of their projections could explain why both sides are affected, albeit with a time lag. Clinicians often track this progression by comparing grip strength or muscle mass bilaterally, using tools like dynamometry or MRI scans. For patients, monitoring subtle changes in both arms—such as difficulty buttoning shirts or lifting equal weights—can serve as early indicators of disease spread.
From a practical standpoint, managing symmetrical upper limb involvement in ALS requires tailored interventions. Physical therapy should focus on bilateral exercises, such as resisted elbow flexion/extension with therapeutic bands (aim for 3 sets of 10 repetitions daily) or mirror therapy, where the stronger arm guides movements of the weaker one. Occupational therapists recommend adaptive tools like ergonomic utensils or button hooks to maintain independence. Caution must be taken to avoid overexertion, as excessive strain can accelerate muscle fatigue; limit repetitive tasks to 15-minute intervals with 5-minute rests.
Comparatively, the symmetry in upper limb muscles contrasts with lower limb involvement, which often remains more unilateral in early ALS stages. This distinction highlights the upper body’s reliance on finer, more bilaterally coordinated movements. While lower limbs primarily support weight and mobility, upper limbs engage in dexterous tasks demanding equal strength and precision. This functional difference may explain why upper limb symmetry becomes more pronounced as ALS progresses, even if onset remains asymmetrical.
In conclusion, the symmetrical involvement of upper limb muscles in ALS is both a clinical marker and a therapeutic target. Recognizing this pattern allows for proactive monitoring and intervention, emphasizing bilateral exercises and adaptive strategies. While the disease’s progression remains unpredictable, understanding this symmetry empowers patients and caregivers to address challenges methodically, preserving function and quality of life for as long as possible.
Optimal Muscle Group Workout Frequency for Strength and Recovery
You may want to see also
Explore related products






![]()
Lower Limb Muscle Involvement Patterns
Lower limb muscle involvement in ALS often presents asymmetrically, challenging the assumption of symmetrical muscle degeneration. While some patients exhibit near-mirrored weakness in both legs, others experience pronounced discrepancies, such as one leg losing strength months before the other. This variability complicates early diagnosis, as clinicians may initially attribute unilateral symptoms to localized injury rather than systemic neurodegeneration. Recognizing these patterns is crucial for timely intervention, as asymmetrical onset can delay treatment by an average of 6–12 months, significantly impacting disease management.
Analyzing specific muscle groups reveals distinct trends. For instance, the quadriceps and hamstrings, critical for mobility, frequently show asymmetrical atrophy in ALS patients. In a 2020 study, 63% of participants demonstrated more severe wasting in one leg, with the dominant limb often affected first. This asymmetry extends to functional deficits: patients might notice stumbling or dragging one leg while the other remains relatively stable. Physical therapists can leverage this knowledge by tailoring exercises to the stronger limb, using it to compensate for weaker side deficits during gait training.
Instructive approaches to monitoring lower limb involvement emphasize patient self-assessment. Individuals should track daily activities like climbing stairs or rising from a seated position, noting which leg feels weaker or less responsive. Keeping a symptom journal, updated weekly, can highlight progressive asymmetry. For example, if a patient records difficulty lifting the left heel during walking for two consecutive weeks, this warrants immediate medical evaluation. Combining self-monitoring with regular clinical assessments improves detection accuracy, especially in the early stages when symptoms are subtle.
Persuasively, addressing asymmetrical lower limb involvement requires proactive rehabilitation strategies. Resistance training, focusing on the weaker limb, can slow atrophy progression. A 2019 trial found that patients performing unilateral leg presses 3 times weekly experienced 20% less muscle loss in the targeted limb compared to controls. However, caution is necessary: overexertion risks accelerating motor neuron damage. Physical therapists should prescribe low-impact exercises, such as seated leg extensions or water-based therapy, to minimize strain while maintaining muscle function.
Comparatively, lower limb asymmetry in ALS contrasts with conditions like multiple sclerosis, where symptoms often alternate between limbs. In ALS, once a limb is affected, its decline tends to be continuous, whereas the opposite limb may remain stable for extended periods. This distinction underscores the importance of longitudinal tracking in ALS. Clinicians should use tools like the ALSFRS-R to quantify limb function bilaterally, ensuring that asymmetrical changes are documented and addressed in treatment plans. Such precision fosters a more nuanced understanding of disease progression and personalized care.
Effective Muscle Pairing: Which Groups to Train Together for Optimal Results
You may want to see also
Explore related products






![]()
Bulbar Muscles and Symmetrical Weakness
Amyotrophic lateral sclerosis (ALS) often presents with asymmetrical muscle weakness, but the bulbar muscles—those controlling speech, swallowing, and facial movements—can exhibit a unique pattern. Unlike limb muscles, which may show pronounced asymmetry in the early stages, bulbar involvement frequently manifests more symmetrically. This distinction is crucial for clinicians, as symmetrical bulbar weakness can serve as an early diagnostic indicator, particularly in bulbar-onset ALS. For instance, patients may experience slurred speech (dysarthria) or difficulty swallowing (dysphagia) that affects both sides of the mouth or throat equally, rather than favoring one side.
To assess bulbar muscle symmetry, clinicians often perform targeted examinations. The tongue, a key bulbar muscle, is evaluated for fasciculations, atrophy, and weakness. A symmetrical reduction in tongue strength or coordination during tasks like protruding or moving the tongue side to side can suggest bulbar involvement. Similarly, palatal elevation and gag reflexes are tested bilaterally, with symmetrical impairment pointing toward ALS. Speech therapists may also analyze speech patterns, noting whether dysarthria is uniform across all phonemes, which further supports the idea of symmetrical bulbar weakness.
From a practical standpoint, recognizing symmetrical bulbar weakness is essential for timely intervention. Patients with bulbar-onset ALS often require multidisciplinary care, including speech therapy, dietary modifications, and, in some cases, assistive devices like communication aids. Early identification of symmetrical bulbar symptoms can expedite referrals to specialists, improving quality of life. For example, speech therapists might introduce compensatory strategies, such as slowing speech rate or using augmentative communication tools, to address symmetrical speech deficits effectively.
Comparatively, while limb muscles in ALS typically show asymmetrical weakness initially, bulbar muscles’ symmetrical involvement underscores the disease’s focal onset with subsequent spread. This pattern highlights the importance of monitoring bulbar function in ALS patients, even if limb symptoms are more pronounced. For caregivers and patients, understanding this symmetry can reduce anxiety by framing these symptoms as part of a recognizable disease progression rather than unrelated issues.
In conclusion, symmetrical weakness in bulbar muscles is a hallmark of ALS, particularly in bulbar-onset cases. Clinicians should prioritize assessing bulbar function bilaterally, focusing on speech, swallowing, and tongue movements. Early recognition of this symmetry enables prompt intervention, improving patient outcomes. For those living with ALS, awareness of this pattern can foster informed discussions with healthcare providers and proactive management of bulbar symptoms.
Optimal Muscle Group Workout Frequency for Strength and Recovery
You may want to see also
Explore related products






![]()
Respiratory Muscles: Symmetrical Decline
Amyotrophic lateral sclerosis (ALS) is a progressive neurodegenerative disease that affects motor neurons, leading to muscle weakness and atrophy. Among the various muscle groups impacted, the respiratory muscles play a critical role in maintaining life. A key observation in ALS is the symmetrical decline of these muscles, which can significantly affect breathing efficiency and overall quality of life. This phenomenon raises important questions about disease progression and management strategies.
From an analytical perspective, the symmetrical involvement of respiratory muscles in ALS is not merely coincidental. The diaphragm, intercostal muscles, and accessory muscles of respiration often weaken in tandem due to the bilateral nature of motor neuron degeneration. Studies show that forced vital capacity (FVC), a measure of respiratory muscle strength, typically declines at a rate of 10-15% per year in ALS patients. This symmetrical decline is crucial to monitor, as it directly correlates with survival rates. For instance, when FVC drops below 50% of predicted value, the risk of respiratory failure increases exponentially, necessitating interventions like non-invasive ventilation (NIV).
Instructively, patients and caregivers must prioritize early detection of respiratory muscle weakness. Simple spirometry tests, performed every 3-6 months, can track FVC and identify symmetrical decline before symptoms become severe. Practical tips include maintaining an upright posture during sleep to optimize diaphragm function and practicing diaphragmatic breathing exercises to strengthen respiratory muscles. Additionally, avoiding supine positioning for extended periods can reduce the risk of atelectasis, a common complication in ALS patients with weakened respiratory muscles.
Persuasively, the symmetrical decline of respiratory muscles underscores the urgency of proactive respiratory care in ALS management. Delaying interventions like NIV or tracheostomy can lead to irreversible damage and decreased survival. Clinicians should educate patients about the importance of adhering to respiratory therapies, even in the absence of noticeable symptoms. For example, initiating NIV when FVC falls below 80% of predicted value has been shown to prolong survival by 6-12 months, highlighting the benefits of early intervention.
Comparatively, the symmetrical involvement of respiratory muscles in ALS contrasts with other muscle groups, where asymmetry is often more pronounced in the early stages. This distinction emphasizes the unique vulnerability of respiratory muscles to bilateral motor neuron loss. Unlike limb muscles, which may show focal weakness initially, respiratory muscles exhibit a more uniform decline, making them a reliable indicator of disease progression. This pattern also differentiates ALS from other motor neuron diseases, such as progressive muscular atrophy, where respiratory involvement may be less symmetrical.
In conclusion, the symmetrical decline of respiratory muscles in ALS is a critical aspect of disease management. By understanding this phenomenon, patients and clinicians can implement targeted strategies to preserve respiratory function and improve outcomes. Regular monitoring, early intervention, and patient education are essential components of a comprehensive approach to addressing this unique challenge in ALS care.
Optimize Your Workout: Ideal Daily Muscle Group Training Strategies
You may want to see also
Explore related products






![]()
Trunk Muscles and Symmetry in ALS
Amyotrophic lateral sclerosis (ALS) often presents with asymmetrical muscle involvement, but the trunk muscles—critical for posture, balance, and respiration—exhibit a unique pattern. Early symptoms in the trunk, such as scoliosis or difficulty maintaining an upright posture, may appear unilaterally, misleadingly suggesting localized weakness. However, as ALS progresses, the trunk muscles typically become bilaterally affected, though not always symmetrically. This asymmetry can complicate diagnosis, as patients may initially present with more pronounced weakness on one side, masking the disease’s systemic nature. Understanding this pattern is crucial for clinicians to differentiate ALS from other conditions like spinal stenosis or muscular dystrophy.
The trunk muscles, including the erector spinae, obliques, and intercostals, play a pivotal role in respiratory function, which is severely compromised in ALS. Asymmetrical weakness in these muscles can lead to uneven chest wall movement, reducing lung capacity more on one side than the other. For instance, a patient with pronounced right-sided trunk weakness may experience greater difficulty with deep inhalation, leading to increased risk of respiratory failure. Monitoring respiratory symmetry through spirometry and chest wall movement assessments can provide early indicators of disease progression, guiding interventions like non-invasive ventilation (NIV) or diaphragm pacing.
Rehabilitation strategies for trunk muscles in ALS must account for asymmetry to maximize functional independence. Physical therapists often employ targeted exercises, such as unilateral core stabilization drills, to address weaker sides while maintaining strength on the stronger side. For example, a patient with left-sided trunk weakness might perform side-lying leg lifts on the left to engage the obliques and quadratus lumborum. Caution must be taken to avoid overexertion, as ALS patients fatigue quickly; sessions should be limited to 20–30 minutes, with rest intervals every 5–10 minutes. Assistive devices like lumbar supports or custom braces can also help compensate for asymmetry, improving posture and reducing energy expenditure.
Comparatively, while limb muscles in ALS often show pronounced asymmetry, trunk muscle involvement tends to progress toward bilateral weakness more rapidly due to their continuous load-bearing role. This distinction highlights the need for proactive management of trunk muscles early in the disease course. Patients and caregivers should be educated on signs of trunk muscle deterioration, such as increased leaning to one side or difficulty rolling in bed. Early intervention, including respiratory therapy and tailored exercise programs, can delay the onset of severe respiratory compromise, a leading cause of mortality in ALS. By focusing on trunk symmetry, clinicians can improve both quality of life and survival outcomes for patients.
Optimal Rest Days for Muscle Recovery and Growth: A Guide
You may want to see also
Frequently asked questions
In the early stages of ALS, muscle involvement is often asymmetrical, meaning one side of the body may be affected before the other. However, as the disease progresses, muscle involvement typically becomes more symmetrical.
ALS is a neurodegenerative disease that affects motor neurons randomly. Initial symptoms often appear in one region due to the selective vulnerability of certain motor neurons, but over time, the disease spreads to involve both sides of the body.
While rare, some cases of ALS may remain predominantly asymmetrical, especially in certain subtypes like limb-onset ALS. However, most patients will experience progression to more symmetrical involvement as the disease advances.
Symmetrical muscle weakness, particularly in later stages, can be a key diagnostic indicator of ALS. However, early asymmetrical symptoms may initially mimic other conditions, making diagnosis more challenging.
Symmetrical involvement itself does not directly influence treatment, but it reflects disease progression. Patients with rapid progression to symmetrical weakness may have a more aggressive disease course, which can impact prognosis and management strategies.