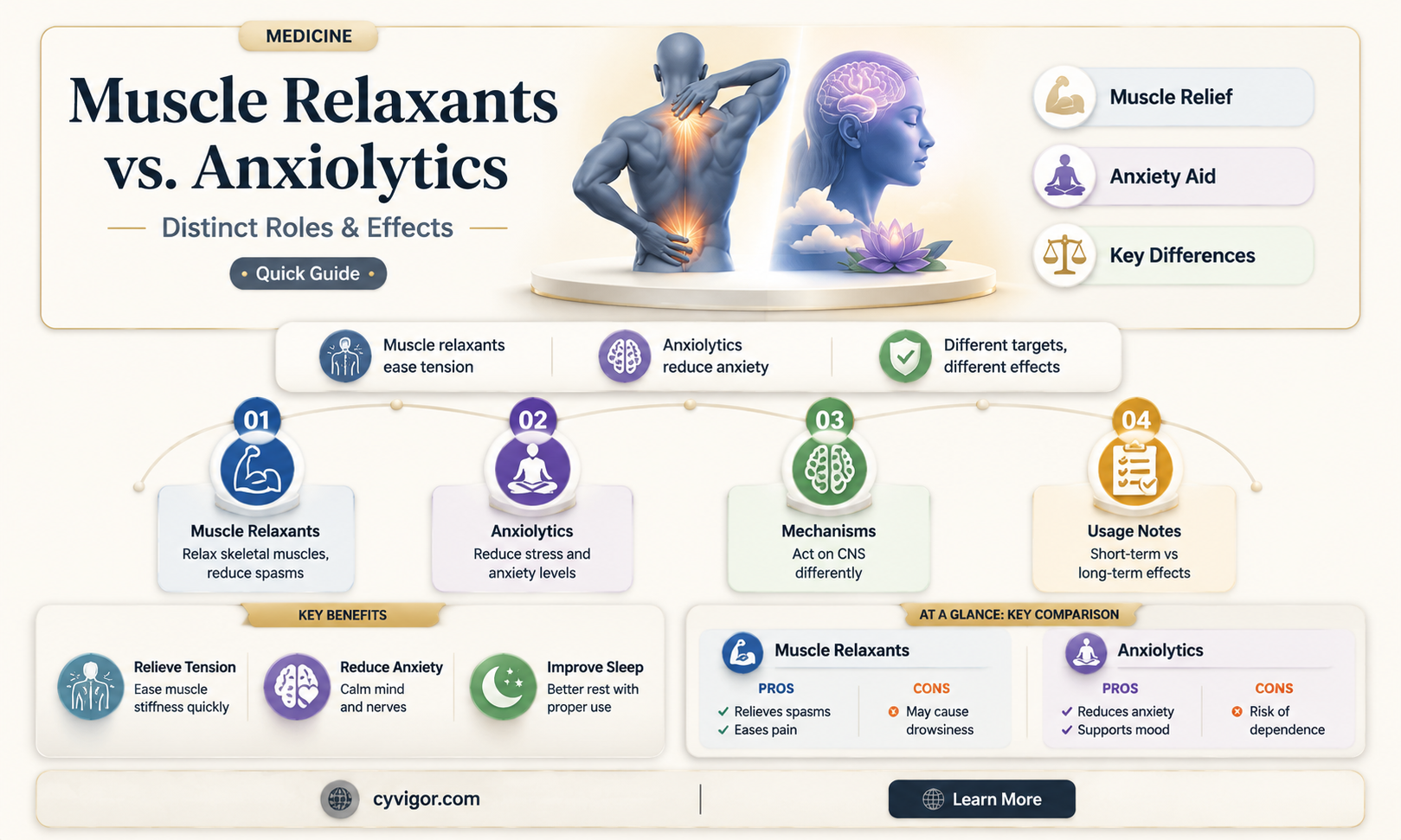
Muscle relaxants and anxiolytics are two distinct classes of medications often used to manage different symptoms, yet their mechanisms of action and effects can sometimes overlap, leading to questions about their interchangeability. Muscle relaxants primarily target skeletal muscle to alleviate pain and discomfort associated with muscle spasms or tension, often acting on the central nervous system or neuromuscular junctions. Anxiolytics, on the other hand, are designed to reduce anxiety and promote relaxation by modulating neurotransmitters like GABA in the brain. While some muscle relaxants, such as cyclobenzaprine and tizanidine, may have sedative effects that indirectly reduce anxiety, they are not classified as anxiolytics. Conversely, certain anxiolytics, like benzodiazepines, can cause muscle relaxation as a secondary effect. Understanding the differences and potential overlaps between these medications is crucial for appropriate prescribing and patient management, as misuse or confusion between the two can lead to suboptimal treatment outcomes or adverse effects.
| Characteristics | Values |
|---|---|
| Definition | Muscle relaxants are drugs that relieve muscle spasms or stiffness, while anxiolytics are medications used to reduce anxiety. |
| Mechanism of Action | Muscle relaxants act on the central nervous system (CNS) or directly on muscles, whereas anxiolytics primarily target GABA receptors in the brain to reduce anxiety. |
| Primary Use | Muscle relaxants are used for musculoskeletal conditions (e.g., back pain, spasms), while anxiolytics are used for anxiety disorders. |
| Overlap in Effects | Some muscle relaxants (e.g., cyclobenzaprine, tizanidine) have sedative effects and may reduce anxiety as a secondary effect. |
| Classification | Muscle relaxants are not classified as anxiolytics, but some may have anxiolytic-like properties due to their CNS effects. |
| Examples | Muscle relaxants: Baclofen, Cyclobenzaprine, Tizanidine; Anxiolytics: Benzodiazepines (e.g., Diazepam), SSRIs, Buspirone. |
| Side Effects | Muscle relaxants: Drowsiness, dizziness, weakness; Anxiolytics: Sedation, dependence, cognitive impairment. |
| Addiction Potential | Some muscle relaxants (e.g., carisoprodol) and anxiolytics (e.g., benzodiazepines) have addiction potential. |
| Medical Supervision | Both types of drugs typically require prescription and medical supervision due to potential risks. |
| Cross-Use | Some muscle relaxants may be prescribed off-label for anxiety, but this is not their primary indication. |
| Pharmacological Class | Muscle relaxants are distinct from anxiolytics in pharmacological classification, though there may be functional overlap. |
Explore related products






What You'll Learn
- Mechanism of Action: How muscle relaxants and anxiolytics differ in brain and body effects
- Overlap in Use: Conditions where muscle relaxants are prescribed for anxiety-related symptoms
- Side Effect Comparison: Sedation, drowsiness, and other shared or distinct side effects
- Pharmacological Classification: Why muscle relaxants are not classified as anxiolytics despite similarities
- Clinical Evidence: Studies on muscle relaxants' efficacy in reducing anxiety symptoms
![]()
Mechanism of Action: How muscle relaxants and anxiolytics differ in brain and body effects
Muscle relaxants and anxiolytics, though sometimes used interchangeably in casual conversation, operate through distinct mechanisms in the brain and body. Muscle relaxants primarily target the neuromuscular system, reducing muscle spasms and tension by inhibiting nerve impulses or altering muscle fiber function. For instance, baclofen, a common muscle relaxant, acts as a GABA-B receptor agonist in the spinal cord, dampening the release of excitatory neurotransmitters like glutamate. This localized action explains why muscle relaxants are effective for conditions like lower back pain or multiple sclerosis but do not directly address anxiety.
In contrast, anxiolytics work centrally in the brain to modulate neurotransmitter systems associated with fear and stress responses. Benzodiazepines, a well-known class of anxiolytics, enhance the activity of GABA-A receptors, increasing chloride ion influx and producing a calming effect. This broad action on the central nervous system not only reduces anxiety but can also induce sedation and cognitive impairment, particularly at higher doses (e.g., 2-10 mg of diazepam for anxiety). Unlike muscle relaxants, anxiolytics are designed to cross the blood-brain barrier, making them potent tools for managing generalized anxiety disorder or panic attacks.
A key difference lies in their side effect profiles and safety considerations. Muscle relaxants like cyclobenzaprine (10-30 mg daily) can cause drowsiness and dizziness but are generally safer for long-term use in musculoskeletal conditions. Anxiolytics, however, carry a higher risk of dependence and withdrawal, especially with prolonged use. For example, abruptly discontinuing benzodiazepines after more than 4-6 weeks of use can lead to rebound anxiety or seizures. This distinction underscores the importance of tailoring treatment to the underlying condition—muscle relaxants for physical symptoms and anxiolytics for psychological distress.
Practical application further highlights their differences. A patient with chronic neck pain might benefit from a muscle relaxant like tizanidine (2-8 mg) before bedtime to improve sleep quality without addressing daytime anxiety. Conversely, someone with social anxiety disorder may require an anxiolytic like buspirone (10-30 mg daily) to manage anticipatory fear, even if muscle tension is a secondary symptom. Combining these medications requires caution, as both classes can cause sedation, and their additive effects may impair motor function or cognitive performance.
In summary, while muscle relaxants and anxiolytics may superficially overlap in their sedative properties, their mechanisms of action and clinical applications diverge significantly. Understanding these differences ensures appropriate prescribing practices and minimizes adverse outcomes. For instance, a 45-year-old with fibromyalgia might tolerate a muscle relaxant well but could experience worsened anxiety if misprescribed an anxiolytic without addressing the root cause of their muscle pain. Always consider the patient’s age, comorbidities, and medication history to optimize therapy.
Can Teladoc Prescribe Muscle Relaxers? What You Need to Know
You may want to see also
Explore related products






![]()
Overlap in Use: Conditions where muscle relaxants are prescribed for anxiety-related symptoms
Muscle relaxants, primarily designed to alleviate muscle spasms and pain, often find their way into the treatment regimens of individuals experiencing anxiety-related symptoms. This overlap in use is particularly evident in conditions where physical tension and psychological distress are intertwined. For instance, patients with generalized anxiety disorder (GAD) frequently report muscle stiffness and chronic pain, which can exacerbate their anxiety. In such cases, muscle relaxants like cyclobenzaprine (Flexeril) or tizanidine (Zanaflex) may be prescribed off-label to address both the physical and emotional components of the disorder. These medications work by reducing muscle tension, which can indirectly alleviate the anxiety associated with physical discomfort.
Consider the scenario of a 35-year-old patient with panic disorder who experiences frequent muscle spasms during panic attacks. Here, a muscle relaxant such as baclofen might be introduced at a starting dose of 5 mg three times daily, gradually increasing to 10–20 mg three times daily as tolerated. The goal is to mitigate the physical symptoms of panic, thereby reducing the overall anxiety burden. However, it’s crucial to monitor for side effects like drowsiness or dizziness, which can complicate daily functioning. This approach underscores the importance of tailoring treatment to the individual’s specific symptom profile.
From a comparative perspective, muscle relaxants differ from traditional anxiolytics like benzodiazepines in their mechanism of action. While benzodiazepines directly target the central nervous system to induce calmness, muscle relaxants primarily act on the musculoskeletal system. Yet, their sedative properties often provide a secondary anxiolytic effect, making them a viable option for patients who cannot tolerate or prefer to avoid benzodiazepines. For example, older adults with anxiety and comorbid arthritis might benefit from methocarbamol (Robaxin), which has a lower risk of cognitive impairment compared to benzodiazepines.
A persuasive argument for this overlap in use lies in the holistic management of anxiety disorders. By addressing both the physical and psychological manifestations of anxiety, clinicians can achieve more comprehensive symptom relief. Practical tips for patients include maintaining a consistent dosing schedule, avoiding alcohol to prevent potentiation of sedative effects, and incorporating non-pharmacological strategies like mindfulness or physical therapy to enhance the benefits of muscle relaxants. This integrated approach not only improves treatment efficacy but also fosters a sense of control and empowerment in managing anxiety.
In conclusion, the prescription of muscle relaxants for anxiety-related symptoms reflects a nuanced understanding of the mind-body connection in mental health. While not classified as anxiolytics, their role in alleviating physical tension can significantly reduce anxiety, particularly in conditions where the two are closely linked. Clinicians must weigh the benefits against potential risks, such as dependence or side effects, and consider individual patient needs when incorporating these medications into treatment plans. This targeted approach highlights the evolving landscape of anxiety management, where interdisciplinary strategies yield the most promising outcomes.
Expired Muscle Relaxers: Are They Safe to Use or Risky?
You may want to see also
Explore related products






![]()
Side Effect Comparison: Sedation, drowsiness, and other shared or distinct side effects
Muscle relaxants and anxiolytics, while serving different primary purposes, often share a common side effect profile that includes sedation and drowsiness. These effects can significantly impact daily functioning, making it crucial to understand their nuances. For instance, cyclobenzaprine, a muscle relaxant, is known to cause pronounced drowsiness, particularly at higher doses (10–30 mg/day), whereas benzodiazepines like diazepam, commonly used as anxiolytics, induce sedation more consistently across their dosage range (2–10 mg/day). Both classes of drugs act on the central nervous system, but their mechanisms differ—muscle relaxants target skeletal muscle function, while anxiolytics modulate GABA receptors to reduce anxiety. Despite these differences, their overlapping side effects necessitate careful consideration in clinical practice.
When comparing sedation and drowsiness, it’s essential to note their distinct implications for patients. Sedation often manifests as a deeper state of relaxation or calmness, which can impair cognitive and motor functions. This is particularly problematic for older adults (aged 65 and above), who are more susceptible to falls and confusion due to age-related pharmacokinetic changes. Drowsiness, on the other hand, is characterized by a persistent urge to sleep, which can disrupt daily activities like driving or operating machinery. For example, a patient prescribed tizanidine (a muscle relaxant) at 4 mg three times daily may experience significant drowsiness, whereas someone on a low dose of lorazepam (an anxiolytic) at 0.5 mg may report milder sedation. Tailoring dosages and monitoring patient responses are critical to minimizing these risks.
Beyond sedation and drowsiness, muscle relaxants and anxiolytics exhibit other shared and distinct side effects. Both classes can cause dizziness, headache, and gastrointestinal disturbances such as nausea or constipation. However, muscle relaxants like baclofen may lead to specific side effects such as muscle weakness or coordination problems, which are less common with anxiolytics. Conversely, anxiolytics, particularly benzodiazepines, carry a higher risk of dependence and withdrawal symptoms, especially with long-term use. For instance, abruptly discontinuing alprazolam after prolonged use can result in rebound anxiety or seizures. Patients should be educated about these risks and advised to taper doses under medical supervision.
Practical tips can help mitigate these side effects. For muscle relaxants, starting with the lowest effective dose (e.g., 5 mg of cyclobenzaprine) and gradually titrating upward can reduce the severity of drowsiness. Similarly, taking these medications at bedtime can align their sedative effects with sleep, minimizing daytime impairment. For anxiolytics, combining pharmacotherapy with non-pharmacological interventions like cognitive-behavioral therapy can reduce reliance on medication and lower the risk of dependence. Additionally, avoiding alcohol and other central nervous system depressants is crucial, as they can exacerbate sedation and drowsiness. Patients should also be encouraged to report any persistent or severe side effects promptly to their healthcare provider for timely intervention.
In conclusion, while muscle relaxants and anxiolytics share side effects like sedation and drowsiness, their distinct profiles and risks require individualized management. Understanding these differences enables healthcare providers to optimize treatment outcomes while minimizing adverse effects. Patients, too, play a vital role in monitoring their responses and adhering to prescribed guidelines. By balancing efficacy with safety, clinicians can ensure that these medications provide relief without compromising quality of life.
Is Vicodin a Muscle Relaxer? Understanding Its Uses and Effects
You may want to see also
Explore related products






![]()
Pharmacological Classification: Why muscle relaxants are not classified as anxiolytics despite similarities
Muscle relaxants and anxiolytics often share symptomatic overlap, particularly in their ability to induce calmness and reduce tension. However, their pharmacological mechanisms and intended uses diverge significantly, leading to distinct classifications. Muscle relaxants primarily target skeletal muscle spasms through actions on the central nervous system (CNS) or neuromuscular junction, while anxiolytics act on neurotransmitter systems like GABA to alleviate anxiety. For instance, cyclobenzaprine, a muscle relaxant, works by inhibiting norepinephrine uptake, whereas benzodiazepines like diazepam enhance GABAergic inhibition. This fundamental difference in mechanism underscores why muscle relaxants are not categorized as anxiolytics, despite their superficial similarities.
Consider the clinical application of these drugs. Muscle relaxants such as tizanidine or baclofen are prescribed for conditions like lower back pain or multiple sclerosis, often at doses of 2–4 mg (tizanidine) or 10–20 mg (baclofen) three times daily. Anxiolytics, on the other hand, are used for generalized anxiety disorder or panic attacks, with benzodiazepines like alprazolam dosed at 0.25–0.5 mg as needed. While both classes may produce sedation, muscle relaxants are not indicated for anxiety management due to their targeted action on muscle spasticity rather than emotional regulation. Misclassification could lead to inappropriate prescribing, such as using a muscle relaxant to treat anxiety, which lacks efficacy and may exacerbate side effects like dizziness or fatigue.
A comparative analysis highlights the importance of pharmacological specificity. Anxiolytics modulate emotional responses by directly influencing limbic system activity, whereas muscle relaxants focus on motor neuron excitability. For example, benzodiazepines increase chloride conductance via GABA receptors, producing anxiolysis, while methocarbamol, a muscle relaxant, acts peripherally to reduce muscle fiber tension. This distinction is critical for healthcare providers, as prescribing a muscle relaxant for anxiety would be akin to using a hammer to tighten a screw—ineffective and potentially harmful. Patients should also be educated on these differences to avoid self-medication errors, especially given the overlap in side effects like drowsiness.
Finally, regulatory and safety considerations reinforce the separate classification of these drugs. Muscle relaxants often carry warnings about impaired motor function, making them unsuitable for anxiety treatment, where cognitive clarity is essential. Anxiolytics, particularly benzodiazepines, are scheduled substances due to their abuse potential, whereas most muscle relaxants are not. This regulatory distinction reflects their unique risk profiles and intended uses. For practical guidance, clinicians should assess the primary symptom—muscle spasm or anxiety—and prescribe accordingly, ensuring patients understand the rationale behind the choice. This precision in classification and prescribing optimizes therapeutic outcomes while minimizing adverse effects.
Muscle Relaxers and Body Toning: Impact on Fitness Goals
You may want to see also
Explore related products






![]()
Clinical Evidence: Studies on muscle relaxants' efficacy in reducing anxiety symptoms
Muscle relaxants, primarily prescribed for musculoskeletal conditions, have been investigated for their potential anxiolytic effects, but clinical evidence remains limited and nuanced. Studies often focus on drugs like tizanidine, baclofen, and cyclobenzaprine, which act on the central nervous system to reduce muscle spasms. A 2018 randomized controlled trial published in *The Journal of Clinical Psychiatry* examined tizanidine’s efficacy in generalized anxiety disorder (GAD) patients. Participants received 4 mg of tizanidine twice daily for six weeks, with results showing a modest reduction in anxiety symptoms compared to placebo. However, the study noted significant side effects, including drowsiness and dizziness, which limited its practicality for long-term anxiety management.
In contrast, baclofen, traditionally used for spasticity in conditions like multiple sclerosis, has shown mixed results in anxiety reduction. A 2020 meta-analysis in *Neuropsychiatric Disease and Treatment* reviewed six studies involving baclofen dosages ranging from 10 to 60 mg/day. While some participants reported decreased anxiety, particularly in those with comorbid alcohol use disorder, the overall effect size was small, and the mechanism remains unclear. Researchers hypothesize that baclofen’s action on GABA-B receptors may contribute to its anxiolytic properties, but further studies are needed to confirm this.
Cyclobenzaprine, another commonly studied muscle relaxant, has been explored in low doses (5–10 mg/day) for anxiety symptoms. A 2019 pilot study in *Primary Care Companion for CNS Disorders* found that patients with chronic pain and comorbid anxiety experienced a 30% reduction in anxiety scores after four weeks of treatment. However, the study’s small sample size and lack of a control group limit its generalizability. Clinicians often caution against using cyclobenzaprine solely for anxiety due to its sedative effects, which can impair daily functioning.
Practical considerations for using muscle relaxants as anxiolytics include patient age, comorbidities, and potential drug interactions. For instance, older adults are more susceptible to side effects like confusion and falls, making these drugs less ideal for this demographic. Additionally, muscle relaxants should not replace first-line anxiety treatments like SSRIs or cognitive-behavioral therapy. Instead, they may serve as adjunctive therapy in specific cases, such as patients with both chronic pain and anxiety. Always start with the lowest effective dose and monitor closely for adverse reactions.
In conclusion, while some clinical evidence suggests muscle relaxants may reduce anxiety symptoms, their efficacy is inconsistent and often outweighed by side effects. These drugs are not FDA-approved for anxiety disorders, and their use in this context remains off-label. Clinicians should approach this strategy cautiously, reserving it for patients who have not responded to conventional anxiolytics and ensuring thorough patient education about risks and benefits.
Muscle Relaxers and Antihistamines: Understanding Their Connection and Effects
You may want to see also
Frequently asked questions
No, muscle relaxants and anxiolytics are different classes of medications. Muscle relaxants primarily target muscle spasms and pain by acting on the central nervous system or directly on muscles, while anxiolytics are specifically designed to reduce anxiety and promote relaxation by affecting neurotransmitters in the brain.
While some muscle relaxants may have mild sedative effects that could indirectly help with anxiety, they are not approved or primarily prescribed for treating anxiety disorders. Anxiolytics, such as benzodiazepines or SSRIs, are more appropriate for managing anxiety symptoms.
Some anxiolytics, particularly benzodiazepines, can have muscle-relaxing properties as a secondary effect due to their sedative and calming actions. However, they are not as targeted or effective for muscle spasms as dedicated muscle relaxants, and their primary use remains anxiety management.