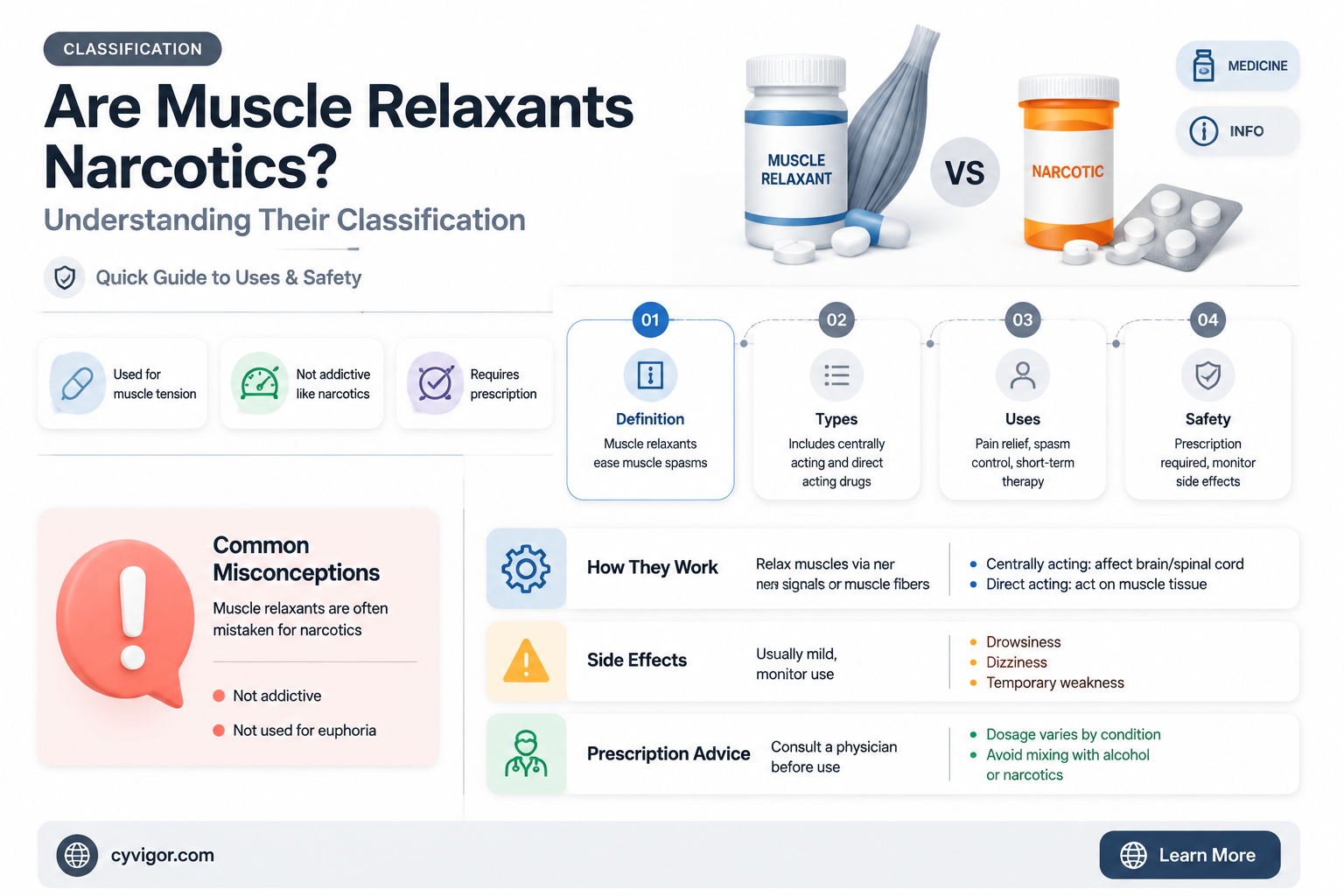
Muscle relaxants and narcotics are often confused due to their potential for misuse and overlapping effects, but they serve distinct medical purposes. Muscle relaxants are primarily used to alleviate muscle spasms and pain by acting on the central nervous system or directly on muscles, while narcotics, also known as opioids, are potent pain relievers that work by binding to opioid receptors in the brain and spinal cord. Although both can induce sedation and have the potential for dependence, muscle relaxants are not classified as narcotics. Understanding the differences between these medications is crucial for safe and effective use, as misclassification can lead to improper prescribing and increased risks of side effects or addiction.
| Characteristics | Values |
|---|---|
| Classification | Muscle relaxants are not classified as narcotics. They are typically categorized as either centrally acting (affecting the brain and spinal cord) or peripherally acting (acting on muscles directly). |
| Mechanism of Action | Centrally acting muscle relaxants work by inhibiting neuronal activity in the central nervous system, while peripherally acting ones act on neuromuscular junctions. |
| Examples | Centrally acting: Baclofen, Tizanidine, Cyclobenzaprine; Peripherally acting: Botulinum toxin, Dantrolene. |
| Addiction Potential | Generally lower addiction potential compared to narcotics, but some centrally acting muscle relaxants may cause dependence with prolonged use. |
| Prescription Status | Requires a prescription; not available over the counter. |
| Side Effects | Drowsiness, dizziness, dry mouth, fatigue, and in some cases, liver toxicity (e.g., with methocarbamol). |
| Drug Interactions | Can interact with alcohol, sedatives, and other CNS depressants, increasing the risk of side effects. |
| Legal Status | Not controlled substances like narcotics, but misuse can lead to regulatory scrutiny. |
| Medical Uses | Treatment of muscle spasms, spasticity, and pain associated with musculoskeletal conditions. |
| Overdose Risk | Lower risk compared to narcotics, but overdose can cause severe drowsiness, respiratory depression, or coma in extreme cases. |
Explore related products






What You'll Learn
![]()
Definition of Muscle Relaxants
Muscle relaxants are a class of medications primarily designed to alleviate muscle spasms, stiffness, and pain by acting on the central nervous system or directly on muscles. Unlike narcotics, which are opioid-based pain relievers, muscle relaxants do not target the brain’s opioid receptors. Instead, they modulate nerve signals or interfere with muscle fiber contractions to produce relaxation. Common examples include baclofen, cyclobenzaprine, and tizanidine, each with distinct mechanisms and applications. For instance, baclofen mimics GABA, a neurotransmitter that inhibits nerve activity, while tizanidine directly suppresses spinal cord signals to reduce muscle tone.
When prescribing muscle relaxants, healthcare providers consider factors like age, medical history, and the underlying cause of muscle tension. Dosages vary widely; cyclobenzaprine is typically started at 5 mg three times daily, while tizanidine may begin at 2 mg every six to eight hours, titrated up to 24 mg daily if needed. Elderly patients often require lower doses due to slower metabolism and increased sensitivity to side effects, such as drowsiness or dizziness. It’s crucial to follow dosage instructions carefully, as misuse can lead to sedation, impaired coordination, or even respiratory depression in severe cases.
One key distinction between muscle relaxants and narcotics is their potential for dependence. While muscle relaxants can cause physical dependence with prolonged use, they are not classified as controlled substances in the same way opioids are. Narcotics, such as oxycodone or morphine, carry a high risk of addiction and are tightly regulated due to their euphoric effects. Muscle relaxants, on the other hand, are generally prescribed for short-term use (2–3 weeks) to manage acute conditions like back spasms or injury-related stiffness. Patients should avoid alcohol and other central nervous system depressants while taking these medications to prevent dangerous interactions.
Practical tips for using muscle relaxants include taking them at bedtime to minimize daytime drowsiness, especially with sedating options like cyclobenzaprine. Physical therapy and stretching exercises often complement medication to improve long-term outcomes. For chronic conditions like multiple sclerosis or cerebral palsy, baclofen may be administered via an intrathecal pump to deliver precise doses directly to the spinal fluid, bypassing systemic side effects. Always consult a healthcare provider before starting or stopping muscle relaxants, as abrupt discontinuation can trigger withdrawal symptoms like insomnia or rebound muscle pain.
In summary, muscle relaxants are distinct from narcotics in their mechanism, purpose, and regulatory status. They offer targeted relief for muscle-related issues without the addictive properties of opioids, making them a safer option for many patients. However, their use requires careful consideration of dosage, duration, and potential side effects to ensure both efficacy and safety. By understanding these differences, patients and providers can make informed decisions about managing musculoskeletal pain and discomfort.
Tiger Balm for Muscle Relaxation: Does It Really Work?
You may want to see also
Explore related products






![]()
Definition of Narcotics
Narcotics, by definition, are substances that induce sleep, relieve pain, and alter mood or behavior, primarily by acting on the central nervous system. They are typically derived from opium or synthesized to mimic its effects, and they include drugs like morphine, codeine, and heroin. The term "narcotic" is often used interchangeably with "opioid," though in a legal context, it may encompass a broader range of substances. Understanding this definition is crucial when discussing whether muscle relaxants fall into this category, as it hinges on their mechanism of action and intended effects.
Analytically, narcotics are distinguished by their ability to bind to opioid receptors in the brain and spinal cord, modulating pain perception and producing euphoria. For instance, morphine is prescribed in doses ranging from 10 to 30 mg every 4 hours for pain management, while heroin, an illicit narcotic, has no standardized dosage but carries a high risk of overdose due to its potency and variability. Muscle relaxants, on the other hand, primarily target skeletal muscle or the nervous system to reduce muscle spasms, not opioid receptors. This fundamental difference in mechanism suggests that muscle relaxants are not narcotics, despite both being used for pain-related conditions.
From a practical standpoint, distinguishing narcotics from muscle relaxants is essential for safe prescribing and patient education. Narcotics carry significant risks, including dependence, respiratory depression, and overdose, particularly when used long-term or in high doses. For example, patients over 65 are more susceptible to the sedative effects of narcotics, increasing the risk of falls. Muscle relaxants, such as cyclobenzaprine or baclofen, are generally safer for muscle-related pain but can cause drowsiness or dizziness. Patients should be advised to avoid alcohol and operate machinery cautiously when using either class of medication, though the underlying reasons for these precautions differ.
Comparatively, while both narcotics and muscle relaxants can alleviate pain-related symptoms, their applications and risks diverge sharply. Narcotics are reserved for severe acute or chronic pain, often in palliative care or post-surgical settings, whereas muscle relaxants are typically used for acute musculoskeletal conditions like back spasms. For instance, a patient with post-operative pain might receive hydrocodone (a narcotic), while someone with a strained muscle might be prescribed tizanidine (a muscle relaxant). This distinction underscores the importance of precise diagnosis and tailored treatment to avoid misclassification and misuse.
In conclusion, the definition of narcotics centers on their opioid-based mechanism and effects on the central nervous system, setting them apart from muscle relaxants. While both classes address pain-related issues, their pharmacological actions, risks, and appropriate uses differ significantly. Recognizing these differences ensures safer and more effective treatment, highlighting why muscle relaxants are not classified as narcotics despite occasional overlaps in their therapeutic applications.
Muscle Relaxer Timing: When to Expect Relief After Taking It
You may want to see also
Explore related products






![]()
Classification Differences
Muscle relaxants and narcotics are often confused due to their overlapping effects on the body, but their classifications differ significantly. Muscle relaxants, such as cyclobenzaprine and tizanidine, primarily target the central nervous system to alleviate muscle spasms and pain. They are typically classified as skeletal muscle relaxants or antispasmodics, not as narcotics. Narcotics, on the other hand, are opioids like morphine, oxycodone, and hydrocodone, which act on the brain’s opioid receptors to relieve pain and induce euphoria. This fundamental difference in mechanism and purpose underscores their distinct classifications.
From a regulatory standpoint, muscle relaxants and narcotics are treated differently. In the United States, muscle relaxants are generally classified as Schedule II, III, or IV controlled substances, depending on their potential for abuse and dependence. For example, carisoprodol (Soma) is a Schedule IV drug, indicating a lower risk compared to narcotics. Narcotics, however, are predominantly Schedule II drugs, reflecting their high potential for abuse and severe dependence. This classification affects prescribing practices, with narcotics requiring stricter monitoring and shorter prescription durations. Patients prescribed narcotics often face more stringent regulations, such as mandatory urine drug tests or participation in pain management programs.
Clinically, the use cases for muscle relaxants and narcotics diverge sharply. Muscle relaxants are typically prescribed for acute musculoskeletal conditions, such as lower back pain or injury-related spasms, with recommended dosages like 5–10 mg of cyclobenzaprine up to three times daily. They are often used for short durations, usually no more than 2–3 weeks, due to their sedative effects and potential for tolerance. Narcotics, in contrast, are reserved for severe pain, such as post-surgical recovery or cancer-related pain, with dosages tailored to the patient’s pain level and tolerance. For instance, oxycodone may start at 5 mg every 4–6 hours, adjusted as needed. The prolonged use of narcotics carries a higher risk of addiction, making them a last-resort option for chronic pain management.
Understanding these classification differences is crucial for both healthcare providers and patients. Misclassification can lead to inappropriate prescribing, increasing the risk of adverse effects or dependency. For example, using a narcotic for a condition better suited to a muscle relaxant could expose the patient to unnecessary risks. Conversely, underestimating the severity of pain and prescribing a muscle relaxant instead of a narcotic may result in inadequate relief. Patients should also be aware of these distinctions to advocate for their care effectively, such as questioning why a narcotic is being prescribed for a condition that might respond better to a muscle relaxant.
In practical terms, patients can take steps to ensure they receive the appropriate medication. Always discuss the nature of your pain with your healthcare provider, specifying its intensity, duration, and impact on daily activities. Ask about the medication’s classification and potential side effects, such as drowsiness from muscle relaxants or constipation from narcotics. For muscle relaxants, avoid activities requiring alertness, like driving, until you know how the drug affects you. If prescribed a narcotic, adhere strictly to the dosage instructions and report any signs of dependence, such as cravings or withdrawal symptoms. By understanding these classification differences, patients and providers can collaborate to achieve optimal pain management while minimizing risks.
Post-CrossFit Muscle Recovery: How Long Until Your Muscles Relax?
You may want to see also
Explore related products






![]()
Common Muscle Relaxants
Muscle relaxants are a diverse group of medications designed to alleviate muscle spasms, pain, and stiffness, but they are not classified as narcotics. Narcotics, or opioids, primarily target the central nervous system to relieve pain and induce sedation, whereas muscle relaxants work by acting on the nervous system to reduce muscle tension. Understanding this distinction is crucial for patients and healthcare providers to manage expectations and potential side effects.
One of the most commonly prescribed muscle relaxants is Cyclobenzaprine (Flexeril). Typically administered in 5 to 10 mg doses up to three times daily, it is effective for acute musculoskeletal conditions but may cause drowsiness and dizziness. Patients are advised to avoid alcohol and activities requiring alertness while on this medication. Another widely used option is Tizanidine (Zanaflex), which is often dosed at 2 to 4 mg every 6 to 8 hours, with a maximum daily limit of 36 mg. Tizanidine is unique in its ability to reduce muscle spasms without causing significant sedation, making it suitable for patients who need to remain functional during the day.
For those seeking a shorter-acting option, Methocarbamol (Robaxin) is frequently prescribed. Dosages range from 1,500 to 4,500 mg daily, divided into multiple doses. It is less sedating than cyclobenzaprine but may still impair coordination, so caution is advised when driving or operating machinery. Baclofen, another common muscle relaxant, is often used for spasticity associated with conditions like multiple sclerosis or spinal cord injuries. Starting doses are typically 5 mg three times daily, gradually increasing to a maximum of 80 mg daily under medical supervision.
It’s important to note that while these medications are not narcotics, they still carry risks. Side effects such as drowsiness, dry mouth, and fatigue are common across most muscle relaxants. Patients with liver or kidney disease, or those taking other central nervous system depressants, should use these medications cautiously. Always follow the prescribed dosage and consult a healthcare provider before combining muscle relaxants with other drugs or supplements. Proper use ensures maximum benefit with minimal risk, making these medications valuable tools in managing muscle-related discomfort.
Muscle Relaxers and Pain Relief: Understanding Their Role in Pain Management
You may want to see also
Explore related products






![]()
Potential for Abuse
Muscle relaxants, while primarily prescribed for musculoskeletal conditions, carry a notable risk of abuse due to their sedative and euphoric effects. Unlike opioids, they are not classified as narcotics, but their potential for misuse warrants careful consideration. For instance, drugs like carisoprodol (Soma) and cyclobenzaprine (Flexeril) are frequently diverted for non-medical use, often in combination with alcohol or other central nervous system depressants. This behavior amplifies their effects but also increases the risk of respiratory depression, overdose, and addiction.
The mechanism of abuse often stems from the drug’s ability to induce relaxation and mild euphoria, particularly at higher doses. Carisoprodol, for example, metabolizes into meprobamate, a substance with anxiolytic properties that can foster psychological dependence. Users may escalate dosage beyond the recommended 250–350 mg three times daily, seeking intensified effects. Similarly, cyclobenzaprine’s dosage of 5–10 mg three times daily can be exceeded, leading to dizziness, confusion, and hallucinations. These behaviors are especially prevalent among individuals with a history of substance use disorders or those seeking self-medication for stress or anxiety.
To mitigate abuse potential, healthcare providers must adhere to strict prescribing guidelines. Muscle relaxants should be prescribed for short durations—typically 2–3 weeks—and only when physical therapy or other non-pharmacological interventions are insufficient. Patients with a history of addiction or those under 18 should be closely monitored, as adolescents are more susceptible to misuse due to developmental brain vulnerabilities. Pharmacists play a critical role by verifying prescriptions and educating patients about the risks of sharing medications.
Practical tips for patients include storing medications securely, avoiding alcohol consumption while on these drugs, and reporting any unusual side effects immediately. If dependence is suspected, tapering under medical supervision is essential to prevent withdrawal symptoms such as insomnia, headache, or rebound muscle pain. Public awareness campaigns highlighting the dangers of misuse can also deter recreational use. While muscle relaxants are not narcotics, their abuse potential demands vigilance from both providers and patients to ensure safe and effective use.
Muscle Relaxants and Sexual Function: What You Need to Know
You may want to see also
Frequently asked questions
No, muscle relaxants are not classified as narcotics. Narcotics typically refer to opioid pain medications, while muscle relaxants are a separate class of drugs used to alleviate muscle spasms and pain.
Some muscle relaxants may cause drowsiness or sedation, which can be similar to side effects of narcotics. However, they do not produce the same euphoric or addictive effects associated with opioid narcotics.
Muscle relaxants generally have a lower risk of addiction compared to narcotics. However, some types, such as carisoprodol, can be habit-forming if misused or taken for extended periods. Always follow your doctor’s prescription to minimize risks.