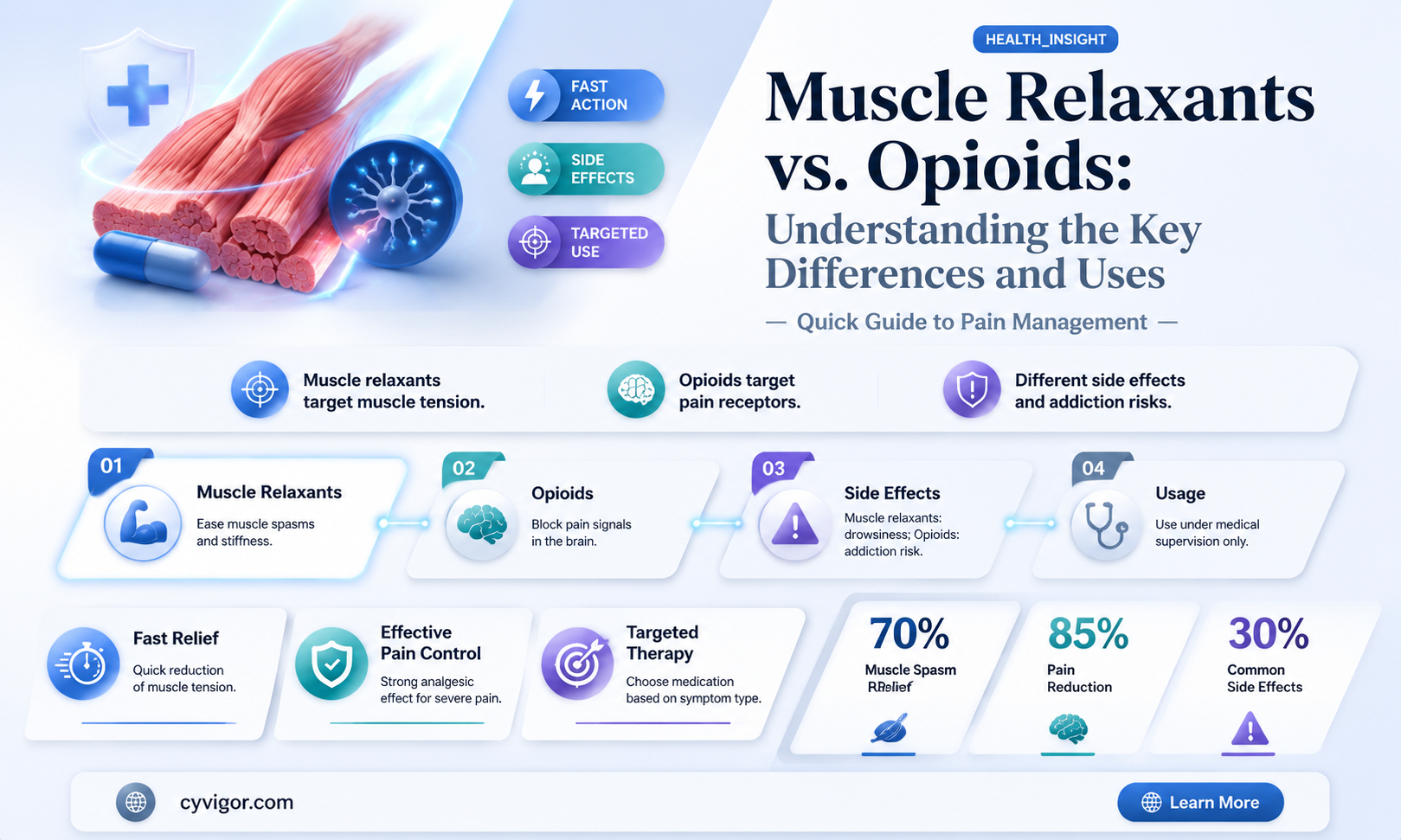
Muscle relaxants and opioids are both classes of medications used to manage pain, but they function in distinct ways and serve different purposes. While opioids, such as morphine or oxycodone, primarily target the central nervous system to alleviate pain by binding to opioid receptors, muscle relaxants work by reducing muscle spasms and tension, often acting directly on the muscles or the spinal cord. Despite their shared role in pain management, muscle relaxants are not classified as opioids, as they do not produce the same euphoric effects or carry the same risk of addiction and dependence. Understanding the differences between these two types of medications is crucial for safe and effective treatment, especially in addressing conditions like chronic pain or musculoskeletal injuries.
Explore related products






What You'll Learn
- Definition and Classification: Differentiating muscle relaxants from opioids based on their pharmacological properties
- Mechanism of Action: How muscle relaxants and opioids affect the nervous system differently
- Medical Uses: Comparing therapeutic applications of muscle relaxants versus opioids in pain management
- Side Effects and Risks: Contrasting potential adverse effects and addiction risks between the two
- Drug Interactions: Key differences in how muscle relaxants and opioids interact with other medications
![]()
Definition and Classification: Differentiating muscle relaxants from opioids based on their pharmacological properties
Muscle relaxants and opioids are often confused due to their overlapping use in pain management, but their pharmacological properties and mechanisms of action are distinct. Muscle relaxants primarily target the central nervous system (CNS) or neuromuscular junction to reduce muscle spasms and tension, while opioids act on the CNS to alter pain perception and emotional response. For instance, cyclobenzaprine, a common muscle relaxant, works by inhibiting nerve impulses in the brain and spinal cord, whereas morphine, an opioid, binds to mu-opioid receptors to produce analgesia and euphoria. This fundamental difference in action underscores the need for clear classification to guide appropriate prescribing practices.
Pharmacologically, muscle relaxants are classified into two main categories: centrally acting and peripherally acting. Centrally acting muscle relaxants, such as baclofen and tizanidine, modulate neurotransmitter release in the spinal cord, often targeting gamma-aminobutyric acid (GABA) receptors. These are typically prescribed for conditions like spasticity in multiple sclerosis or spinal cord injuries. Peripherally acting relaxants, like botulinum toxin, act directly on muscle fibers or the neuromuscular junction, making them suitable for localized muscle disorders. Opioids, in contrast, are classified based on their receptor affinity and potency, with examples including weak opioids like codeine (50–60 mg doses for mild pain) and strong opioids like fentanyl (microgram doses for severe pain). This classification highlights the divergent therapeutic goals of the two drug classes.
A critical distinction lies in their side effect profiles and safety considerations. Muscle relaxants often cause drowsiness, dizziness, and dry mouth, with centrally acting agents carrying a higher risk of sedation. For example, cyclobenzaprine’s sedative effects necessitate caution in elderly patients or those with hepatic impairment. Opioids, however, are associated with more severe risks, including respiratory depression, constipation, and addiction, particularly with long-term use. The CDC recommends limiting opioid prescriptions to the lowest effective dose (e.g., starting with 5–10 mg of oxycodone every 4–6 hours) and duration (preferably <7 days) to mitigate these risks. This comparison emphasizes the importance of tailoring treatment to the patient’s condition and risk profile.
Clinically, the choice between a muscle relaxant and an opioid depends on the nature of the pain and underlying pathology. Muscle relaxants are ideal for musculoskeletal pain with spasms, such as acute lower back strain, where reducing muscle tension is the primary goal. Opioids are reserved for severe nociceptive or neuropathic pain unresponsive to other modalities, such as post-surgical pain or cancer-related pain. For example, a patient with a herniated disc may benefit from a short course of tizanidine (2–4 mg every 6–8 hours) combined with physical therapy, whereas a post-operative patient might require hydrocodone (5–10 mg every 4–6 hours) for breakthrough pain. Understanding these distinctions ensures safer and more effective pain management strategies.
In summary, differentiating muscle relaxants from opioids based on their pharmacological properties is essential for precise clinical decision-making. While both classes address pain-related symptoms, their mechanisms, classifications, and risk profiles diverge significantly. Muscle relaxants target muscle spasms through CNS or peripheral actions, whereas opioids modulate pain perception via opioid receptors. By recognizing these differences, healthcare providers can optimize treatment outcomes, minimize adverse effects, and reduce the potential for misuse or dependency. This clarity is particularly crucial in an era where opioid overuse remains a public health concern.
Understanding Muscle Relaxants: Effects, Benefits, and Potential Side Effects
You may want to see also
Explore related products






![]()
Mechanism of Action: How muscle relaxants and opioids affect the nervous system differently
Muscle relaxants and opioids, though both used to manage pain and discomfort, operate through distinct mechanisms within the nervous system. Opioids, such as morphine or oxycodone, primarily target the central nervous system by binding to opioid receptors in the brain and spinal cord. This interaction reduces the perception of pain and can induce feelings of euphoria. For instance, a standard dose of morphine (10–30 mg every 4 hours) directly modulates pain signals, making it a potent analgesic. In contrast, muscle relaxants like cyclobenzaprine or baclofen act on the musculoskeletal system and spinal cord to alleviate muscle spasms and tension. Cyclobenzaprine, typically dosed at 5–10 mg three times daily, works by suppressing nerve signals in the brainstem, reducing muscle hyperactivity without directly altering pain perception.
The differences in their mechanisms highlight their appropriate use cases. Opioids are reserved for acute, severe pain due to their potent effects on the brain’s reward system, which carries a high risk of dependence. Muscle relaxants, however, are better suited for conditions like muscle strains or sprains, where spasms are the primary issue. For example, a patient with lower back pain caused by muscle tightness might benefit from a short course of tizanidine (2–4 mg every 6–8 hours) to relieve spasms without the sedative or addictive properties of opioids. Understanding these distinctions ensures safer prescribing practices, particularly in populations like the elderly, where opioid side effects (e.g., respiratory depression) are more pronounced.
A comparative analysis reveals how these drugs interact with different neural pathways. Opioids activate G-protein-coupled receptors, inhibiting neurotransmitter release and dampening pain signals. Muscle relaxants, on the other hand, often act as central nervous system depressants, enhancing GABAergic activity or reducing nerve excitability. For instance, baclofen mimics GABA, an inhibitory neurotransmitter, to decrease spinal cord neuron activity, effectively calming muscle contractions. This targeted approach minimizes systemic side effects, making muscle relaxants a preferred choice for localized musculoskeletal issues. However, their effectiveness is limited to spasticity and not generalized pain, underscoring the importance of accurate diagnosis.
Practical considerations further differentiate their use. Opioids require careful titration to balance analgesia with risks like tolerance and withdrawal, especially in chronic pain management. Muscle relaxants, while generally safer, can cause drowsiness or dizziness, necessitating caution in patients operating machinery or driving. For example, combining cyclobenzaprine with alcohol amplifies sedation, a critical warning for patients. Additionally, muscle relaxants are often prescribed for short durations (e.g., 2–3 weeks) to avoid dependency, whereas opioids may be tapered over months in chronic cases. Tailoring treatment to the patient’s condition and risk profile ensures optimal outcomes while minimizing adverse effects.
In summary, while both muscle relaxants and opioids address pain-related symptoms, their mechanisms of action diverge significantly. Opioids modulate pain perception centrally, offering powerful relief but with substantial risks, whereas muscle relaxants target muscle hyperactivity directly, providing localized relief with fewer systemic concerns. Clinicians must consider these differences when selecting treatments, factoring in the patient’s condition, age, and potential for side effects. For instance, a 65-year-old with acute muscle spasms might benefit from methocarbamol (500–1500 mg up to 4 times daily) over opioids, given its lower risk profile. This nuanced approach ensures effective symptom management while prioritizing patient safety.
Understanding Muscle Relaxer Costs: What You Need to Know
You may want to see also
Explore related products






![]()
Medical Uses: Comparing therapeutic applications of muscle relaxants versus opioids in pain management
Muscle relaxants and opioids serve distinct roles in pain management, yet their applications often overlap, leading to confusion about their therapeutic uses. Muscle relaxants, such as cyclobenzaprine and tizanidine, primarily target musculoskeletal pain by reducing muscle spasms and tension. They are commonly prescribed for conditions like acute lower back pain, where muscle stiffness exacerbates discomfort. Opioids, on the other hand, act on the central nervous system to alleviate severe pain, making them suitable for post-surgical recovery or chronic pain conditions like cancer-related pain. While both classes aim to relieve pain, their mechanisms and indications differ significantly.
Consider a patient with acute lower back pain caused by muscle strain. A muscle relaxant like cyclobenzaprine (10–30 mg daily) may be prescribed to ease spasms, allowing for improved mobility and reduced pain. Opioids, such as hydrocodone, might be considered if the pain is severe and unresponsive to other measures, but their use is typically short-term due to risks of dependence and side effects like drowsiness and constipation. For older adults or patients with renal impairment, dosages of both muscle relaxants and opioids must be adjusted to avoid adverse effects, highlighting the need for tailored treatment plans.
In contrast, opioids are often the go-to option for nociceptive pain that originates from tissue damage, such as postoperative pain or bone fractures. For instance, morphine (5–15 mg every 4 hours) is frequently administered in hospital settings to manage acute, severe pain. Muscle relaxants are less effective in these scenarios because they do not address the underlying cause of pain but rather its muscular symptoms. However, combining muscle relaxants with opioids can sometimes enhance pain relief, particularly in cases where muscle spasms contribute to overall discomfort, though this approach requires careful monitoring to avoid drug interactions.
A critical distinction lies in the side effect profiles and long-term implications of these medications. Opioids carry a high risk of addiction, respiratory depression, and tolerance, limiting their use to short-term or end-of-life care. Muscle relaxants, while generally safer for prolonged use, can cause dizziness, fatigue, and liver toxicity, particularly with drugs like methocarbamol. Patients should be educated on these risks and advised to avoid activities requiring alertness, such as driving, while on these medications. Additionally, muscle relaxants are often preferred for musculoskeletal conditions due to their lower potential for misuse compared to opioids.
In practice, the choice between muscle relaxants and opioids hinges on the pain’s origin, severity, and patient-specific factors. For acute musculoskeletal pain, muscle relaxants offer targeted relief with fewer systemic risks. Opioids remain indispensable for severe, acute pain but should be reserved for cases where alternatives are insufficient. Clinicians must weigh the benefits against risks, considering patient history, age, and comorbidities. Ultimately, both classes have unique roles in pain management, and their use should be guided by evidence-based practices and individualized care.
Cortisone and Muscle Relaxation: Unraveling the Truth Behind the Myth
You may want to see also
Explore related products






![]()
Side Effects and Risks: Contrasting potential adverse effects and addiction risks between the two
Muscle relaxants and opioids, though both prescribed for pain management, diverge significantly in their side effects and addiction risks. Opioids, such as oxycodone or hydrocodone, are known for their potent analgesic properties but carry a high risk of dependence, respiratory depression, and fatal overdose, especially at doses exceeding 90 morphine milligram equivalents (MME) daily. Muscle relaxants, like cyclobenzaprine or tizanidine, primarily target muscle spasms and are less likely to cause addiction, though they can induce drowsiness, dizziness, and impaired coordination, particularly in elderly patients or when combined with alcohol.
Consider the practical implications of these differences. For instance, a 60-year-old patient with chronic back pain might be prescribed tizanidine (4 mg, three times daily) to alleviate muscle spasms. While this regimen minimizes addiction risk, the patient must be cautioned against driving or operating machinery due to potential sedation. In contrast, an opioid prescription for the same condition would necessitate frequent monitoring for signs of tolerance or misuse, such as escalating dosage requests or mood changes. The choice between the two hinges on balancing efficacy with safety, particularly in vulnerable populations like the elderly or those with a history of substance use disorder.
From a persuasive standpoint, the addiction risk of opioids far outweighs their benefits in many cases, especially for long-term use. The CDC reports that even short-term opioid use (less than 8 days) can lead to long-term dependence in 6% of patients. Muscle relaxants, while not without risks, offer a safer alternative for musculoskeletal conditions, provided they are used judiciously. For example, combining tizanidine with a liver-metabolized medication like amitriptyline can cause dangerously low blood pressure, underscoring the need for careful drug interaction assessments.
A comparative analysis reveals that while both classes can cause central nervous system depression, opioids pose a more immediate threat due to their respiratory effects. A single high dose of an opioid can suppress breathing to lethal levels, whereas muscle relaxants typically require chronic misuse or overdose to reach life-threatening toxicity. However, muscle relaxants’ side effects, such as dry mouth or blurred vision, can significantly impair quality of life, particularly in patients requiring prolonged treatment. Tailoring the choice to the patient’s specific condition and risk profile is critical.
In conclusion, while neither muscle relaxants nor opioids are without risks, their adverse effect profiles and addiction potentials differ markedly. Opioids demand stringent monitoring and are best reserved for acute, severe pain, whereas muscle relaxants offer a lower-risk option for muscle-related conditions, albeit with their own set of precautions. Clinicians and patients must weigh these factors carefully, prioritizing safety without compromising pain relief.
Does GABA Relax Muscles? Unlocking the Science Behind Muscle Relaxation
You may want to see also
Explore related products






![]()
Drug Interactions: Key differences in how muscle relaxants and opioids interact with other medications
Muscle relaxants and opioids, though both used to manage pain, interact with other medications in distinct ways, often leading to different risks and outcomes. Understanding these differences is crucial for safe and effective treatment, especially when patients are on multiple therapies. For instance, opioids like oxycodone and hydrocodone are metabolized primarily by the liver’s CYP450 enzyme system, particularly CYP3A4. This makes them prone to interactions with medications that inhibit or induce this enzyme, such as certain antifungals (e.g., ketoconazole) or antiretrovirals (e.g., ritonavir). Such interactions can elevate opioid levels, increasing the risk of respiratory depression or sedation. In contrast, muscle relaxants like cyclobenzaprine or tizanidine have varying metabolic pathways; cyclobenzaprine is metabolized by CYP3A4, while tizanidine is primarily eliminated unchanged in the urine. This means cyclobenzaprine shares some interaction risks with opioids, but tizanidine’s interactions are more limited to drugs affecting renal function, such as diuretics or NSAIDs.
Consider a patient on both an opioid and a muscle relaxant, such as oxycodone and tizanidine, for chronic back pain. Adding an SSRI antidepressant like fluoxetine could significantly complicate the picture. Fluoxetine inhibits CYP1A2, the enzyme responsible for metabolizing tizanidine, potentially leading to dangerously high levels of the muscle relaxant and symptoms like severe hypotension or sedation. Meanwhile, fluoxetine’s impact on opioids is minimal, as they are primarily metabolized by CYP3A4. This example highlights how the interaction profiles of muscle relaxants and opioids diverge, requiring careful consideration of each medication’s unique metabolic pathways.
From a practical standpoint, healthcare providers must prioritize medication reconciliation when prescribing either class. For opioids, monitoring for CYP3A4 inhibitors or inducers is essential. For example, grapefruit juice, a known CYP3A4 inhibitor, can increase oxycodone levels, necessitating patient education to avoid it. Muscle relaxants, particularly those like tizanidine, require attention to renal function and medications affecting it. Patients over 65 or those with pre-existing kidney issues may need dosage adjustments to avoid accumulation. Additionally, combining opioids and muscle relaxants, such as hydrocodone and cyclobenzaprine, can potentiate central nervous system depression, warranting lower starting doses and close monitoring, especially in older adults or those with hepatic impairment.
The takeaway is clear: while both muscle relaxants and opioids are used for pain management, their interaction profiles differ markedly. Opioids’ reliance on CYP3A4 metabolism makes them susceptible to a broad range of drug interactions, whereas muscle relaxants’ varied pathways create more specific but equally critical risks. Clinicians must tailor prescriptions and monitoring strategies to these differences, ensuring patient safety without compromising pain relief. For patients, understanding these nuances can empower them to ask informed questions and adhere to recommendations, such as avoiding certain foods or medications. Ultimately, recognizing these key differences is not just academic—it’s a practical necessity for optimizing therapy and minimizing harm.
Is Weed a Muscle Relaxant? Exploring Cannabis and Its Effects
You may want to see also
Frequently asked questions
No, muscle relaxants are not opioids. They are a separate class of medications used to relieve muscle spasms and pain, whereas opioids are primarily used for pain relief and act on the central nervous system.
Some muscle relaxants may cause drowsiness or sedation, but they do not produce the euphoria or addiction potential associated with opioids. Their mechanisms of action are distinct from opioids.
No, muscle relaxants are not typically used to treat opioid withdrawal. Medications like methadone, buprenorphine, or clonidine are more commonly used for managing opioid withdrawal symptoms.
Combining muscle relaxants and opioids can increase the risk of side effects such as drowsiness, respiratory depression, and impaired coordination. It’s important to consult a healthcare provider before using them together.