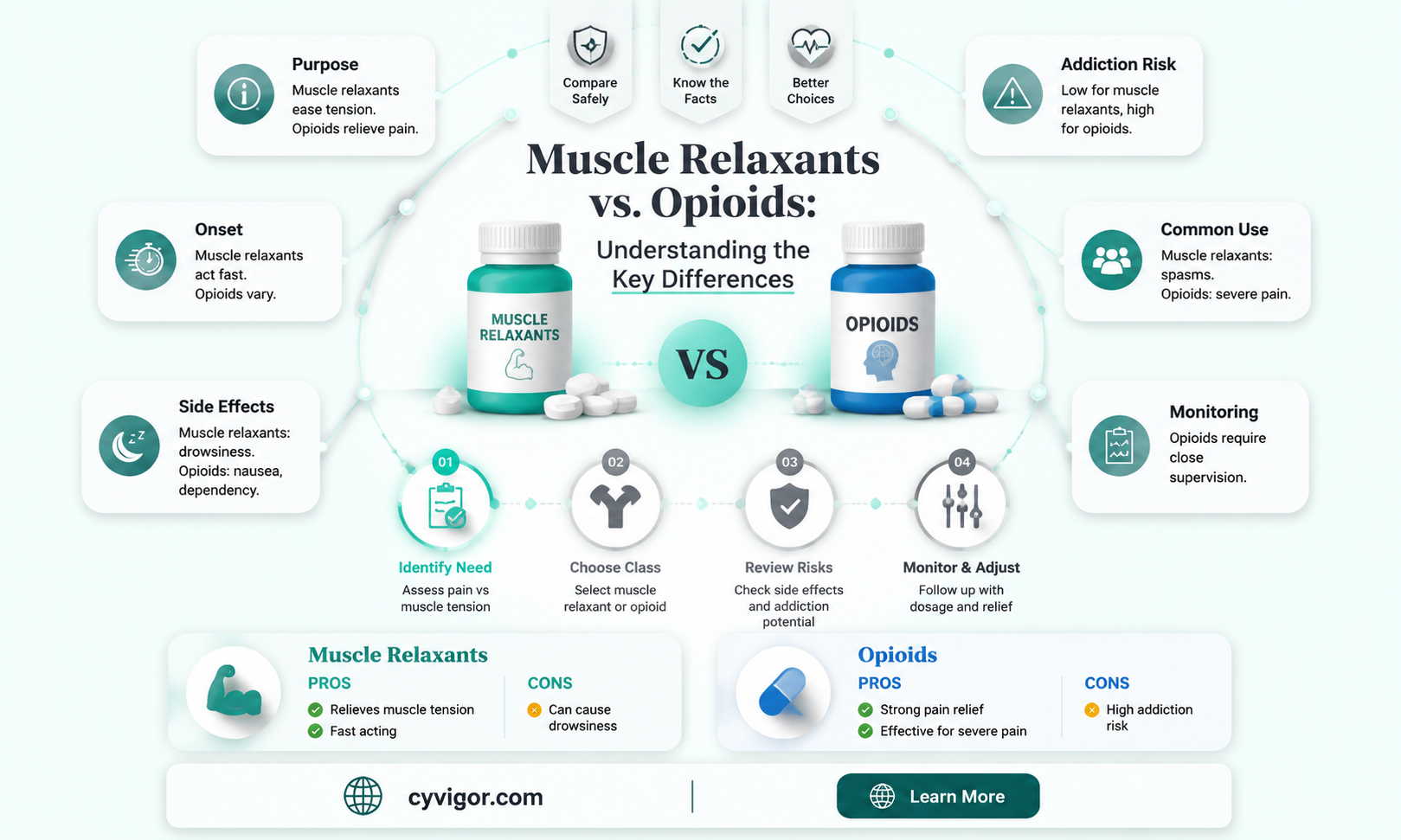
Muscle relaxants and opioids are both medications used to manage pain, but they belong to distinct drug classes and function through different mechanisms. While opioids, such as morphine and oxycodone, primarily target the central nervous system to alleviate pain and produce euphoria, muscle relaxants like cyclobenzaprine and baclofen work by reducing muscle spasms and tension, often without the same level of central nervous system effects. Despite their differences, there is sometimes confusion about whether muscle relaxants are opioids, as both can be prescribed for pain relief. However, muscle relaxants are not classified as opioids, and they do not carry the same risks of addiction, respiratory depression, or tolerance associated with opioid use. Understanding these distinctions is crucial for patients and healthcare providers to ensure appropriate and safe treatment for musculoskeletal conditions.
| Characteristics | Values |
|---|---|
| Classification | Muscle relaxants are not classified as opioids. |
| Mechanism of Action | Act on the central nervous system (CNS) or neuromuscular junction, not on opioid receptors. |
| Primary Use | Treat muscle spasms, pain, and stiffness; opioids primarily treat pain. |
| Addiction Potential | Generally lower risk of addiction compared to opioids. |
| Side Effects | Drowsiness, dizziness, dry mouth (muscle relaxants); respiratory depression, constipation (opioids). |
| Examples | Cyclobenzaprine, Baclofen, Tizanidine (muscle relaxants); Morphine, Oxycodone (opioids). |
| Withdrawal Symptoms | Mild withdrawal possible (muscle relaxants); severe withdrawal (opioids). |
| Overdose Risk | Lower overdose risk (muscle relaxants); high overdose risk (opioids). |
| Drug Interactions | May interact with CNS depressants; opioids interact with other opioids and depressants. |
| Legal Status | Typically prescription-only; opioids are highly regulated due to misuse potential. |
Explore related products






What You'll Learn
- Definition and Classification: Differentiating muscle relaxants and opioids based on their pharmacological properties
- Mechanism of Action: How muscle relaxants and opioids affect the nervous system differently
- Medical Uses: Comparing the therapeutic applications of muscle relaxants versus opioids
- Side Effects and Risks: Contrasting the potential adverse effects of both drug classes
- Addiction Potential: Evaluating the risk of dependence with muscle relaxants and opioids
![]()
Definition and Classification: Differentiating muscle relaxants and opioids based on their pharmacological properties
Muscle relaxants and opioids are often confused due to their overlapping use in pain management, but their pharmacological properties and mechanisms of action are distinct. Muscle relaxants primarily target the central nervous system (CNS) or neuromuscular junction to reduce muscle spasms and tension, while opioids act on the CNS to alter pain perception and provide analgesia. This fundamental difference in action necessitates clear classification to ensure appropriate prescribing and patient safety.
Pharmacological Classification and Mechanisms
Muscle relaxants are broadly categorized into two groups: antispasmodics and antispastics. Antispasmodics, such as cyclobenzaprine and tizanidine, act on the CNS to inhibit nerve impulses that cause muscle spasms. For instance, cyclobenzaprine has a half-life of 18 hours and is typically dosed at 5–10 mg three times daily for adults. Antispastics, like baclofen, mimic GABA, a neurotransmitter that reduces muscle tone, and are often prescribed at 5–20 mg three times daily. In contrast, opioids, including morphine, oxycodone, and fentanyl, bind to mu-opioid receptors in the brain and spinal cord, modulating pain signals. Morphine, for example, has a half-life of 2–3 hours and is administered at 5–10 mg every 4 hours for acute pain. This receptor-specific action distinguishes opioids from muscle relaxants, which do not interact with opioid pathways.
Clinical Applications and Dosage Considerations
Understanding these pharmacological differences is critical for clinical practice. Muscle relaxants are primarily used for musculoskeletal conditions like acute back pain or spasticity from multiple sclerosis, while opioids are reserved for moderate to severe pain, such as post-surgical or cancer-related pain. For instance, tizanidine’s alpha-2 adrenergic agonism makes it effective for muscle spasms but requires careful dosing (2–4 mg every 6–8 hours) to avoid hypotension. Opioids, however, carry a higher risk of dependence and side effects like respiratory depression, necessitating lower starting doses in elderly patients or those with renal impairment. A 2020 study highlighted that misclassification of these drugs led to 15% of patients receiving inappropriate prescriptions, underscoring the need for precise differentiation.
Practical Tips for Differentiation
To avoid confusion, healthcare providers should focus on the intended therapeutic effect. If the goal is to alleviate muscle spasms or stiffness, a muscle relaxant is appropriate. For pain relief, particularly when non-opioid options are insufficient, opioids may be considered. Patients should be educated on the differences: muscle relaxants may cause drowsiness but do not induce euphoria, while opioids carry a higher risk of addiction. For example, a patient with acute lower back strain might benefit from a short course of cyclobenzaprine (10 mg at bedtime) rather than hydrocodone, which could lead to unnecessary opioid exposure.
Takeaway: Precision in Prescribing
Differentiating muscle relaxants and opioids based on their pharmacological properties ensures safer and more effective treatment. While both classes address pain-related conditions, their mechanisms, risks, and applications are distinct. Clinicians should prioritize patient history, condition severity, and potential side effects when selecting between these medications. For instance, a 65-year-old with chronic back pain and a history of falls may tolerate baclofen better than an opioid due to its lower risk of sedation and cognitive impairment. By adhering to these principles, healthcare providers can optimize outcomes and minimize adverse events.
Exploring PGE2's Role in Relaxing Circular Muscle: Mechanisms and Insights
You may want to see also
Explore related products






![]()
Mechanism of Action: How muscle relaxants and opioids affect the nervous system differently
Muscle relaxants and opioids, though both used to manage pain and discomfort, operate through distinct mechanisms within the nervous system. Opioids, such as morphine and oxycodone, primarily target the central nervous system (CNS) by binding to opioid receptors in the brain and spinal cord. This interaction reduces the perception of pain and can induce euphoria, making them highly effective for acute and chronic pain management. However, their action on the CNS also increases the risk of dependence, respiratory depression, and other side effects, particularly at higher dosages (e.g., morphine doses exceeding 30 mg for adults).
In contrast, muscle relaxants like cyclobenzaprine and baclofen act directly on skeletal muscles or the CNS to alleviate muscle spasms and stiffness. For instance, cyclobenzaprine works by suppressing nerve signals in the brainstem, reducing muscle hyperactivity without directly affecting opioid receptors. Baclofen, on the other hand, mimics GABA, an inhibitory neurotransmitter, to decrease muscle tone. These drugs are typically prescribed for conditions like lower back pain or multiple sclerosis, with dosages ranging from 5 to 30 mg daily for cyclobenzaprine, depending on patient tolerance and age (lower doses for elderly patients to avoid sedation).
The key difference lies in their site of action and intended effect. Opioids modulate pain perception globally, while muscle relaxants target specific pathways related to muscle function. For example, opioids may be prescribed post-surgery for severe pain (e.g., 10 mg of oxycodone every 4–6 hours), whereas muscle relaxants are used for localized muscle spasms (e.g., 10 mg of baclofen three times daily). Combining these drugs requires caution, as both can cause CNS depression, increasing the risk of dizziness or respiratory issues, especially in patients over 65 or with renal impairment.
Practical considerations highlight the importance of tailoring treatment to the underlying condition. Opioids are reserved for intense pain unresponsive to other therapies, while muscle relaxants are preferred for musculoskeletal issues. Patients should avoid alcohol and sedatives when using either class, as these potentiate CNS effects. For instance, a 45-year-old with acute back spasms might start with 5 mg of cyclobenzaprine at bedtime to minimize daytime drowsiness, whereas a post-operative patient might receive 5 mg of oxycodone every 6 hours for breakthrough pain. Understanding these mechanisms ensures safer, more effective treatment.
How Albuterol Relieves Muscle Tension: A Comprehensive Guide
You may want to see also
Explore related products






![]()
Medical Uses: Comparing the therapeutic applications of muscle relaxants versus opioids
Muscle relaxants and opioids, though both used in pain management, serve distinct therapeutic purposes and are not interchangeable. Muscle relaxants, such as cyclobenzaprine and tizanidine, primarily target skeletal muscle spasms and stiffness, often associated with conditions like lower back pain or multiple sclerosis. They work by acting on the central nervous system to reduce muscle tone without directly addressing pain perception. Opioids, on the other hand, such as morphine or oxycodone, are potent analgesics that bind to opioid receptors in the brain and spinal cord to alleviate moderate to severe pain, often from surgery, trauma, or chronic conditions like cancer. While muscle relaxants may have mild analgesic effects due to reduced muscle tension, their primary mechanism differs fundamentally from opioids.
Consider a patient with acute lower back pain caused by muscle spasms. A physician might prescribe a muscle relaxant like cyclobenzaprine (10–30 mg/day) to alleviate muscle tension and improve mobility. This treatment is particularly effective when the pain is musculoskeletal in origin. However, if the pain is neuropathic or severe, an opioid like hydrocodone (5–10 mg every 4–6 hours) might be added to manage the pain component directly. The key distinction lies in their application: muscle relaxants address the source of muscle-related pain, while opioids provide systemic pain relief. This complementary approach highlights their non-overlapping roles in clinical practice.
From a practical standpoint, the choice between muscle relaxants and opioids depends on the pain’s etiology and severity. For instance, postoperative patients with significant pain might receive opioids for immediate relief, while those with chronic musculoskeletal conditions may benefit more from long-term muscle relaxant therapy. It’s crucial to note that muscle relaxants are generally not recommended for elderly patients due to risks of sedation and falls, whereas opioids, despite their efficacy, carry a high risk of dependence and respiratory depression. Dosage adjustments and careful monitoring are essential for both classes, but the therapeutic goals and patient profiles differ markedly.
A persuasive argument for the judicious use of these medications lies in their side effect profiles and long-term implications. Opioids, while effective for severe pain, are associated with tolerance, addiction, and overdose, making them a last-resort option in many cases. Muscle relaxants, though safer in terms of addiction potential, can cause drowsiness, dizziness, and impaired coordination, limiting their use in active individuals or those operating machinery. Clinicians must weigh these factors, tailoring treatment to the patient’s specific needs and condition. For example, a young athlete with a muscle strain might benefit from a short course of tizanidine (2–4 mg every 6–8 hours) to restore function without the risks associated with opioids.
In conclusion, while both muscle relaxants and opioids play vital roles in pain management, their therapeutic applications are distinct and non-interchangeable. Muscle relaxants target muscle spasms and stiffness, offering relief for musculoskeletal conditions, whereas opioids provide systemic pain relief for severe or neuropathic pain. Understanding these differences allows for more precise and effective treatment strategies, minimizing risks and maximizing patient outcomes. Always consult a healthcare provider for personalized guidance, as individual responses to these medications can vary widely.
Ejaculation and Muscle Relaxation: Unraveling the Science Behind the Release
You may want to see also
Explore related products






![]()
Side Effects and Risks: Contrasting the potential adverse effects of both drug classes
Muscle relaxants and opioids, though sometimes prescribed for similar conditions like pain and muscle spasms, carry distinct side effect profiles that patients and healthcare providers must carefully consider. Opioids, such as oxycodone and hydrocodone, are primarily known for their potent analgesic effects but come with a high risk of dependence, respiratory depression, and constipation. For instance, even short-term use of opioids can lead to tolerance, requiring higher doses to achieve the same effect, while long-term use increases the risk of addiction, particularly in individuals with a history of substance abuse. In contrast, muscle relaxants like cyclobenzaprine and baclofen are less likely to cause dependence but can induce drowsiness, dizziness, and impaired coordination, making activities like driving or operating machinery hazardous.
Consider the practical implications of these side effects in daily life. Opioids often require careful monitoring due to their potential for life-threatening respiratory depression, especially when combined with alcohol or other central nervous system depressants. For example, a patient prescribed oxycodone should avoid alcohol entirely and be aware of signs of slowed breathing, such as shallow breaths or prolonged pauses between breaths. Muscle relaxants, on the other hand, may necessitate adjustments to daily routines. A patient taking tizanidine, which can cause significant sedation, might need to schedule doses for bedtime to minimize disruption during the day. Both drug classes require tailored strategies to mitigate risks, but the nature of those strategies differs markedly.
From a comparative standpoint, the age-related risks of these drugs further highlight their contrasting profiles. Opioids pose a heightened danger in older adults due to age-related changes in metabolism and increased sensitivity to their effects. For instance, a 70-year-old patient prescribed morphine may experience more pronounced confusion, falls, or respiratory issues compared to a younger individual. Muscle relaxants, however, can be problematic across all age groups but are particularly risky in younger patients who may underestimate their sedative effects. A 25-year-old taking cyclobenzaprine might mistakenly believe they can drive safely after a dose, only to experience delayed onset drowsiness that impairs reaction time.
To navigate these risks effectively, patients and providers should adopt a proactive approach. For opioids, starting with the lowest effective dose (e.g., 5 mg of oxycodone every 4–6 hours) and regularly reassessing pain levels can help minimize adverse effects. Combining opioids with non-pharmacological interventions, such as physical therapy, can also reduce reliance on the drug. For muscle relaxants, patients should be educated about the delayed onset of action (e.g., baclofen may take 1–2 hours to work) and the importance of avoiding abrupt discontinuation, which can cause rebound spasms. Practical tips, like keeping a symptom diary to track side effects, can empower patients to communicate effectively with their healthcare team.
Ultimately, the choice between muscle relaxants and opioids hinges on balancing efficacy with risk tolerance. While opioids offer powerful pain relief, their potential for addiction and systemic harm necessitates cautious prescribing, particularly in vulnerable populations. Muscle relaxants, though less habit-forming, demand vigilance regarding sedation and coordination issues. By understanding these distinctions, patients and providers can make informed decisions that prioritize safety without compromising therapeutic goals.
Effective Techniques to Relax and Release Tight Scalene Muscles
You may want to see also
Explore related products






![]()
Addiction Potential: Evaluating the risk of dependence with muscle relaxants and opioids
Muscle relaxants and opioids, though both prescribed for pain management, differ significantly in their mechanisms and addiction potential. Opioids, such as oxycodone and hydrocodone, act on the central nervous system to alleviate pain and induce euphoria, making them highly prone to misuse and dependence. Muscle relaxants, like cyclobenzaprine and baclofen, primarily target muscle spasms and tension, with a lower risk of euphoria. However, prolonged use of either class can lead to physical dependence, underscoring the need for careful evaluation of their addiction profiles.
To assess addiction potential, consider the pharmacological properties and intended use. Opioids bind to opioid receptors in the brain, altering pain perception and releasing dopamine, which reinforces repeated use. Muscle relaxants, on the other hand, work by depressing the central nervous system or directly affecting muscle fibers, with minimal impact on dopamine pathways. For instance, a typical opioid prescription might start at 5–10 mg of oxycodone every 4–6 hours, while cyclobenzaprine is often dosed at 5–10 mg three times daily. Despite lower euphoric effects, muscle relaxants can still lead to psychological dependence, particularly in individuals with a history of substance abuse.
Practical tips for minimizing dependence risk include adhering strictly to prescribed dosages and durations. For opioids, tapering under medical supervision is critical to avoid withdrawal symptoms, which can include anxiety, nausea, and muscle aches. Muscle relaxants, while less addictive, should also be discontinued gradually, especially after long-term use. Patients over 65 or those with liver or kidney impairment require lower doses due to slower metabolism, reducing the risk of accumulation and dependence.
Comparatively, opioids pose a higher addiction risk due to their direct influence on reward pathways, whereas muscle relaxants are more likely to cause tolerance or physical dependence without the same level of euphoria-driven misuse. For example, a study found that 21–29% of patients prescribed opioids for chronic pain developed opioid use disorder, compared to 5–10% of muscle relaxant users experiencing withdrawal symptoms upon abrupt cessation. This highlights the importance of selecting the appropriate medication based on pain severity, patient history, and risk factors.
In conclusion, while muscle relaxants are not opioids, both classes require vigilant monitoring to mitigate dependence. Opioids demand stricter controls due to their high addiction potential, while muscle relaxants necessitate awareness of tolerance and withdrawal risks. Healthcare providers should educate patients on these distinctions, emphasizing the importance of short-term use and alternative therapies, such as physical therapy or cognitive-behavioral interventions, to reduce reliance on pharmacological solutions.
Alcohol and Muscle Relaxation: Fact or Fiction? Unveiling the Truth
You may want to see also
Frequently asked questions
No, muscle relaxants are not opioids. They are a separate class of medications used to relieve muscle spasms and pain, whereas opioids are primarily used for pain relief and work by binding to opioid receptors in the brain.
While muscle relaxants can cause drowsiness, dizziness, or sedation, they do not produce the euphoria or addiction potential associated with opioids. Their side effects are generally milder and unrelated to opioid mechanisms.
Yes, muscle relaxants are sometimes prescribed as alternatives to opioids for certain types of pain, particularly musculoskeletal pain or muscle spasms. However, they are not interchangeable and are used based on the specific condition being treated.