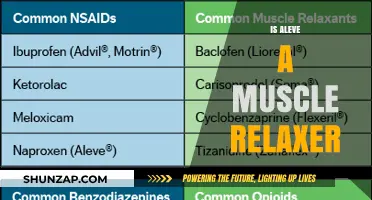
Muscle relaxers and anti-inflammatory medications are often discussed in the context of pain management, but they serve distinct purposes. Muscle relaxers primarily target muscle spasms and tension by acting on the central nervous system, helping to alleviate stiffness and discomfort associated with conditions like back pain or injuries. On the other hand, anti-inflammatory drugs, such as NSAIDs, reduce inflammation, swelling, and pain by inhibiting certain enzymes in the body. While both types of medications can relieve pain, they address different underlying issues, and the question of whether a muscle relaxer is also an anti-inflammatory arises from their overlapping use in treating musculoskeletal conditions. Understanding their mechanisms and differences is crucial for effective and safe treatment.
| Characteristics | Values |
|---|---|
| Primary Function | Muscle relaxers primarily target muscle spasms and pain by acting on the central nervous system or directly on muscles. |
| Anti-Inflammatory Properties | Most muscle relaxers do not have inherent anti-inflammatory effects. They are not designed to reduce inflammation. |
| Mechanism of Action | Muscle relaxers work by inhibiting nerve signals to muscles (e.g., cyclobenzaprine, tizanidine) or directly relaxing muscle fibers (e.g., baclofen, dantrolene). |
| Common Examples | Cyclobenzaprine, tizanidine, baclofen, methocarbamol, carisoprodol. |
| Anti-Inflammatory Medications | NSAIDs (e.g., ibuprofen, naproxen), corticosteroids, and other anti-inflammatory drugs are used to reduce inflammation. |
| Combined Therapy | Muscle relaxers may be prescribed alongside anti-inflammatory medications for conditions involving both muscle spasms and inflammation (e.g., acute back pain). |
| Side Effects | Muscle relaxers may cause drowsiness, dizziness, or dry mouth, while anti-inflammatory drugs may cause stomach irritation or increased bleeding risk. |
| Usage | Muscle relaxers are used for acute musculoskeletal conditions, whereas anti-inflammatory drugs are used for inflammatory conditions like arthritis. |
| Conclusion | Muscle relaxers are not anti-inflammatory; they serve distinct purposes in managing pain and discomfort. |
Explore related products






What You'll Learn
- Mechanism of Action: How muscle relaxers differ from anti-inflammatory drugs in targeting pain
- Common Uses: Conditions treated by muscle relaxers vs. anti-inflammatory medications
- Side Effects: Comparing side effects of muscle relaxers and anti-inflammatory drugs
- Drug Interactions: Potential risks when combining muscle relaxers with anti-inflammatory meds
- Effectiveness: Which works better for muscle pain and inflammation: relaxers or anti-inflammatories
![]()
Mechanism of Action: How muscle relaxers differ from anti-inflammatory drugs in targeting pain
Muscle relaxers and anti-inflammatory drugs both aim to alleviate pain, but they operate through distinct mechanisms, targeting different root causes of discomfort. Muscle relaxers, such as cyclobenzaprine and tizanidine, act on the central nervous system to reduce muscle spasms and tension. They work by inhibiting nerve signals in the brain and spinal cord, effectively calming overactive muscles. This makes them particularly effective for acute musculoskeletal conditions like lower back pain or injury-induced spasms. In contrast, anti-inflammatory drugs, including NSAIDs (e.g., ibuprofen) and corticosteroids, focus on reducing inflammation at the site of pain. They block enzymes like COX-1 and COX-2, which are responsible for producing prostaglandins—chemicals that promote inflammation and sensitize nerves to pain. This dual action not only decreases swelling but also lowers pain perception.
Consider a scenario where a patient experiences chronic neck pain due to repetitive strain. A muscle relaxer might be prescribed to alleviate the spasms causing stiffness, often at doses like 5–10 mg of cyclobenzaprine up to three times daily. However, if the pain is primarily driven by inflammation, an NSAID like naproxen (250–500 mg twice daily) would be more appropriate. The choice depends on the underlying cause: muscle relaxers address neurological hyperactivity, while anti-inflammatory drugs target tissue inflammation. Combining both types of medication can sometimes provide synergistic relief, but this requires careful monitoring to avoid side effects like drowsiness or gastrointestinal bleeding.
From a practical standpoint, understanding these differences helps patients and providers tailor treatment effectively. For instance, muscle relaxers are often short-term solutions due to their sedative effects, making them unsuitable for prolonged use in older adults or those with cognitive impairments. Anti-inflammatory drugs, while generally safer for long-term use, carry risks like kidney damage or cardiovascular issues, especially at high doses (e.g., exceeding 2400 mg of ibuprofen daily). Patients should also be aware of contraindications: muscle relaxers may interact with alcohol or antidepressants, while NSAIDs should be avoided in those with a history of ulcers or bleeding disorders.
A comparative analysis reveals that while both drug classes target pain, their pathways are fundamentally different. Muscle relaxers act systemically to reduce muscle activity, whereas anti-inflammatory drugs work locally to suppress inflammation and pain signals. This distinction underscores the importance of accurate diagnosis—misidentifying the source of pain can lead to ineffective treatment. For example, prescribing a muscle relaxer for arthritis pain (primarily inflammatory) would yield limited results, whereas an NSAID might fail to relieve pain caused by muscle spasms.
In conclusion, the mechanism of action of muscle relaxers and anti-inflammatory drugs highlights their complementary yet distinct roles in pain management. Muscle relaxers address neurological causes of muscle tension, while anti-inflammatory drugs combat inflammation-driven pain. By recognizing these differences, healthcare providers can prescribe more targeted therapies, improving outcomes and minimizing risks. Patients, too, can advocate for themselves by understanding whether their pain stems from muscle spasms or inflammation, ensuring they receive the most appropriate treatment.
When to Take Muscle Relaxers: Timing Your 10mg Dose for Relief
You may want to see also
Explore related products





![]()
Common Uses: Conditions treated by muscle relaxers vs. anti-inflammatory medications
Muscle relaxers and anti-inflammatory medications serve distinct purposes in managing pain and discomfort, targeting different underlying causes. Muscle relaxers, such as cyclobenzaprine (Flexeril) or tizanidine (Zanaflex), primarily address muscle spasms and stiffness by acting on the central nervous system to reduce muscle tension. They are commonly prescribed for conditions like acute lower back pain, neck pain, or injuries involving muscle strains. Anti-inflammatory medications, on the other hand, such as ibuprofen (Advil) or naproxen (Aleve), work by reducing inflammation and pain at the site of injury or irritation. These are often used for conditions like arthritis, tendonitis, or post-surgical swelling. Understanding the specific condition is crucial to determining which medication—or combination—is most effective.
Consider a scenario where a 45-year-old patient experiences chronic lower back pain due to muscle spasms. A muscle relaxer like cyclobenzaprine (10 mg, taken 2-3 times daily) might be prescribed to alleviate the spasms, allowing for better mobility and comfort. However, if the pain is primarily due to inflammation from osteoarthritis, an anti-inflammatory like naproxen (500 mg twice daily) would be more appropriate. For acute injuries, such as a sprained ankle, combining both types of medication under medical supervision could provide comprehensive relief by addressing both muscle tension and inflammation. Always consult a healthcare provider to tailor the treatment to individual needs.
While muscle relaxers and anti-inflammatory medications differ in mechanism, they can sometimes overlap in usage. For instance, fibromyalgia patients may benefit from muscle relaxers to manage widespread muscle pain, but anti-inflammatory drugs might also be used to address coexisting conditions like joint inflammation. Dosage and duration are critical: muscle relaxers are typically prescribed for short-term use (2-3 weeks) due to side effects like drowsiness, while anti-inflammatory medications can be used long-term but require monitoring for gastrointestinal or cardiovascular risks. Practical tips include taking muscle relaxers at bedtime to minimize drowsiness and using anti-inflammatory medications with food to reduce stomach irritation.
A comparative analysis reveals that muscle relaxers are more suited for conditions involving acute muscle spasms or tension, whereas anti-inflammatory medications excel in managing chronic inflammatory disorders. For example, a patient with rheumatoid arthritis would likely benefit more from a long-term anti-inflammatory regimen than a muscle relaxer. However, in cases like whiplash or sports injuries, where both muscle spasms and inflammation are present, a combined approach may be optimal. Age and health status also play a role: older adults or those with kidney issues may require lower doses of anti-inflammatory drugs, while muscle relaxers should be used cautiously in individuals with liver disease. Always prioritize professional guidance to avoid adverse interactions or complications.
In summary, the choice between muscle relaxers and anti-inflammatory medications hinges on the root cause of the condition. Muscle relaxers target spasms and stiffness, making them ideal for acute musculoskeletal issues, while anti-inflammatory drugs address inflammation and are better suited for chronic conditions like arthritis. Combining both under medical supervision can provide synergistic relief in complex cases. Practical considerations, such as dosage, duration, and side effects, are essential for safe and effective treatment. By understanding these distinctions, patients and providers can make informed decisions to optimize pain management and improve quality of life.
Melatonin's Muscle Relaxation Benefits: Fact or Fiction?
You may want to see also
Explore related products






![]()
Side Effects: Comparing side effects of muscle relaxers and anti-inflammatory drugs
Muscle relaxers and anti-inflammatory drugs serve distinct purposes, but their side effects often overlap, creating a complex landscape for patients and healthcare providers. Muscle relaxers, such as cyclobenzaprine and tizanidine, primarily target muscle spasms by acting on the central nervous system. Anti-inflammatory drugs, including NSAIDs like ibuprofen and naproxen, reduce inflammation and pain by inhibiting prostaglandin production. While both classes can alleviate discomfort, their side effect profiles differ significantly, necessitating careful consideration when prescribing or using them.
Central Nervous System Impacts: Sedation vs. Gastrointestinal Risks
Muscle relaxers are notorious for their sedative effects, often causing drowsiness, dizziness, and impaired coordination. For instance, cyclobenzaprine can make driving or operating machinery hazardous, particularly at higher doses (10–30 mg daily). In contrast, anti-inflammatory NSAIDs rarely cause sedation but pose a higher risk of gastrointestinal issues, such as stomach ulcers or bleeding, especially in older adults or those taking high doses (e.g., 800 mg ibuprofen three times daily). Patients with a history of GI disorders should exercise caution with NSAIDs, while those needing muscle relaxers should plan for potential daytime fatigue.
Cardiovascular and Renal Considerations
Anti-inflammatory drugs, particularly NSAIDs, can elevate blood pressure and strain the kidneys, making them less suitable for individuals with hypertension or renal disease. COX-2 inhibitors like celecoxib carry a lower GI risk but still pose cardiovascular concerns. Muscle relaxers, on the other hand, rarely affect cardiovascular or renal systems directly but may interact with other medications, such as blood thinners, exacerbating side effects. For example, combining tizanidine with fluvoxamine can lead to dangerously low blood pressure.
Practical Tips for Minimizing Side Effects
To mitigate risks, start with the lowest effective dose of either drug. For muscle relaxers, take them at bedtime to reduce daytime sedation. With NSAIDs, pair them with food or a proton pump inhibitor (e.g., omeprazole) to protect the stomach. Always disclose existing conditions and medications to your provider, as age, liver function, and concurrent drug use can amplify side effects. For instance, individuals over 65 may require lower doses of both drug classes due to reduced metabolic efficiency.
Balancing Efficacy and Safety
While muscle relaxers and anti-inflammatory drugs address different aspects of pain and discomfort, their side effects demand tailored approaches. Muscle relaxers are ideal for acute muscle spasms but require vigilance for CNS effects, whereas anti-inflammatory drugs excel in managing chronic inflammation but necessitate monitoring for GI and cardiovascular risks. By understanding these distinctions, patients and providers can make informed decisions, optimizing relief while minimizing adverse outcomes.
Understanding Muscle Relaxers: Shelf Life and Effectiveness Explained
You may want to see also
Explore related products






![]()
Drug Interactions: Potential risks when combining muscle relaxers with anti-inflammatory meds
Muscle relaxers and anti-inflammatory medications are often prescribed together to manage pain and discomfort, but their combined use can lead to significant drug interactions. For instance, cyclobenzaprine (a muscle relaxer) and ibuprofen (an NSAID) are commonly paired for conditions like acute back pain. However, both drugs can cause central nervous system depression, increasing the risk of dizziness, drowsiness, and impaired coordination. Patients over 65 are particularly vulnerable due to age-related changes in drug metabolism, making dosage adjustments critical. Always consult a healthcare provider before combining these medications, especially if you have pre-existing conditions like liver or kidney disease.
Analyzing the pharmacological mechanisms reveals why these interactions occur. Muscle relaxers like tizanidine work by suppressing the central nervous system, while anti-inflammatory drugs like naproxen reduce inflammation by inhibiting COX enzymes. When combined, they can exacerbate side effects such as hypotension (low blood pressure) and gastrointestinal bleeding. For example, tizanidine’s blood pressure-lowering effect can be intensified by NSAIDs, which may reduce renal blood flow. To mitigate risks, start with the lowest effective dose of each medication—tizanidine at 2 mg and naproxen at 250 mg—and monitor for adverse reactions over 24–48 hours.
From a practical standpoint, patients should be aware of specific red flags when combining these drugs. Symptoms like severe fatigue, confusion, or unusual bruising warrant immediate medical attention. For instance, the combination of methocarbamol (a muscle relaxer) and diclofenac (an NSAID) can increase the risk of liver toxicity, particularly in patients with pre-existing hepatic issues. To minimize risks, avoid alcohol, as it amplifies sedation and impairs judgment. Additionally, maintain a medication diary to track doses and side effects, sharing this information with all healthcare providers to ensure coordinated care.
Comparatively, some muscle relaxers pose higher interaction risks than others. Baclofen, for example, has a lower potential for CNS depression compared to cyclobenzaprine but can still interact with NSAIDs to cause dizziness. In contrast, anti-inflammatory drugs like celecoxib (a COX-2 inhibitor) have a reduced risk of gastrointestinal bleeding compared to traditional NSAIDs but may still interact with muscle relaxers to cause renal impairment. When in doubt, opt for short-term use of these combinations and explore alternatives like physical therapy or acetaminophen, which has fewer interactions with muscle relaxers.
In conclusion, while muscle relaxers and anti-inflammatory medications can provide relief when used together, their interaction risks demand caution. Patients should prioritize open communication with healthcare providers, adhere to prescribed dosages, and remain vigilant for adverse effects. For example, if prescribed cyclobenzaprine 10 mg and ibuprofen 800 mg, take them at different times of the day to minimize overlapping side effects. By understanding these dynamics, individuals can safely manage pain while avoiding potential complications.
Valium for Muscle Relaxation: Optimal Duration and Safe Usage Guide
You may want to see also
Explore related products






![]()
Effectiveness: Which works better for muscle pain and inflammation: relaxers or anti-inflammatories?
Muscle relaxers and anti-inflammatory medications target different mechanisms of pain and discomfort, making their effectiveness dependent on the root cause of the symptoms. Muscle relaxers, such as cyclobenzaprine or tizanidine, work by reducing muscle spasms and tension, primarily through central nervous system depression. They are most effective for acute musculoskeletal conditions like lower back strain or neck pain, where muscle tightness is the primary issue. Anti-inflammatories, including NSAIDs (e.g., ibuprofen, naproxen) and corticosteroids, reduce inflammation and associated pain by inhibiting inflammatory pathways. For conditions like arthritis or tendonitis, where inflammation drives pain, anti-inflammatories are typically more effective. Understanding the underlying cause is crucial for choosing the right treatment.
When comparing the two for muscle pain and inflammation, the choice often hinges on the specific condition. For instance, a strained muscle with significant spasm may respond better to a muscle relaxer, especially if the pain is exacerbated by movement. A typical dose of cyclobenzaprine (5–10 mg) taken at bedtime can alleviate spasms and improve sleep, though it may cause drowsiness. In contrast, if the pain is accompanied by swelling and redness—hallmarks of inflammation—an NSAID like ibuprofen (200–400 mg every 4–6 hours) or naproxen (220–440 mg twice daily) may provide more relief. For severe cases, a short course of oral corticosteroids (e.g., prednisone 10–20 mg daily for 5–7 days) can be prescribed, but long-term use should be avoided due to side effects like bone density loss.
Practical considerations also play a role in determining effectiveness. Muscle relaxers are generally not recommended for long-term use due to risks of dependence and side effects like dizziness or fatigue. They are best suited for short-term relief (2–3 weeks) in adults under 65, as older adults may be more sensitive to their sedative effects. Anti-inflammatories, while effective, carry their own risks, such as gastrointestinal bleeding or kidney damage, especially with prolonged use. Patients with a history of ulcers, hypertension, or kidney disease should use NSAIDs cautiously and under medical supervision. Combining both types of medications is sometimes done under a doctor’s guidance, but this approach requires careful monitoring to avoid adverse interactions.
In cases where the cause of pain is unclear, a trial of each medication can help determine the most effective treatment. For example, if a patient with chronic back pain finds no relief from ibuprofen after 7–10 days, a muscle relaxer could be tried next. Conversely, if a muscle relaxer fails to alleviate pain in someone with joint stiffness, an anti-inflammatory might be more appropriate. Physical therapy and lifestyle modifications, such as stretching or applying heat/ice, should complement medication use for optimal results. Ultimately, the choice between muscle relaxers and anti-inflammatories should be tailored to the individual’s symptoms, medical history, and the specific nature of their pain and inflammation.
Muscle Relaxants Shelf Life: How Long Are They Effective After Subscription?
You may want to see also
Frequently asked questions
No, muscle relaxers are not anti-inflammatory medications. They work by reducing muscle spasms and tension, while anti-inflammatory drugs target inflammation in the body.
No, muscle relaxers do not reduce swelling or inflammation. They are designed to alleviate muscle pain and stiffness, not to address inflammatory processes.
Not always. Muscle relaxers are typically used for acute muscle spasms or injuries, while anti-inflammatory drugs are used for conditions involving inflammation, such as arthritis or tendonitis.
Yes, in some cases, a doctor may prescribe both a muscle relaxer and an anti-inflammatory together to address muscle pain and inflammation simultaneously, but this should only be done under medical supervision.
No, muscle relaxers do not have anti-inflammatory properties. They act on the central nervous system or muscles directly to relieve spasms and pain, not on inflammatory pathways.