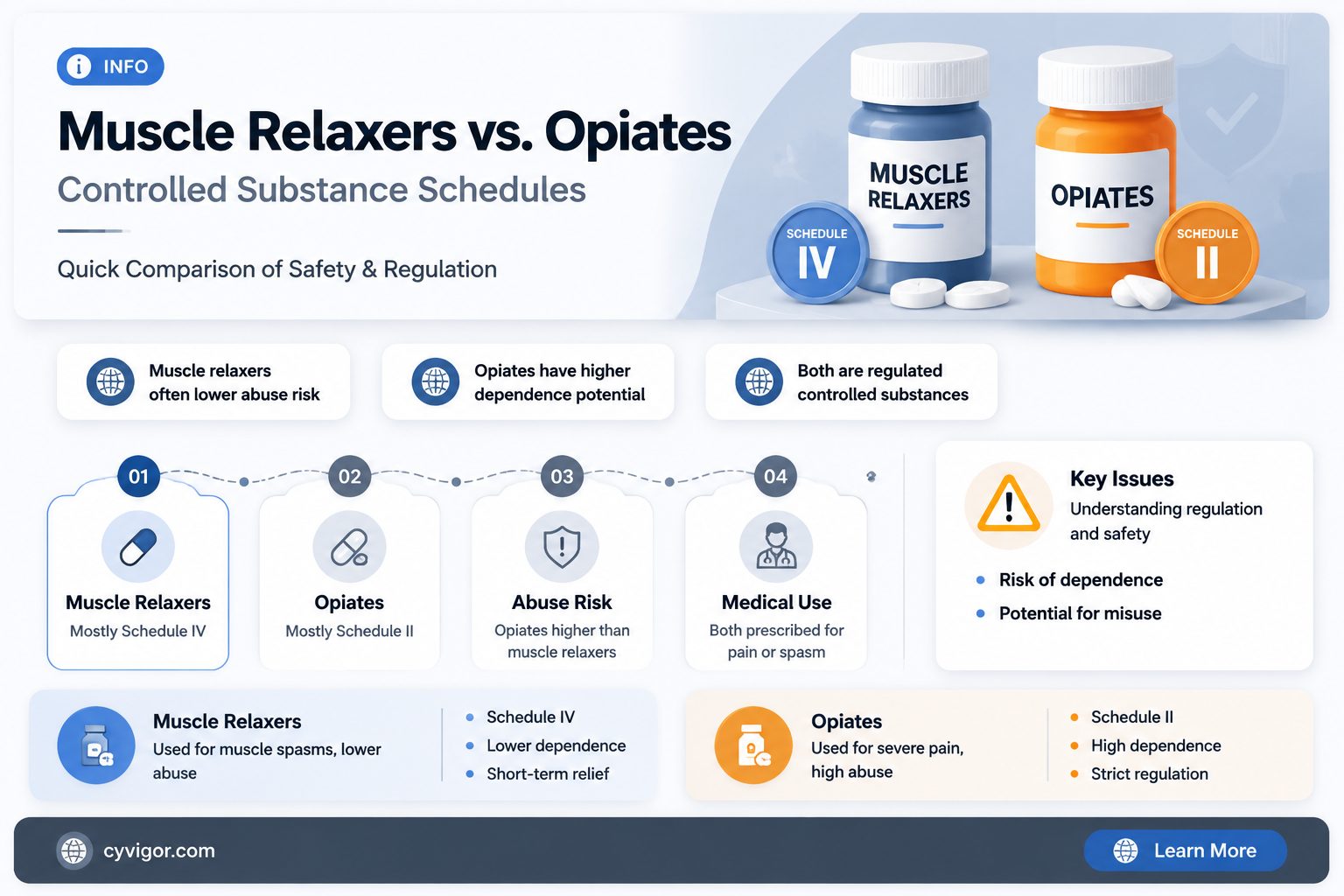
Muscle relaxers and opiates are both prescription medications, but they are classified differently under the Controlled Substances Act (CSA) in the United States. Opiates, such as morphine, oxycodone, and hydrocodone, are typically categorized as Schedule II drugs due to their high potential for abuse and severe dependence. In contrast, muscle relaxers like cyclobenzaprine and tizanidine are generally classified as Schedule IV drugs, indicating a lower potential for abuse and dependence compared to opiates. However, some muscle relaxers, such as carisoprodol, have been reclassified to Schedule IV from unscheduled due to concerns over misuse and addiction. Understanding these scheduling differences is crucial for patients and healthcare providers to ensure appropriate use and minimize risks associated with these medications.
| Characteristics | Values |
|---|---|
| Classification | Muscle relaxers and opiates are classified differently under the Controlled Substances Act. |
| Schedule for Opiates | Most opiates (e.g., morphine, oxycodone) are Schedule II due to high potential for abuse and dependence. |
| Schedule for Muscle Relaxers | Most muscle relaxers (e.g., cyclobenzaprine, tizanidine) are not scheduled and are available by prescription. |
| Exceptions for Muscle Relaxers | Some muscle relaxers like carisoprodol are Schedule IV due to potential for abuse, but still not in the same schedule as opiates. |
| Potential for Abuse | Opiates have a higher potential for abuse and addiction compared to most muscle relaxers. |
| Medical Use | Both are used for pain management, but opiates are primarily for severe pain, while muscle relaxers target muscle spasms. |
| Side Effects | Opiates: respiratory depression, constipation, sedation. Muscle relaxers: drowsiness, dizziness, dry mouth. |
| Regulatory Control | Opiates face stricter prescribing and dispensing regulations compared to most muscle relaxers. |
| Dependency Risk | Opiates carry a significantly higher risk of physical and psychological dependence. |
| Examples | Opiates: morphine, oxycodone. Muscle relaxers: cyclobenzaprine, tizanidine, carisoprodol. |
Explore related products






What You'll Learn
- DEA Scheduling Overview: Muscle relaxers vs. opiates: DEA classification differences and legal implications
- Common Muscle Relaxers: Examples like Baclofen, Cyclobenzaprine, and their scheduling status
- Opiate Scheduling: Opioids like Oxycodone, Morphine, and their DEA Schedule II placement
- Addiction Potential: Comparing abuse risks of muscle relaxers and opiates
- Prescription Regulations: Differences in prescribing rules for muscle relaxers vs. opiates
![]()
DEA Scheduling Overview: Muscle relaxers vs. opiates: DEA classification differences and legal implications
Muscle relaxers and opiates are both prescription medications, but their DEA scheduling and legal implications differ significantly. The DEA classifies drugs into schedules based on their potential for abuse, medical utility, and safety profiles. Opiates, such as morphine and oxycodone, are typically classified as Schedule II substances due to their high potential for abuse and severe psychological or physical dependence. In contrast, most muscle relaxers, like cyclobenzaprine and baclofen, are not scheduled or are classified as Schedule IV, indicating a lower potential for abuse and dependence. This fundamental difference in scheduling has profound implications for prescribing practices, patient access, and legal consequences.
Consider the prescribing guidelines for these substances. Schedule II opiates require a written prescription, cannot be refilled, and are subject to strict quotas and monitoring. For instance, a 30-day supply of oxycodone must be accompanied by a hard copy prescription, and prescribers must register with the DEA. Muscle relaxers, on the other hand, often allow for refills and can be prescribed electronically. For example, a patient with chronic back pain might receive a 90-day supply of cyclobenzaprine with up to five refills, depending on state regulations. This disparity highlights the DEA’s recognition of opiates as high-risk substances, while muscle relaxers are generally viewed as safer for long-term use.
Legal implications further underscore the scheduling differences. Possession of Schedule II opiates without a valid prescription is a felony, often resulting in severe penalties, including imprisonment and fines. For instance, unauthorized possession of 100 grams of heroin (a Schedule I opiate) can lead to up to 20 years in prison under federal law. Muscle relaxers, being Schedule IV or unscheduled, carry far less severe penalties. Unauthorized possession of a Schedule IV substance, such as diazepam, typically results in misdemeanor charges with penalties like probation or short-term incarceration. However, misuse or distribution of either class of drugs can escalate legal consequences, emphasizing the importance of adhering to prescription guidelines.
Practical tips for patients and healthcare providers can mitigate risks associated with these substances. Patients prescribed opiates should store medications securely, avoid sharing prescriptions, and dispose of unused pills at designated collection sites. Providers should educate patients on the risks of dependence and monitor usage through prescription drug monitoring programs (PDMPs). For muscle relaxers, patients should follow dosage instructions carefully, as even these lower-risk drugs can cause drowsiness or impaired coordination. Providers should reassess the need for long-term muscle relaxer use, as prolonged reliance may mask underlying conditions requiring alternative treatments.
In summary, the DEA’s scheduling of muscle relaxers and opiates reflects their distinct risk profiles and informs their legal treatment. While opiates face stringent controls due to their high abuse potential, muscle relaxers enjoy more lenient regulations, facilitating broader access for legitimate medical use. Understanding these differences is crucial for patients, providers, and policymakers to navigate the complexities of prescription drug management and ensure safe, effective treatment.
Muscle Relaxers and Heart Rate: Understanding the Potential Impact
You may want to see also
Explore related products






![]()
Common Muscle Relaxers: Examples like Baclofen, Cyclobenzaprine, and their scheduling status
Muscle relaxers, often prescribed for acute musculoskeletal conditions, are not uniformly classified in the same scheduling category as opiates. While opiates like oxycodone and morphine are typically Schedule II controlled substances due to their high potential for abuse and dependence, muscle relaxers vary widely in their scheduling status. This distinction is crucial for understanding their accessibility, prescription requirements, and potential risks.
Baclofen, for instance, is a muscle relaxer commonly used to treat muscle spasms caused by conditions like multiple sclerosis or spinal cord injuries. Unlike opiates, baclofen is not a controlled substance in the United States, meaning it lacks the strict regulations associated with scheduled drugs. This unscheduled status allows for easier prescription and refills, though it does not diminish the importance of monitoring for side effects such as drowsiness or dizziness. Patients are typically advised to start with a low dose, around 5 mg three times daily, gradually increasing under medical supervision to minimize adverse reactions.
Cyclobenzaprine, another widely prescribed muscle relaxer, is classified as a Schedule IV controlled substance in some states but remains unscheduled federally. This classification reflects its lower potential for abuse compared to opiates, though it still carries risks, particularly when combined with alcohol or other central nervous system depressants. Prescribed for short-term relief of muscle spasms, cyclobenzaprine is often dosed at 5–10 mg up to three times daily. Patients, especially older adults, should be cautious due to increased sensitivity to its sedative effects.
The scheduling differences between muscle relaxers like baclofen and cyclobenzaprine highlight the need for individualized treatment plans. While neither is as tightly regulated as opiates, their misuse can still lead to dependence or adverse effects. For example, abruptly stopping baclofen can cause withdrawal symptoms, emphasizing the importance of tapering under medical guidance. Cyclobenzaprine’s Schedule IV status in some regions serves as a reminder to use it judiciously, particularly in populations prone to drug interactions or side effects.
In practice, healthcare providers must balance the benefits of muscle relaxers with their potential risks, considering factors like patient age, comorbidities, and concurrent medications. Unlike opiates, which are often reserved for severe pain due to their scheduling, muscle relaxers offer a more accessible but still regulated option for managing acute musculoskeletal issues. Understanding their scheduling status ensures appropriate prescribing practices and patient education, fostering safer and more effective treatment outcomes.
Optimal Duration for Progressive Muscle Relaxation Sessions: A Guide
You may want to see also
Explore related products



![]()
Opiate Scheduling: Opioids like Oxycodone, Morphine, and their DEA Schedule II placement
Opioids such as oxycodone and morphine are classified by the Drug Enforcement Administration (DEA) as Schedule II substances, a designation that reflects their high potential for abuse and severe psychological or physical dependence. This scheduling places them in a category reserved for drugs with accepted medical use but under strict controls. For instance, a prescription for oxycodone typically limits the quantity dispensed to a 30-day supply, and refills require a new prescription from a licensed practitioner. This contrasts with Schedule III or IV drugs, which may allow refills under certain conditions. Understanding this classification is crucial for both healthcare providers and patients, as it dictates prescribing practices, patient monitoring, and legal consequences for misuse.
Analyzing the rationale behind Schedule II placement reveals the delicate balance between therapeutic benefit and risk. Opioids like morphine are indispensable in managing severe pain, particularly post-surgery or in palliative care. However, their misuse can lead to rapid tolerance, dependence, and overdose. For example, a single dose of morphine sulfate ranges from 5 to 15 mg every 4 hours for pain relief, but exceeding this can escalate risks exponentially. The DEA’s scheduling ensures that these drugs are accessible for legitimate medical needs while minimizing diversion and abuse. This dual nature underscores why opioids remain tightly regulated, unlike muscle relaxants, which are generally classified in lower schedules due to their lower abuse potential.
From a practical standpoint, patients prescribed Schedule II opioids must adhere to specific guidelines to ensure safety and compliance. Prescriptions cannot be called in or faxed; they require a handwritten or electronic prescription directly from the provider. Patients should also be educated on proper storage (e.g., in a locked cabinet) and disposal (e.g., through take-back programs or DEA-approved methods). For adolescents and young adults, who are at higher risk for opioid misuse, providers often start with lower doses (e.g., 5 mg of oxycodone) and closely monitor for signs of dependency. Caregivers and family members play a critical role in overseeing medication use and recognizing early warning signs of abuse.
Comparatively, muscle relaxants like cyclobenzaprine (Flexeril) are typically classified as Schedule IV drugs, indicating a lower potential for abuse and dependence. This distinction highlights the DEA’s nuanced approach to drug regulation, tailoring controls to the specific risks posed by each substance. While opioids demand stringent oversight, muscle relaxants are prescribed with fewer restrictions, such as allowing refills and less frequent follow-ups. This disparity emphasizes the importance of understanding scheduling not just as a legal framework but as a tool for informed decision-making in pain management. Patients and providers alike benefit from recognizing these differences to optimize treatment outcomes while mitigating risks.
In conclusion, the DEA’s Schedule II placement of opioids like oxycodone and morphine serves as a critical safeguard in balancing their medical utility with inherent risks. By contrast, muscle relaxants’ lower scheduling reflects their comparatively safer profile. This distinction is not merely bureaucratic but has tangible implications for prescribing, patient care, and public health. Awareness of these classifications empowers individuals to navigate pain management more effectively, ensuring that powerful tools like opioids are used responsibly and reserved for cases where their benefits outweigh the dangers.
Understanding Muscle Relaxant Dosage: Grams and Safe Usage Explained
You may want to see also
![]()
Addiction Potential: Comparing abuse risks of muscle relaxers and opiates
Muscle relaxers and opiates, though both prescribed for pain management, are classified differently under the Controlled Substances Act. Opiates, such as oxycodone and morphine, are typically Schedule II drugs due to their high potential for abuse and severe dependence. Muscle relaxers, like cyclobenzaprine and tizanidine, are generally not scheduled or are classified as Schedule IV, indicating a lower risk of abuse and dependence. This classification difference reflects their distinct pharmacological profiles and addiction potentials.
Analyzing the abuse risks, opiates act on the brain’s reward system by binding to opioid receptors, producing euphoria and reinforcing repeated use. This mechanism makes them highly addictive, with studies showing that 21–29% of patients prescribed opioids for chronic pain misuse them, and 8–12% develop an opioid use disorder. In contrast, muscle relaxers primarily act on the central nervous system to alleviate muscle spasms, with minimal euphoric effects. For instance, cyclobenzaprine has a lower risk of abuse, though misuse can occur when taken in high doses (e.g., 60 mg or more) or combined with other substances like alcohol.
Instructively, healthcare providers must consider patient history when prescribing these medications. Opiates are often reserved for acute, severe pain due to their addiction potential, while muscle relaxers are preferred for musculoskeletal conditions like back pain or injury. For older adults (65+), muscle relaxers may be safer due to their lower risk of respiratory depression compared to opiates. However, both classes require careful monitoring, as even Schedule IV muscle relaxers can lead to dependence when used long-term or in high doses.
Persuasively, the lower scheduling of muscle relaxers should not lull prescribers or patients into a false sense of security. While their abuse potential is lower, misuse can still occur, particularly in individuals with a history of substance use disorders. For example, tizanidine, when taken in excess of 36 mg daily, can cause dizziness, hallucinations, and withdrawal symptoms upon abrupt cessation. Opiates, on the other hand, pose a more immediate and severe risk, with overdose deaths involving prescription opioids reaching over 16,000 in 2021, according to the CDC.
Comparatively, the addiction potential of these drugs underscores the need for alternative pain management strategies. Non-pharmacological approaches, such as physical therapy, acupuncture, or cognitive-behavioral therapy, can reduce reliance on medications. When pharmacotherapy is necessary, starting with the lowest effective dose and limiting treatment duration can mitigate risks. For instance, a 7-day supply of opioids is often sufficient for acute pain, while muscle relaxers should be prescribed for no more than 2–3 weeks.
In conclusion, while muscle relaxers and opiates serve distinct roles in pain management, their addiction potentials differ significantly. Opiates, with their Schedule II classification, pose a higher risk of abuse and dependence, necessitating strict prescribing practices. Muscle relaxers, though generally safer, are not without risks, particularly when misused or combined with other depressants. Understanding these differences is crucial for both healthcare providers and patients to balance effective pain relief with harm reduction.
Effective Techniques to Release Tension and Relax Your Neck Muscles
You may want to see also
![]()
Prescription Regulations: Differences in prescribing rules for muscle relaxers vs. opiates
Muscle relaxers and opiates, while both prescribed for pain management, fall under different regulatory schedules due to their distinct pharmacological profiles and potential for abuse. Opiates, such as oxycodone and hydrocodone, are classified as Schedule II controlled substances by the DEA, indicating a high potential for abuse and severe psychological or physical dependence. In contrast, most muscle relaxers, like cyclobenzaprine and tizanidine, are not scheduled or are classified as Schedule IV, suggesting a lower potential for abuse and dependence. This fundamental difference in scheduling dictates how these medications are prescribed, monitored, and dispensed.
Prescribing rules for opiates are stringent, reflecting their high abuse potential. Physicians must adhere to state-specific prescription drug monitoring programs (PDMPs), which track the dispensing of controlled substances to prevent misuse. Opiates are typically prescribed for acute pain, such as post-surgical recovery, and are limited to short durations, often 3–7 days. Refills are rarely automatic and require a new prescription. Additionally, prescribers must conduct thorough patient assessments, including medical history, risk factors for addiction, and alternative treatment options, before initiating opiate therapy.
Muscle relaxers, on the other hand, enjoy more lenient prescribing rules due to their lower abuse potential. They are commonly prescribed for musculoskeletal conditions like back pain or muscle spasms and can be used for longer durations, often 2–3 weeks. Refills are more readily granted, and some states allow pharmacists to extend prescriptions without a new authorization. However, prescribers must still exercise caution, particularly with patients who have a history of substance abuse or are concurrently taking central nervous system depressants, as muscle relaxers can potentiate sedation and respiratory depression.
A critical difference lies in the monitoring and documentation requirements. Opiate prescriptions necessitate detailed record-keeping, including informed consent, treatment agreements, and periodic urine drug testing to ensure compliance and detect misuse. Muscle relaxers, while not subject to the same level of scrutiny, still require careful patient monitoring, especially for adverse effects like dizziness, drowsiness, or liver toxicity. Prescribers must balance the therapeutic benefits against the risks, particularly in elderly patients or those with renal impairment, where dosage adjustments may be necessary.
In practice, understanding these regulatory differences is essential for both healthcare providers and patients. For instance, a patient prescribed cyclobenzaprine for chronic back pain may receive a 90-day supply with refills, whereas a patient prescribed oxycodone for post-surgical pain will likely receive a 3-day supply with no refills. Providers must navigate these rules to ensure compliance while optimizing patient care, while patients should be educated on the appropriate use, storage, and disposal of these medications to mitigate risks. Ultimately, the divergent scheduling of muscle relaxers and opiates underscores the need for tailored prescribing practices that prioritize safety and efficacy.
Extracellular Fluid's Role in Smooth Muscle Contraction and Relaxation
You may want to see also
Frequently asked questions
No, muscle relaxers are generally not classified in the same schedule as opiates. Opiates, such as morphine and oxycodone, are typically Schedule II controlled substances due to their high potential for abuse and dependence. Muscle relaxers, like cyclobenzaprine or tizanidine, are usually not scheduled or are classified as Schedule IV, indicating a lower potential for abuse.
Muscle relaxers are generally less addictive than opiates. While some muscle relaxers may cause dependence with prolonged use, their addictive potential is significantly lower compared to opiates, which are highly addictive and carry a greater risk of misuse and severe withdrawal symptoms.
No, muscle relaxers are typically prescribed differently than opiates. Opiates are usually prescribed for severe pain and are closely monitored due to their high risk of abuse. Muscle relaxers are prescribed for muscle spasms or pain and are often used for shorter durations, with less stringent monitoring compared to opiates.