Muscle relaxers, often prescribed to alleviate muscle spasms and pain, are a class of medications that work by targeting the central nervous system or directly affecting muscle fibers. While they are primarily known for their ability to reduce muscle tension, there is ongoing debate about whether they can be classified as depressants. Depressants are substances that slow down brain activity, leading to relaxation and sedation, and some muscle relaxers, particularly those acting on the central nervous system, share similar effects. However, not all muscle relaxers fall into this category, as some work peripherally on muscles without significantly impacting brain function. Understanding whether muscle relaxers are depressants is crucial for assessing their potential risks, side effects, and interactions with other medications, especially for individuals with conditions like anxiety, depression, or substance use disorders.
| Characteristics | Values |
|---|---|
| Classification | Muscle relaxers are generally classified as central nervous system (CNS) depressants. |
| Mechanism of Action | They work by reducing nerve activity in the brain and spinal cord, leading to muscle relaxation. |
| Types | Include antispasmodics (e.g., Baclofen) and antispastics (e.g., Tizanidine), both of which have depressant effects. |
| Effects on CNS | Slow down brain activity, causing drowsiness, reduced anxiety, and relaxation. |
| Side Effects | Common side effects include fatigue, dizziness, and impaired coordination, typical of depressants. |
| Potential for Dependence | Prolonged use can lead to physical dependence and withdrawal symptoms, similar to other depressants. |
| Medical Use | Prescribed for muscle spasms, pain, and conditions like multiple sclerosis or spinal cord injuries. |
| Interaction with Other Depressants | Can enhance the effects of alcohol, opioids, and benzodiazepines, increasing sedation and risk. |
| Legal Status | Many muscle relaxers are prescription-only due to their depressant properties and potential for misuse. |
| Overdose Risk | Overdose can cause severe CNS depression, respiratory failure, and coma, similar to other depressants. |
Explore related products






What You'll Learn
![]()
How Muscle Relaxers Work
Muscle relaxers, often prescribed for acute musculoskeletal conditions, primarily target the central nervous system (CNS) to alleviate pain and reduce muscle spasms. Unlike direct muscle intervention, these medications act on the brain and spinal cord, modulating nerve signals to decrease muscle activity. For instance, baclofen mimics GABA, an inhibitory neurotransmitter, to suppress nerve excitation, while tizanidine reduces spinal cord neuron activity. This CNS-centric mechanism distinguishes muscle relaxers from topical treatments or physical therapy, making them effective for conditions like lower back pain or multiple sclerosis-related spasms. However, their systemic action raises questions about their classification as depressants, as they share similarities with CNS depressants like benzodiazepines.
Consider the dosage and administration of muscle relaxers, which underscore their potent effects on the CNS. Cyclobenzaprine, for example, is typically prescribed at 5–10 mg three times daily, with a maximum dose of 30 mg/day, due to its sedative properties. Similarly, diazepam, another muscle relaxer with depressant qualities, is dosed at 2–10 mg, 2–4 times daily, depending on the patient’s age and condition. Elderly patients often require lower doses due to increased sensitivity to CNS depressants, highlighting the need for tailored prescriptions. Overdosing or combining these medications with alcohol or opioids can amplify depressant effects, leading to respiratory depression or severe drowsiness. Always follow a healthcare provider’s instructions and avoid abrupt discontinuation to minimize withdrawal risks.
Comparatively, muscle relaxers and traditional CNS depressants share overlapping mechanisms but serve distinct purposes. While depressants like barbiturates or alcohol broadly suppress brain activity, muscle relaxers target specific pathways to reduce muscle tension without necessarily inducing sedation in all cases. For instance, dantrolene acts directly on muscle fibers, bypassing the CNS entirely, though it’s less commonly prescribed due to potential side effects like liver toxicity. In contrast, methocarbamol’s mild depressant effects are often secondary to its muscle-relaxing properties, making it a preferred choice for patients needing daytime relief. This nuanced distinction explains why muscle relaxers are sometimes categorized as depressants but are not universally classified as such.
Practically, integrating muscle relaxers into a treatment plan requires balancing efficacy with side effects. Patients should avoid activities requiring alertness, such as driving, until they understand how the medication affects them. Combining muscle relaxers with heat therapy or gentle stretching can enhance their effectiveness, but caution is advised to prevent overexertion. For chronic conditions, periodic reassessment of the medication’s necessity is crucial, as prolonged use may lead to tolerance or dependence. Pregnant or breastfeeding individuals should consult their doctor, as some muscle relaxers pose risks to fetal or infant health. Ultimately, while muscle relaxers can provide significant relief, their depressant-like qualities necessitate informed, cautious use.
Chamomile Tea's Muscle Relaxing Benefits: Fact or Fiction?
You may want to see also
Explore related products






![]()
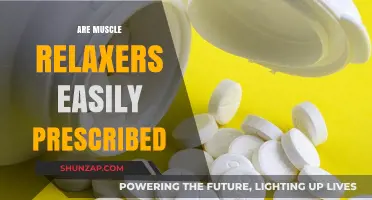
Depressant Effects on CNS
Muscle relaxers, often prescribed for acute musculoskeletal conditions, exert depressant effects on the central nervous system (CNS) by modulating neuronal activity. These medications, such as cyclobenzaprine and tizanidine, primarily act on the spinal cord and brainstem to reduce muscle tone and alleviate pain. Their mechanism involves enhancing inhibitory neurotransmitters like GABA or directly suppressing nerve signal transmission, which parallels the action of classic CNS depressants like benzodiazepines or barbiturates. This shared pharmacological pathway raises the question: Are muscle relaxers, in essence, depressants?
Consider the dosage implications. Cyclobenzaprine, for instance, is typically prescribed at 5–10 mg three times daily, but even within therapeutic ranges, it can induce drowsiness, dizziness, and cognitive impairment—hallmarks of CNS depression. Tizanidine, dosed at 2–4 mg every 6–8 hours, carries a higher risk of sedation and hypotension, particularly in elderly patients or those with hepatic impairment. These side effects underscore the fine line between therapeutic benefit and depressant-like adverse reactions, necessitating careful titration and patient monitoring.
From a comparative standpoint, muscle relaxers differ from traditional depressants in their primary indication but overlap in their CNS impact. Unlike benzodiazepines, which are broadly used for anxiety or insomnia, muscle relaxers target musculoskeletal pain. However, their ability to reduce neuronal excitability aligns them with depressants in terms of potential for abuse, dependence, and respiratory depression, especially when combined with alcohol or opioids. This duality highlights the need for prescribers to balance efficacy with safety, particularly in vulnerable populations such as the elderly or those with comorbidities.
Practically, patients using muscle relaxers should adopt specific precautions to mitigate CNS depressant effects. Avoid operating heavy machinery or driving until tolerance to sedation is established. Limit alcohol consumption, as it potentiates CNS depression. For those on tizanidine, monitor blood pressure regularly, as hypotension can occur within 1–2 hours post-dose. Additionally, consider non-pharmacological alternatives like physical therapy or heat therapy for muscle pain, especially in cases where the risk of CNS depression outweighs the benefit.
In conclusion, muscle relaxers function as depressants on the CNS through their mechanism of action and side effect profile. While their therapeutic role is distinct, their potential for sedation, cognitive impairment, and drug interactions warrants cautious use. Understanding this depressant effect is crucial for both clinicians and patients to optimize treatment outcomes while minimizing risks.
Unwinding Muscles: Understanding Relaxation's Impact on Muscle Structure and Function
You may want to see also
Explore related products






![]()
Side Effects Comparison
Muscle relaxers and depressants, while distinct in their primary functions, share overlapping side effects that warrant careful comparison. Both classes of drugs can induce drowsiness, dizziness, and impaired coordination, but the intensity and duration of these effects vary significantly. For instance, cyclobenzaprine, a commonly prescribed muscle relaxer, often causes pronounced sedation, particularly at higher doses (10–30 mg), whereas benzodiazepines like diazepam, a depressant, may produce similar symptoms but with a longer half-life, increasing the risk of next-day impairment. Understanding these nuances is critical for patients managing conditions like chronic pain or anxiety, where the choice of medication can impact daily functioning.
From a practical standpoint, the side effect profiles of muscle relaxers and depressants demand tailored management strategies. Muscle relaxers frequently cause dry mouth and blurred vision, which can be mitigated by staying hydrated and avoiding activities requiring sharp visual acuity, such as driving. Depressants, on the other hand, often lead to cognitive slowing and memory issues, particularly in older adults (aged 65 and above), who are more susceptible to these effects due to age-related metabolic changes. Patients on depressants should be advised to take their medication at bedtime to minimize daytime interference, while those on muscle relaxers may benefit from splitting doses to reduce peak sedation.
A persuasive argument for cautious prescribing emerges when examining the additive risks of combining muscle relaxers and depressants. Both drug classes depress the central nervous system, and concurrent use can lead to dangerous respiratory depression or profound sedation. For example, pairing tizanidine (a muscle relaxer) with alcohol or opioids amplifies these risks exponentially. Clinicians must educate patients about these interactions, emphasizing the importance of disclosing all medications, including over-the-counter sleep aids or antihistamines, which can further potentiate depressant effects.
Comparatively, the withdrawal symptoms of muscle relaxers and depressants highlight another dimension of side effect management. Depressants, particularly benzodiazepines, are notorious for causing rebound anxiety, insomnia, and seizures upon abrupt discontinuation, necessitating a gradual tapering regimen over weeks or months. Muscle relaxers, while less habit-forming, can still lead to rebound muscle spasms and discomfort if stopped suddenly. Patients should be instructed to follow a structured tapering plan, reducing doses by no more than 25% weekly for depressants and 10–20% weekly for muscle relaxers, depending on the specific medication and duration of use.
In conclusion, while muscle relaxers and depressants are not pharmacologically identical, their side effect profiles demand similar vigilance and patient education. By focusing on specific symptoms, practical management strategies, and potential risks, healthcare providers can optimize treatment outcomes and minimize adverse events. Whether prescribing cyclobenzaprine for musculoskeletal pain or diazepam for anxiety, the goal remains the same: balancing therapeutic benefits with the safety and well-being of the patient.
Discover Natural Muscle Relaxers: Effective Remedies for Tension Relief
You may want to see also
Explore related products



$9.65 $12.49

![]()
Medical Uses vs. Risks
Muscle relaxers, often prescribed for acute musculoskeletal conditions, serve a critical medical purpose by alleviating pain and improving mobility. For instance, cyclobenzaprine (Flexeril) is commonly used to treat muscle spasms caused by injuries like strains or sprains, typically at doses of 5 to 10 mg three times daily. Similarly, tizanidine (Zanaflex) is prescribed for spasticity in conditions such as multiple sclerosis, with dosages ranging from 2 to 8 mg every 6 to 8 hours. These medications act centrally on the nervous system, reducing muscle tension and allowing patients to engage in physical therapy or resume daily activities. Their effectiveness in short-term use (2-3 weeks) is well-documented, particularly when combined with rest and rehabilitation.
However, the risks associated with muscle relaxers cannot be overlooked, especially when misused or taken long-term. Common side effects include drowsiness, dizziness, and dry mouth, which can impair daily functioning. For example, older adults (aged 65 and above) are more susceptible to these effects due to slower metabolism and potential drug interactions with other medications. More severe risks include respiratory depression, particularly when muscle relaxers are combined with opioids or alcohol. A 2020 study found that concurrent use of tizanidine and opioids increased the risk of hospitalization by 60%. Additionally, prolonged use can lead to dependence, with withdrawal symptoms such as insomnia, nausea, and rebound muscle pain.
To balance medical uses and risks, healthcare providers must adhere to strict prescribing guidelines. Muscle relaxers should be reserved for acute conditions and avoided in patients with a history of substance abuse or liver disease. For instance, methocarbamol (Robaxin) is often preferred for its lower risk of sedation, but it still requires dose adjustments in patients with renal impairment. Patients must also be educated on proper use, such as avoiding alcohol and not driving until they understand how the medication affects them. Combining muscle relaxers with non-pharmacological treatments like heat therapy or stretching can enhance efficacy while minimizing reliance on medication.
A comparative analysis reveals that while muscle relaxers share depressant qualities with other central nervous system (CNS) depressants like benzodiazepines, their medical utility is more specialized. Unlike benzodiazepines, which are primarily used for anxiety or insomnia, muscle relaxers target musculoskeletal issues directly. However, their depressant effects necessitate cautious prescribing, particularly in vulnerable populations. For example, diazepam (Valium) is sometimes used as a muscle relaxer but carries a higher risk of cognitive impairment in older adults compared to cyclobenzaprine. This highlights the importance of selecting the most appropriate medication based on patient-specific factors.
In conclusion, muscle relaxers are valuable tools in managing acute musculoskeletal conditions, but their depressant properties demand careful consideration of risks. By adhering to short-term use, monitoring for side effects, and integrating them with non-pharmacological therapies, healthcare providers can maximize benefits while minimizing harm. Patients, too, play a crucial role in adhering to prescribed dosages and reporting any adverse effects promptly. This balanced approach ensures that muscle relaxers remain a safe and effective option in the medical arsenal.
Safe Dosage Guide: 10 mg Muscle Relaxers – How Much to Take?
You may want to see also
Explore related products





![]()
Potential for Dependence
Muscle relaxers, often prescribed for acute musculoskeletal conditions, carry a significant risk of dependence, particularly when used beyond the recommended duration or dosage. These medications, such as cyclobenzaprine and carisoprodol, act on the central nervous system to alleviate muscle spasms and pain. However, their depressant effects can lead to psychological and physical reliance, especially in individuals with a history of substance use disorders. For instance, carisoprodol, when combined with alcohol or opioids, enhances its sedative properties, increasing the likelihood of misuse. Patients prescribed these drugs should strictly adhere to their healthcare provider’s instructions, typically limiting use to 2–3 weeks, to minimize the risk of dependence.
The mechanism of dependence often begins with tolerance, where the body requires higher doses to achieve the same effect. For example, a patient initially prescribed 350 mg of carisoprodol twice daily might find the medication less effective over time, prompting self-increased dosages without medical oversight. This behavior can escalate to physical dependence, marked by withdrawal symptoms such as insomnia, tremors, and anxiety when the drug is discontinued. Withdrawal severity varies but is particularly pronounced in long-term users or those with pre-existing mental health conditions. Healthcare providers must monitor patients closely, especially those over 65 or with a history of addiction, to prevent the progression from therapeutic use to dependence.
To mitigate dependence, healthcare professionals should prioritize non-pharmacological interventions, such as physical therapy and heat therapy, before prescribing muscle relaxers. When medication is necessary, they should educate patients about the risks and provide clear guidelines. For instance, cyclobenzaprine should be taken at the lowest effective dose, typically 5–10 mg three times daily, and avoided in patients with glaucoma or thyroid disorders. Patients should also be advised to avoid alcohol and other central nervous system depressants while on these medications. Regular follow-ups are essential to assess efficacy and monitor for signs of misuse, ensuring early intervention if dependence emerges.
Comparatively, muscle relaxers like tizanidine and baclofen have a lower potential for dependence but still require cautious use. Tizanidine, for example, is often preferred for its shorter duration of action, reducing the risk of accumulation in the system. However, its abrupt discontinuation can lead to rebound hypertension, emphasizing the need for gradual tapering. Baclofen, while effective for spasticity, can cause dizziness and drowsiness, particularly in older adults, necessitating dose adjustments. Patients and providers must weigh the benefits against the risks, considering alternatives like benzodiazepines or even non-drug therapies, to avoid the pitfalls of dependence associated with long-term muscle relaxer use.
In conclusion, the potential for dependence on muscle relaxers underscores the need for informed, cautious prescribing practices. Patients must be proactive in reporting any changes in their response to the medication or unusual cravings. Providers should employ a multifaceted approach, combining medication management with behavioral strategies, to address both the physical and psychological aspects of dependence. By fostering awareness and adherence to guidelines, the therapeutic benefits of muscle relaxers can be maximized while minimizing the risks of long-term reliance.
Muscle Relaxers and Mental Fogginess: Do They Make You Loopy?
You may want to see also
Frequently asked questions
Yes, many muscle relaxers act as central nervous system (CNS) depressants, slowing down brain activity to reduce muscle spasms and pain.
Muscle relaxers work by suppressing the nervous system, decreasing nerve signals to muscles and promoting relaxation, which is a characteristic effect of depressants.
No, not all muscle relaxers are depressants. Some work directly on muscles (peripheral muscle relaxants) rather than the CNS, while others do have depressant effects.
Risks include drowsiness, dizziness, impaired coordination, and potential for dependence or overdose, especially when combined with other depressants like alcohol or opioids.