Muscle relaxers and painkillers are often confused due to their overlapping uses in managing discomfort, but they serve distinct purposes and function differently in the body. Muscle relaxers, such as cyclobenzaprine or tizanidine, primarily target muscle spasms and tension by acting on the central nervous system to reduce muscle activity, while painkillers, or analgesics, like acetaminophen or opioids, work to alleviate pain signals in the brain and throughout the body. Although both can provide relief, their mechanisms, side effects, and appropriate applications vary significantly, making it essential to understand their differences for effective and safe use.
| Characteristics | Values |
|---|---|
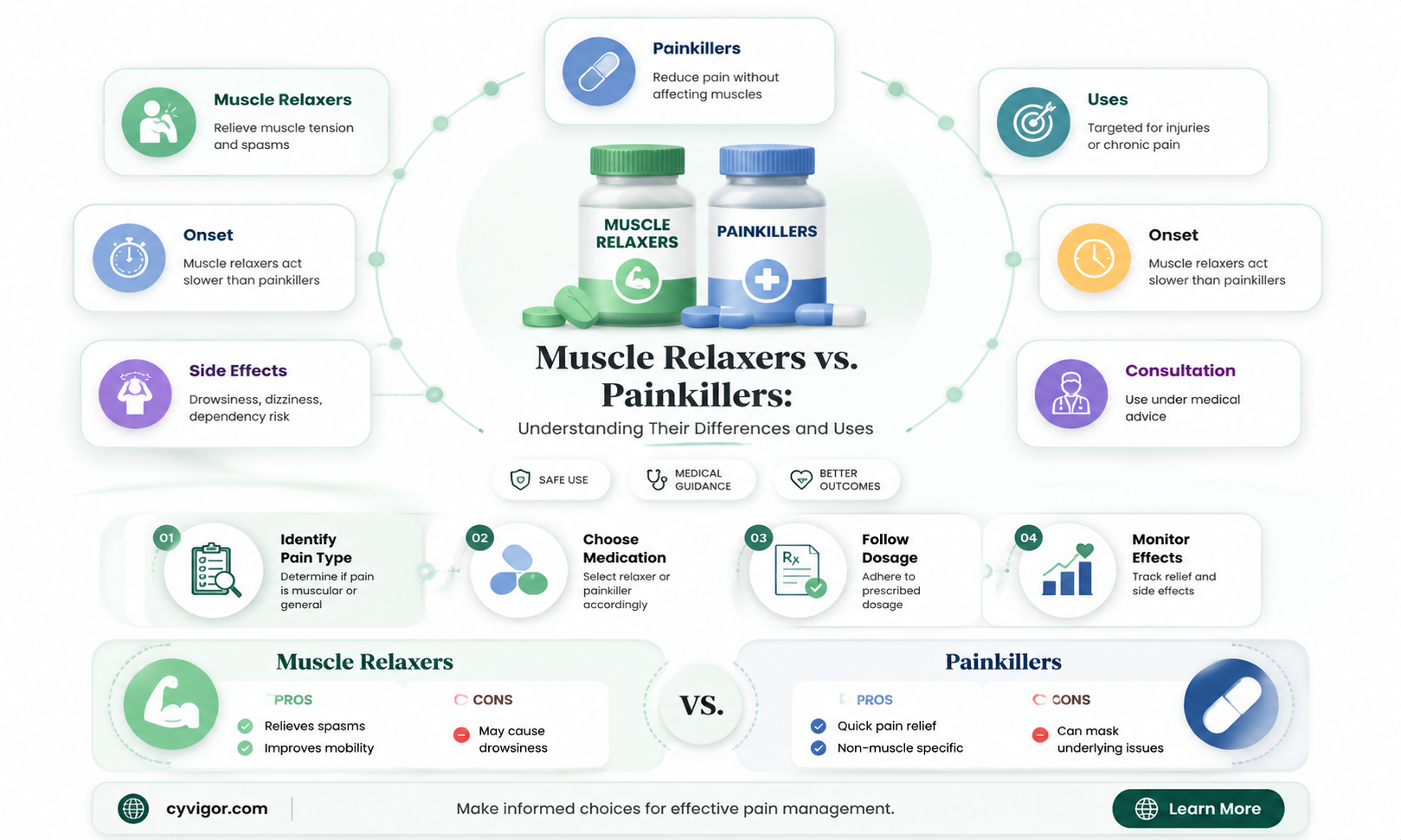
| Primary Function | Muscle relaxers primarily target muscle spasms and stiffness, while painkillers (analgesics) focus on reducing pain signals to the brain. |
| Mechanism of Action | Muscle relaxers act on the central nervous system (CNS) or directly on muscles to reduce tension. Painkillers block pain pathways in the CNS or periphery. |
| Types | Muscle relaxers: e.g., Cyclobenzaprine, Baclofen, Tizanidine. Painkillers: e.g., Acetaminophen, NSAIDs (Ibuprofen), Opioids (Morphine). |
| Common Uses | Muscle relaxers: Muscle spasms, back pain, injuries. Painkillers: Headaches, arthritis, post-surgery pain, chronic pain. |
| Side Effects | Muscle relaxers: Drowsiness, dizziness, dry mouth. Painkillers: Stomach upset, liver damage (acetaminophen), addiction (opioids). |
| Addiction Risk | Muscle relaxers: Moderate risk, especially with prolonged use. Painkillers: High risk, especially opioids. |
| Over-the-Counter Availability | Muscle relaxers: Generally prescription-only. Painkillers: Some (e.g., acetaminophen, ibuprofen) are OTC; others require prescription. |
| Interaction with Other Medications | Both can interact with other CNS depressants (e.g., alcohol, benzodiazepines), but specifics vary by drug. |
| Long-Term Use | Muscle relaxers: Not typically recommended for long-term use due to tolerance and side effects. Painkillers: Depends on type; opioids risky long-term, NSAIDs safer but still monitored. |
| Effect on Pain Perception | Muscle relaxers: Indirectly reduce pain by relaxing muscles. Painkillers: Directly reduce pain perception. |
| Examples of Conditions Treated | Muscle relaxers: Fibromyalgia, multiple sclerosis. Painkillers: Migraines, dental pain, cancer pain. |
| Potential for Overdose | Muscle relaxers: Possible but less common. Painkillers: High risk, especially opioids. |
| Impact on Mobility | Muscle relaxers: Improve mobility by reducing muscle stiffness. Painkillers: May improve mobility by reducing pain but do not directly relax muscles. |
Explore related products






What You'll Learn
- Mechanism of Action: How muscle relaxers and painkillers differ in targeting pain and muscle tension
- Types of Medications: Classification of muscle relaxers vs. painkillers (e.g., opioids, NSAIDs)
- Side Effects: Comparison of potential risks and adverse effects of both drug types
- Use Cases: When muscle relaxers or painkillers are prescribed for specific conditions
- Interactions & Overlap: How these drugs may interact or be used together in treatment
![]()
Mechanism of Action: How muscle relaxers and painkillers differ in targeting pain and muscle tension
Muscle relaxers and painkillers, though often prescribed together, operate through distinct mechanisms to alleviate discomfort. Painkillers, such as acetaminophen (Tylenol) or nonsteroidal anti-inflammatory drugs (NSAIDs) like ibuprofen (Advil), primarily target the central nervous system or inflammation pathways. They block pain signals or reduce inflammatory responses, providing systemic relief. Muscle relaxers, on the other hand, act directly on the musculoskeletal system by inhibiting nerve impulses or altering muscle fiber function, easing spasms and tension. For instance, cyclobenzaprine (Flexeril) depresses the central nervous system, while baclofen (Lioresal) acts on spinal cord receptors to reduce muscle hyperactivity.
Consider a scenario where a patient experiences lower back pain due to muscle spasms. An NSAID like naproxen (Aleve) might be prescribed at 500 mg twice daily to reduce inflammation and pain perception. However, if muscle tension persists, a muscle relaxer like tizanidine (Zanaflex) could be added, starting at 2 mg every 6–8 hours, with dosage adjustments based on tolerance. This combination targets both the inflammatory and neuromuscular components of pain, offering more comprehensive relief. It’s crucial to monitor for side effects, such as drowsiness or dizziness, especially in older adults or those with renal impairment.
From a persuasive standpoint, understanding these mechanisms empowers patients to advocate for tailored treatment plans. For acute injuries, a short-term regimen of NSAIDs paired with a muscle relaxer can break the cycle of pain and tension, promoting faster recovery. However, long-term use of muscle relaxers should be approached cautiously due to risks of dependence or cognitive impairment. Painkillers, while effective for mild to moderate pain, may not address the root cause of muscle spasms, making them less ideal as standalone treatments for musculoskeletal conditions.
A comparative analysis reveals that while both classes aim to alleviate discomfort, their applications differ significantly. Painkillers are versatile, addressing a wide range of pain types, from headaches to post-surgical aches. Muscle relaxers, however, are niche, reserved for conditions like fibromyalgia, multiple sclerosis, or acute muscle strains. For example, methocarbamol (Robaxin) is often preferred for its minimal sedative effects compared to cyclobenzaprine, making it suitable for daytime use. Conversely, opioids like oxycodone, though potent painkillers, lack muscle-relaxing properties and carry higher risks of addiction.
In practice, combining these medications requires careful consideration. A patient with chronic neck pain might benefit from a low-dose NSAID regimen supplemented by occasional use of a muscle relaxer during flare-ups. Lifestyle modifications, such as physical therapy or heat therapy, can enhance efficacy while reducing reliance on medication. Always consult a healthcare provider to determine the safest and most effective approach, as individual responses to these drugs vary widely. Understanding their mechanisms ensures informed decisions, optimizing pain management while minimizing risks.
Post-Back Surgery Muscle Relaxer Use: Duration and Recovery Tips
You may want to see also
Explore related products






![]()
Types of Medications: Classification of muscle relaxers vs. painkillers (e.g., opioids, NSAIDs)
Muscle relaxers and painkillers, though often prescribed together, serve distinct purposes and belong to different pharmacological classes. Muscle relaxers, such as cyclobenzaprine (Flexeril) and tizanidine (Zanaflex), target the central nervous system to alleviate muscle spasms and stiffness. They are typically used for acute conditions like lower back pain or injury-related tension. Painkillers, on the other hand, are broadly categorized into opioids (e.g., oxycodone, morphine) and nonsteroidal anti-inflammatory drugs (NSAIDs, e.g., ibuprofen, naproxen). Opioids act on the brain to reduce pain perception, while NSAIDs inhibit inflammation and pain at the site of injury. Understanding these classifications is crucial for effective treatment and minimizing side effects.
Consider the mechanism of action to differentiate these medications. Muscle relaxers work by depressing the central nervous system, often causing drowsiness, dizziness, and impaired coordination. For instance, cyclobenzaprine is typically prescribed at 5–10 mg three times daily, but patients are advised to avoid driving or operating machinery due to its sedative effects. Painkillers like opioids bind to opioid receptors in the brain and spinal cord, providing potent pain relief but carrying a high risk of dependence. NSAIDs, in contrast, block enzymes (COX-1 and COX-2) involved in inflammation, making them suitable for mild to moderate pain. For example, ibuprofen is commonly dosed at 200–400 mg every 4–6 hours, with a maximum daily limit of 1,200 mg to prevent gastrointestinal bleeding.
When comparing these medications, it’s essential to weigh their benefits against risks. Muscle relaxers are generally short-term solutions due to their side effects and potential for tolerance. Painkillers, particularly opioids, are reserved for severe pain but come with significant risks, including addiction and respiratory depression. NSAIDs are safer for long-term use but can cause kidney damage or cardiovascular issues if overused. For instance, elderly patients or those with pre-existing conditions may require lower doses or alternative treatments. Always consult a healthcare provider to determine the most appropriate medication based on the type and severity of pain.
Practical tips can enhance the effectiveness and safety of these medications. For muscle relaxers, combine them with physical therapy or stretching exercises to address the root cause of muscle tension. When using painkillers, follow the prescribed dosage strictly and avoid alcohol, as it can exacerbate side effects. For NSAIDs, take them with food to reduce stomach irritation, and stay hydrated to protect kidney function. Additionally, monitor for signs of adverse reactions, such as difficulty breathing (opioids) or unexplained bruising (NSAIDs), and seek medical attention immediately if they occur. By understanding the unique properties of muscle relaxers and painkillers, patients can make informed decisions to manage pain effectively.
Celexa and Muscle Relaxers: Potential Interactions and Safety Concerns
You may want to see also
Explore related products






![]()
Side Effects: Comparison of potential risks and adverse effects of both drug types
Muscle relaxers and painkillers, while both used to manage discomfort, carry distinct side effect profiles that patients and healthcare providers must weigh carefully. Muscle relaxers, such as cyclobenzaprine and tizanidine, primarily target muscle spasms and are often prescribed for conditions like lower back pain. Common side effects include drowsiness, dizziness, and dry mouth. For instance, cyclobenzaprine can cause significant sedation, particularly in older adults, with studies showing that up to 30% of patients over 65 experience pronounced fatigue. In contrast, painkillers, ranging from over-the-counter acetaminophen to prescription opioids like oxycodone, address a broader spectrum of pain but come with their own risks. Opioids, for example, are notorious for causing nausea, constipation, and respiratory depression, with the latter being a potentially life-threatening complication, especially at higher doses or when combined with alcohol.
The risk of dependency and addiction sharply differentiates painkillers, particularly opioids, from muscle relaxers. Opioids alter the brain’s reward system, leading to physical and psychological dependence, even when used as prescribed. The CDC reports that misuse of prescription opioids contributes to over 15,000 overdose deaths annually in the U.S. Muscle relaxers, while less addictive, are not without risk; prolonged use of drugs like carisoprodol can lead to tolerance and withdrawal symptoms, including anxiety and insomnia. However, their addictive potential is generally lower, making them a safer option for short-term use in patients without a history of substance abuse.
Another critical distinction lies in the cardiovascular and cognitive effects of these drugs. Muscle relaxers, particularly baclofen, can cause hypotension (low blood pressure), especially when initiating therapy or increasing doses. Patients are often advised to start with a low dose, such as 5 mg three times daily, and gradually titrate upward to minimize this risk. Painkillers, especially NSAIDs like ibuprofen, can elevate blood pressure and increase the risk of heart attack or stroke, particularly in individuals with pre-existing cardiovascular conditions. For example, long-term NSAID use is associated with a 19% increased risk of hypertension, according to a study published in *The BMJ*.
Practical considerations for minimizing side effects include patient-specific factors such as age, renal function, and concurrent medications. Older adults, for instance, metabolize drugs more slowly and are at higher risk for adverse effects from both muscle relaxers and painkillers. Acetaminophen, a common painkiller, can cause liver damage if dosed above 3,000 mg per day, particularly in patients with pre-existing liver conditions or those consuming alcohol regularly. To mitigate risks, healthcare providers often recommend combining therapies, such as pairing a muscle relaxer with physical therapy or using a topical NSAID instead of an oral formulation to reduce systemic exposure.
In conclusion, while both muscle relaxers and painkillers are valuable tools for pain management, their side effect profiles demand careful consideration. Muscle relaxers pose risks of sedation and hypotension but carry a lower addiction potential, making them suitable for acute musculoskeletal conditions. Painkillers, particularly opioids, offer potent pain relief but come with significant risks of dependency, gastrointestinal issues, and cardiovascular complications. Tailoring treatment to the patient’s specific needs, monitoring for adverse effects, and exploring non-pharmacological alternatives can optimize outcomes while minimizing harm.
Understanding Muscle Relaxation: The Sliding Filament Theory Explained
You may want to see also
Explore related products





![]()
Use Cases: When muscle relaxers or painkillers are prescribed for specific conditions
Muscle relaxers and painkillers, though often confused, serve distinct purposes in medical treatment. While painkillers primarily target pain perception, muscle relaxers focus on reducing muscle spasms and tension. Understanding their unique use cases is crucial for effective prescription and patient management.
Acute Musculoskeletal Injuries: A Case for Muscle Relaxers
In cases of acute injuries like strained backs or neck pain, muscle relaxers such as cyclobenzaprine (5–10 mg thrice daily) or tizanidine (2–4 mg every 6–8 hours) are often prescribed. These medications alleviate muscle spasms that exacerbate pain, enabling patients to move more comfortably during recovery. Unlike painkillers, they do not directly address pain but work by calming overactive muscles. Patients are typically advised to take these medications at night due to their sedative effects, ensuring rest without daytime drowsiness.
Chronic Pain Management: The Role of Painkillers
For chronic conditions like osteoarthritis or neuropathic pain, painkillers such as acetaminophen (up to 3,000 mg/day) or NSAIDs (e.g., ibuprofen 600 mg every 6 hours) are commonly prescribed. Opioids like oxycodone (5–10 mg every 4–6 hours) may be used for severe cases but are reserved due to addiction risks. Painkillers target pain pathways in the nervous system, providing relief that muscle relaxers cannot. Dosage adjustments are often necessary based on patient tolerance and pain severity, with regular monitoring to prevent side effects like liver damage or gastrointestinal issues.
Post-Surgical Recovery: A Combined Approach
After surgeries, such as spinal procedures or joint replacements, a combination of muscle relaxers and painkillers may be prescribed. For instance, a patient might receive hydrocodone/acetaminophen (5 mg/325 mg every 4–6 hours) for pain alongside methocarbamol (500–1,500 mg every 4–6 hours) to reduce muscle rigidity. This dual approach addresses both pain and muscle tension, enhancing recovery. Patients are cautioned about potential side effects like dizziness or constipation and advised to avoid alcohol or heavy machinery operation.
Pediatric and Elderly Considerations: Tailored Prescriptions
In pediatric cases, muscle relaxers are rarely used due to limited safety data, while painkillers like ibuprofen (10 mg/kg every 6–8 hours) are preferred for conditions like post-surgical pain. For the elderly, lower doses of both medications are recommended—for example, cyclobenzaprine (2.5 mg daily) to minimize risks of falls or cognitive impairment. Painkillers like tramadol (25–50 mg every 6 hours) may be used cautiously, balancing pain relief with side effects like sedation. Always consult a pediatrician or geriatric specialist for age-specific dosing and monitoring.
Practical Tips for Patients
When prescribed muscle relaxers or painkillers, follow these tips: take medications as directed, avoid abrupt discontinuation, and report side effects promptly. For muscle relaxers, plan for rest after dosing; for painkillers, pair with physical therapy or ice/heat therapy for optimal results. Always disclose other medications to prevent interactions, especially with opioids or sedatives. Understanding the specific use case of your prescription ensures safer, more effective treatment.
Muscle Relaxers and Digestion: Understanding Their Impact on Your Gut
You may want to see also
Explore related products






![]()
Interactions & Overlap: How these drugs may interact or be used together in treatment
Muscle relaxers and painkillers, though distinct in their primary functions, often intersect in treatment plans, particularly for conditions involving musculoskeletal pain. Understanding their interactions is crucial for optimizing therapy and minimizing risks. For instance, cyclobenzaprine, a common muscle relaxant, is frequently paired with acetaminophen or ibuprofen to address both muscle spasms and associated pain. However, this combination requires careful consideration, as both drug classes can cause central nervous system depression, potentially amplifying side effects like drowsiness or dizziness.
When prescribing these medications together, clinicians often start with the lowest effective doses. For adults, a typical regimen might include 5–10 mg of cyclobenzaprine three times daily, combined with 650 mg of acetaminophen every 4–6 hours as needed for pain. Elderly patients or those with hepatic impairment may require reduced dosages due to slower metabolism and increased sensitivity to side effects. It’s essential to monitor for signs of over-sedation or respiratory depression, especially in patients with pre-existing conditions like COPD or sleep apnea.
A persuasive argument for combining these drugs lies in their synergistic effects. Muscle relaxers target hypertonicity and spasms, while painkillers address nociceptive pain. Together, they can provide more comprehensive relief than either drug alone, particularly in acute conditions like lower back strain. However, this approach is not without risks. Both classes can impair cognitive function, making activities like driving hazardous. Patients should be advised to avoid alcohol and other CNS depressants while on these medications, as the interaction can be life-threatening.
Comparatively, the overlap between muscle relaxers and opioid painkillers is more complex. While opioids like hydrocodone are potent analgesics, their combination with muscle relaxers like tizanidine can lead to severe hypotension or respiratory failure. Such combinations are generally reserved for severe cases and require close monitoring. Non-opioid alternatives, such as the muscle relaxer/NSAID pairing, are often preferred for their safer profile, though even these carry risks of gastrointestinal bleeding or renal impairment with prolonged use.
In practice, the key to safe co-administration lies in individualized treatment. Factors like age, comorbidities, and concurrent medications must be considered. For example, patients on SSRIs or MAOIs may experience serotonin syndrome when taking certain muscle relaxers, necessitating alternative therapies. Practical tips include taking medications at different times to minimize peak interactions and using non-pharmacological adjuncts like physical therapy to reduce reliance on drugs. Ultimately, while muscle relaxers and painkillers are not the same, their strategic overlap can enhance treatment outcomes when managed thoughtfully.
Effective Natural Muscle Relaxers: Soothing Remedies for Human Relief
You may want to see also
Frequently asked questions
No, muscle relaxers and painkillers are different types of medications. Muscle relaxers target muscle spasms and tension, while painkillers (analgesics) primarily relieve pain.
Muscle relaxers may indirectly reduce pain by easing muscle spasms, but they are not designed to treat pain directly like painkillers do.
No, they have different side effects. Muscle relaxers often cause drowsiness and dizziness, while painkillers may lead to nausea, constipation, or stomach issues.
They can be taken together under a doctor’s supervision, but combining them increases the risk of side effects, such as excessive drowsiness or respiratory depression.
It depends on the cause of the pain. Muscle relaxers are better for muscle spasms, while painkillers are more effective for general pain relief. Consult a doctor for the best option.































