Skeletal muscle relaxants are a class of medications primarily used to alleviate muscle spasms and pain associated with musculoskeletal conditions. While they are effective in reducing muscle tension and improving mobility, there is often confusion regarding whether these drugs are classified as narcotics. Narcotics, typically referring to opioid pain relievers, act on the central nervous system to alleviate pain and induce sedation. In contrast, skeletal muscle relaxants work by targeting the nervous system to reduce muscle activity, but they do not possess the same opioid properties or addiction potential. Therefore, skeletal muscle relaxants are not considered narcotics, though they may share some sedative effects and require careful use under medical supervision.
| Characteristics | Values |
|---|---|
| Classification | Skeletal muscle relaxants are not classified as narcotics. |
| Mechanism of Action | Act on the central nervous system (CNS) or neuromuscular junction to reduce muscle tone, but do not bind to opioid receptors. |
| Addiction Potential | Generally lower addiction potential compared to narcotics, though some (e.g., carisoprodol) may have abuse potential. |
| Examples | Cyclobenzaprine, tizanidine, baclofen, carisoprodol, methocarbamol. |
| DEA Scheduling | Most are not scheduled, but carisoprodol is a Schedule IV controlled substance in the U.S. due to abuse concerns. |
| Pain Relief | Primarily treat muscle spasms, not pain; narcotics are used for pain relief. |
| Side Effects | Drowsiness, dizziness, dry mouth (common); narcotics cause euphoria, respiratory depression, and constipation. |
| Medical Use | Used for musculoskeletal conditions (e.g., back pain, injury); narcotics are for severe pain management. |
| Withdrawal Symptoms | Minimal withdrawal risk; narcotics have significant withdrawal symptoms (e.g., anxiety, nausea, cravings). |
| Legal Status | Widely available with prescription; narcotics are strictly regulated due to high abuse potential. |
Explore related products






What You'll Learn
![]()
Definition of skeletal muscle relaxants
Skeletal muscle relaxants are a class of medications designed to alleviate muscle spasms, stiffness, and pain by acting on the central nervous system or directly on muscle fibers. Unlike narcotics, which primarily target the brain’s opioid receptors to relieve pain, these relaxants modulate nerve signals or muscle function to reduce tension. Common examples include baclofen, cyclobenzaprine, and tizanidine, each with distinct mechanisms and applications. For instance, baclofen mimics GABA, an inhibitory neurotransmitter, to suppress nerve activity, while tizanidine reduces muscle tone without causing sedation at low doses (2–4 mg). Understanding their definition clarifies why they are not classified as narcotics, despite sometimes being prescribed alongside opioids for comprehensive pain management.
To use skeletal muscle relaxants effectively, follow specific dosage guidelines tailored to age, condition, and severity. Adults typically start with 5–10 mg of cyclobenzaprine up to three times daily, while tizanidine is dosed at 2–4 mg every 6–8 hours, not exceeding 36 mg in 24 hours. Elderly patients or those with hepatic impairment may require lower doses due to slower metabolism. For acute conditions like lower back pain, a short-term regimen of 3–7 days is standard, as prolonged use increases risks of dependence and side effects like dizziness or drowsiness. Always pair these medications with physical therapy or rest for optimal recovery, as they address symptoms, not underlying causes.
A critical distinction between skeletal muscle relaxants and narcotics lies in their mechanism and potential for misuse. While narcotics like oxycodone bind to opioid receptors to block pain perception, muscle relaxants act on the spinal cord or muscles directly, reducing spasticity without altering pain thresholds. This difference minimizes the euphoric effects associated with narcotics, lowering the risk of addiction. However, muscle relaxants can still cause sedation and impairment, necessitating caution during activities like driving. For example, tizanidine’s half-life of 2–4 hours requires careful timing to avoid peak drowsiness, whereas narcotics’ longer-acting formulations may provide sustained pain relief but higher abuse potential.
In practice, skeletal muscle relaxants are often prescribed for musculoskeletal conditions such as sprains, strains, or spinal injuries, where muscle spasms exacerbate pain. They are not first-line treatments but are reserved for cases unresponsive to NSAIDs or acetaminophen. Patients should be educated on potential interactions—for instance, combining tizanidine with fluvoxamine can lead to dangerous drops in blood pressure. Additionally, abrupt discontinuation of certain relaxants, like baclofen, can trigger withdrawal symptoms, emphasizing the need for gradual tapering. By adhering to these principles, clinicians can harness the benefits of muscle relaxants while mitigating risks, ensuring they remain distinct from narcotics in both function and safety profile.
Stretching Techniques for Muscle Relaxation: Unwind and Release Tension
You may want to see also
Explore related products






![]()
Narcotic classification criteria
Skeletal muscle relaxants, such as cyclobenzaprine and baclofen, are often prescribed to alleviate muscle spasms and pain. However, their classification as narcotics remains a subject of debate. To understand this, one must first examine the criteria used to classify substances as narcotics. Narcotics are typically defined as substances that act on the central nervous system to relieve pain and induce sleep, often with a high potential for abuse and dependence. The U.S. Drug Enforcement Administration (DEA) classifies narcotics under Schedule II, III, IV, or V of the Controlled Substances Act, depending on their medical utility and abuse potential. For instance, opioids like morphine and oxycodone are classic examples of narcotics due to their potent analgesic effects and significant risk of addiction.
The classification process involves evaluating a substance’s pharmacological properties, therapeutic use, and potential for misuse. Skeletal muscle relaxants, while affecting the central nervous system, primarily target muscle spasticity rather than pain relief. For example, cyclobenzaprine is structurally similar to tricyclic antidepressants and does not bind to opioid receptors, a hallmark of narcotics. Similarly, baclofen acts on GABA receptors to reduce muscle tone but lacks the euphoric effects associated with opioid narcotics. This distinction is crucial, as it influences prescribing practices and regulatory oversight. Physicians must consider these differences to avoid over-classification, which could limit patient access to necessary treatments.
From a regulatory standpoint, the DEA’s scheduling criteria provide a framework for determining whether a substance qualifies as a narcotic. Schedule II drugs, like fentanyl, have a high potential for abuse and severe dependence, while Schedule V drugs, such as cough suppressants with limited opioids, pose the lowest risk. Skeletal muscle relaxants are generally classified as Schedule III or IV, indicating a lower potential for abuse compared to opioids. For instance, carisoprodol, a muscle relaxant with mild sedative effects, was reclassified from Schedule IV to III in 2020 due to concerns about misuse when combined with opioids. This reclassification highlights the importance of monitoring drug interactions and patient history to prevent abuse.
Practically, understanding narcotic classification criteria helps healthcare providers make informed decisions. For patients over 65, lower dosages of muscle relaxants are often recommended due to increased sensitivity and risk of side effects. For example, cyclobenzaprine dosages typically range from 5 to 10 mg, taken up to three times daily, but elderly patients may start at 5 mg once daily. Additionally, providers should educate patients about the differences between muscle relaxants and narcotics to manage expectations and reduce stigma. Clear communication ensures patients understand that muscle relaxants are not opioids and do not carry the same risks of addiction or withdrawal.
In conclusion, while skeletal muscle relaxants share some central nervous system effects with narcotics, they do not meet the pharmacological or regulatory criteria for narcotic classification. Their distinct mechanisms of action, lower abuse potential, and therapeutic focus on muscle spasticity set them apart from opioids. By adhering to classification criteria and tailoring prescriptions to individual patient needs, healthcare providers can optimize treatment outcomes while minimizing risks. This nuanced understanding is essential for both clinical practice and regulatory compliance.
Hydrocodone as a Muscle Relaxer: Facts, Uses, and Risks Explained
You may want to see also
Explore related products






![]()
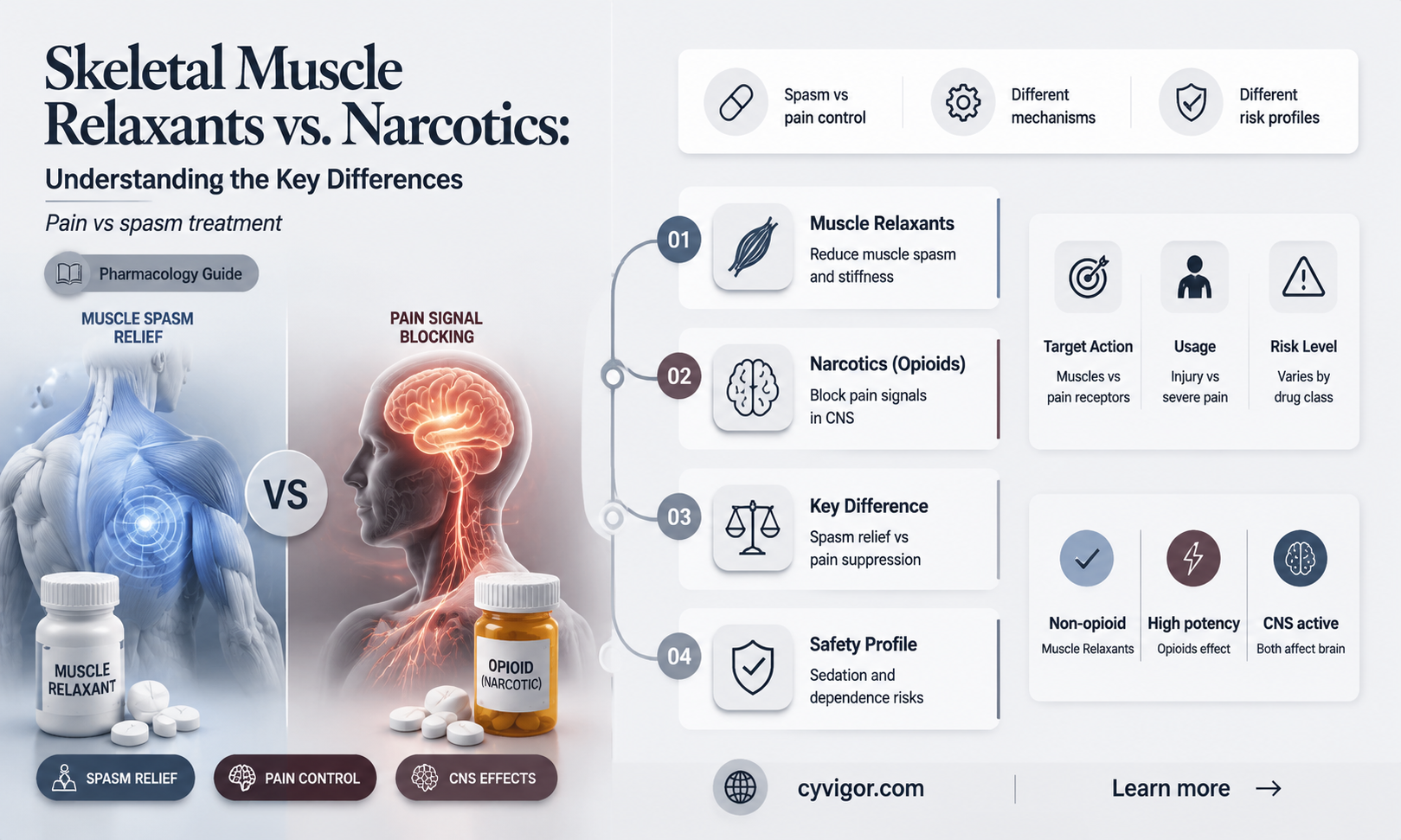
Mechanism of action differences
Skeletal muscle relaxants and narcotics operate through distinct mechanisms, targeting different physiological pathways to achieve their effects. Narcotics, such as opioids, primarily act on the central nervous system (CNS) by binding to opioid receptors, modulating pain perception and producing analgesia and euphoria. In contrast, skeletal muscle relaxants work either centrally or peripherally. Centrally acting relaxants, like cyclobenzaprine and tizanidine, depress the CNS by inhibiting neuronal activity in the brain stem or spinal cord, reducing muscle tone without directly affecting muscle fibers. Peripheral relaxants, such as dantrolene, act directly on muscle fibers by interfering with calcium release in the sarcoplasmic reticulum, thereby inhibiting muscle contraction.
Consider the example of tizanidine, a centrally acting muscle relaxant. It mimics the action of inhibitory neurotransmitters like GABA, reducing nerve impulses that lead to muscle spasms. This mechanism contrasts sharply with opioids like morphine, which primarily alter pain signaling in the brain and spinal cord. While both classes of drugs can induce sedation, the root cause differs: opioids suppress the perception of pain and induce euphoria, whereas muscle relaxants reduce muscle activity and CNS excitability. This distinction is critical for clinicians when prescribing, as combining these drugs can potentiate CNS depression, increasing risks like respiratory depression or excessive sedation.
For practical application, understanding these mechanisms guides dosing and patient monitoring. Centrally acting muscle relaxants are typically initiated at low doses—for instance, cyclobenzaprine at 5 mg/day—and titrated upward to minimize side effects like dizziness or drowsiness. Narcotics, on the other hand, require careful titration to balance analgesia with risks like tolerance or dependence. Patients over 65 or those with hepatic impairment may require lower doses of both classes due to reduced drug metabolism. Always assess for drug interactions, particularly with CYP1A2 inhibitors (e.g., ciprofloxacin) for tizanidine, which can elevate its plasma levels and toxicity risk.
A comparative analysis highlights the importance of mechanism-based prescribing. While narcotics are indispensable for severe pain, their addictive potential and systemic effects limit their use. Muscle relaxants, though effective for acute musculoskeletal conditions like lower back pain, are not without risks—centrally acting agents can impair cognitive function, while dantrolene carries a rare but serious risk of hepatotoxicity. Clinicians must weigh these factors, often opting for muscle relaxants in patients with contraindications to opioids or those requiring targeted muscle spasm relief.
In conclusion, the mechanism of action differences between skeletal muscle relaxants and narcotics underscore their distinct roles in therapy. By targeting muscle tone versus pain perception, these drugs offer complementary but non-interchangeable benefits. Practitioners should leverage this knowledge to optimize treatment, ensuring efficacy while minimizing adverse effects. For instance, pairing a centrally acting relaxant with physical therapy can enhance functional recovery in acute sprains, whereas narcotics remain reserved for pain management when alternatives are insufficient. This nuanced approach ensures patient safety and treatment success.
Does Detrol Relax Muscles? Exploring Its Effects and Uses
You may want to see also
Explore related products






![]()
Addiction potential comparison
Skeletal muscle relaxants, often prescribed for acute musculoskeletal conditions, are not classified as narcotics but carry their own risks of dependence and misuse. Unlike opioids, which act on the central nervous system to produce euphoria, muscle relaxants primarily target the nervous system to reduce muscle spasms. However, their sedative effects can lead to psychological dependence, particularly in individuals with a history of substance use disorders. For instance, cyclobenzaprine (Flexeril) and carisoprodol (Soma) are frequently cited in reports of misuse due to their calming effects, which users may seek to replicate.
When comparing addiction potential, opioids like oxycodone or hydrocodone remain significantly more addictive due to their direct activation of the brain’s reward system. Opioids are Schedule II controlled substances, indicating a high potential for abuse, while most muscle relaxants are Schedule IV, reflecting a lower but still present risk. Dosage plays a critical role here: carisoprodol, for example, is often prescribed at 350 mg three times daily, but exceeding this can amplify sedative effects and increase misuse risk. In contrast, opioids are typically dosed more cautiously due to their higher addiction profile.
Age and medical history are crucial factors in assessing addiction risk. Younger adults (18–25) and individuals with a history of substance abuse are more likely to misuse muscle relaxants, often combining them with alcohol or opioids to enhance effects. For older adults (65+), the risk lies in prolonged use, as chronic pain conditions may lead to physical dependence. Practical advice includes limiting prescriptions to 2–3 weeks for acute conditions and monitoring patients with a history of addiction closely.
To minimize addiction potential, healthcare providers should prioritize non-pharmacological interventions, such as physical therapy or heat therapy, before prescribing muscle relaxants. If medication is necessary, alternatives like tizanidine (Zanaflex), which has less sedative effects, may be preferable. Patients should be educated on the risks of misuse and instructed to avoid alcohol and other central nervous system depressants while taking these medications. Clear communication and follow-up appointments are essential to ensure safe use and prevent dependence.
In summary, while skeletal muscle relaxants are not narcotics, their addiction potential warrants careful consideration. Opioids remain the more addictive class, but muscle relaxants pose a unique risk due to their sedative properties and potential for misuse. Tailoring prescriptions to individual risk factors, emphasizing short-term use, and promoting non-pharmacological alternatives are key strategies to mitigate dependence. Awareness and proactive management by both providers and patients are critical in navigating this comparison.
How Much Muscle Relaxer is Too Much? Understanding Safe Dosages
You may want to see also
Explore related products

![Marihuana / Narcotic (Forbidden Fruit Vol. 4) [Blu-ray]](https://m.media-amazon.com/images/I/81Wog2yhQDL._AC_UY218_.jpg)




![]()
Medical use vs. narcotic misuse
Skeletal muscle relaxants, such as cyclobenzaprine and tizanidine, are primarily prescribed to alleviate acute musculoskeletal pain and discomfort. These medications work by acting on the central nervous system to reduce muscle spasms and improve mobility. When used as directed, they offer significant relief for conditions like lower back pain, neck strain, and post-surgical stiffness. For instance, a typical dose of cyclobenzaprine is 5–10 mg taken up to three times daily, with adjustments based on patient response and tolerance. Adherence to prescribed dosage and duration is critical, as these drugs are intended for short-term use, usually no longer than 2–3 weeks.
Despite their therapeutic benefits, skeletal muscle relaxants carry a risk of misuse due to their sedative effects and potential for psychological dependence. Unlike opioids, they are not classified as narcotics, but their misuse can still lead to harmful outcomes. Individuals may misuse these drugs to achieve relaxation or euphoria, often combining them with alcohol or other central nervous system depressants. This behavior amplifies the risk of respiratory depression, dizziness, and impaired judgment. For example, tizanidine, when taken in excess of its recommended 2–4 mg dose, can cause severe hypotension and sedation. Misuse is particularly concerning among adolescents and young adults, who may perceive these medications as less dangerous than opioids.
The line between medical use and narcotic-like misuse blurs when patients self-medicate or exceed prescribed limits. Healthcare providers must educate patients about the risks and monitor for signs of dependency, such as frequent requests for early refills or reported "lost" prescriptions. Patients should be instructed to avoid abrupt discontinuation, as this can lead to withdrawal symptoms like nausea, headache, and tachycardia. Tapering the dose under medical supervision is recommended for those who have used the medication long-term. Additionally, alternative therapies like physical therapy, heat application, and stretching exercises should be encouraged to minimize reliance on pharmacological interventions.
Comparatively, the misuse of skeletal muscle relaxants differs from opioid misuse in its motivations and consequences. While opioids are often sought for their potent analgesic and euphoric effects, muscle relaxants are more commonly misused for their anxiolytic and sedative properties. However, both classes of drugs share the potential for dependency and adverse interactions with other substances. Policymakers and healthcare providers must address this issue through stricter prescription monitoring programs and increased public awareness. For instance, integrating drug screening into routine care can help identify at-risk individuals early, allowing for timely intervention and support.
In conclusion, while skeletal muscle relaxants are valuable tools for managing acute musculoskeletal conditions, their potential for misuse necessitates cautious prescribing practices and patient education. By understanding the distinctions between medical use and narcotic-like misuse, healthcare professionals can optimize therapeutic outcomes while minimizing risks. Patients, too, play a crucial role in adhering to prescribed regimens and exploring non-pharmacological alternatives. Together, these efforts can ensure that these medications remain a safe and effective option for those in need.
Muscle Relaxers Post-Anesthesia: Timing and Recovery Explained
You may want to see also
Frequently asked questions
No, skeletal muscle relaxants are not classified as narcotics. They are a separate class of medications used to relieve muscle spasms and pain.
No, skeletal muscle relaxants primarily target muscle spasms and tension, while narcotics (opioids) are used for pain relief and can cause sedation and euphoria.
While some skeletal muscle relaxants can cause dependence if misused, they are generally less addictive than narcotics and are not classified as controlled substances in the same way.
No, skeletal muscle relaxants are typically prescribed for muscle spasms, stiffness, or injuries, whereas narcotics are prescribed for moderate to severe pain.
No, skeletal muscle relaxants do not show up as narcotics in standard drug tests, as they are chemically distinct and not part of the opioid family.