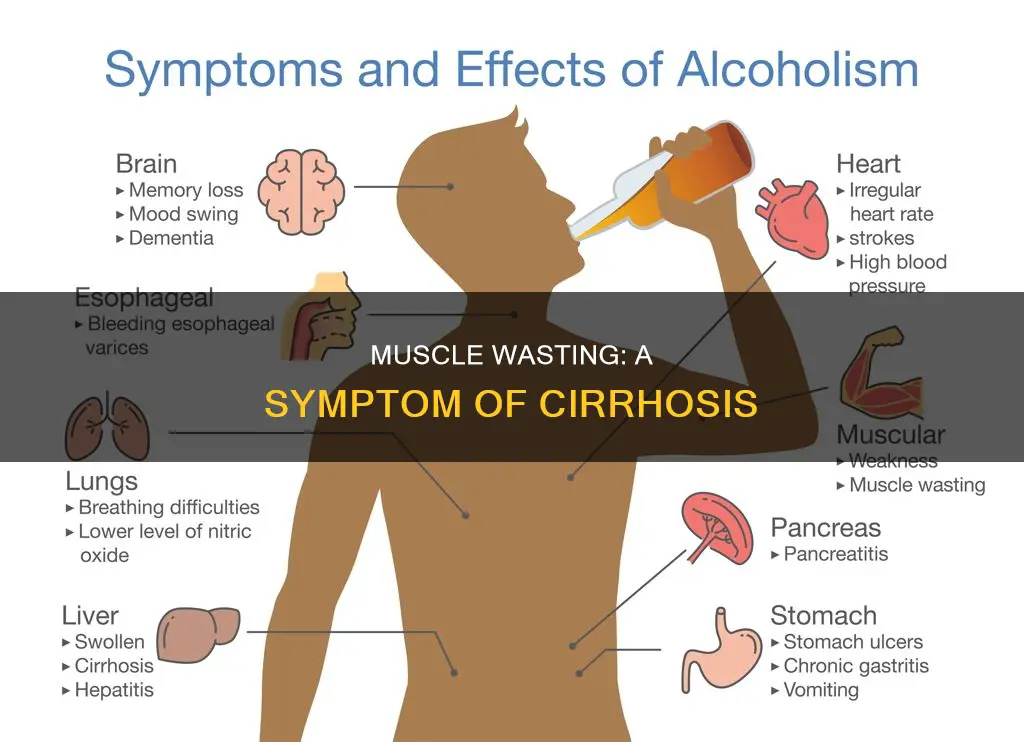
Cirrhosis is a state of anabolic resistance, which can lead to muscle wasting or sarcopenia. Sarcopenia is a condition of low muscle mass, quality, and strength, and is associated with adverse clinical outcomes, including reduced quality of life, increased mortality, and post-transplant complications. It is estimated that muscle depletion affects approximately 40% of patients with cirrhosis, and its prevalence increases with disease severity. Several studies have found that muscle wasting is independently associated with mortality in patients with cirrhosis.
| Characteristics | Values |
|---|---|
| What is muscle wasting? | Muscle wasting is defined as the progressive and generalized loss of muscle mass. |
| What is cirrhosis? | Cirrhosis is a state of anabolic resistance. |
| What is sarcopenia? | Sarcopenia is a word coined in 1988 to describe loss of skeletal muscle mass and function. |
| How is muscle wasting assessed? | Muscle wasting is assessed by using the computed tomography cross-sectional area of skeletal muscles at the level of the third lumbar vertebra. |
| Prevalence of muscle wasting in cirrhosis patients | Muscle depletion is found in approximately 40% of patients with cirrhosis. |
| Can cirrhosis cause muscle wasting? | Yes, cirrhosis is believed to be a state of anabolic resistance and is a risk factor for the loss of muscle mass. |
| Treatment for muscle wasting in cirrhosis patients | Nutritional supplementation alone is not effective. High doses of leucine and potentially other branched-chain amino acids and long-term ammonia-lowering measures may be beneficial. |
Explore related products





What You'll Learn
- Muscle wasting is associated with mortality in cirrhosis patients
- Sarcopenia, or loss of muscle mass, is common in cirrhosis patients
- Nutritional interventions and exercise may improve survival rates
- CT and MRI scans are the best methods to measure muscle mass
- Cirrhosis is a state of anabolic resistance
![]()
Muscle wasting is associated with mortality in cirrhosis patients
Cirrhosis is a state of anabolic resistance and a risk factor for the loss of muscle mass. Sarcopenia, defined as a low level of muscle mass, occurs in patients with cirrhosis. Sarcopenia is associated with aging, but it can also be present as a result of chronic diseases and malignancies. Sarcopenia was more prevalent in alcoholic liver cirrhosis compared to other etiologies.
Muscle wasting is defined as the progressive and generalized loss of muscle mass. It is considered the main criterion to diagnose sarcopenia, along with a decline in muscle function (loss of strength or physical performance). Muscle depletion is a common feature of chronic liver disease found in approximately 40% of patients with cirrhosis. Its prevalence increases along with disease severity.
Several studies have assessed the impact of muscle wasting on the overall survival of patients awaiting liver transplantation, and there is a general agreement that decreased muscle size assessed by CT scan is an independent predictor of mortality in cirrhosis. Nutritional interventions and exercise aiming to correct muscle depletion may improve the survival of patients with cirrhosis, but further investigation is needed.
Univariate Cox analysis associated mortality in cirrhosis patients with ascites, encephalopathy, level of bilirubin, international normalized ratio, level of creatinine, level of albumin, serum level of sodium, Model for End-Stage Liver Disease (MELD) score, Child-Pugh score, and sarcopenia. However, only Child-Pugh and MELD scores and sarcopenia were independently associated with mortality in multivariate Cox analysis. The median survival time for patients with sarcopenia was 19 ± 6 months, compared to 34 ± 11 months for nonsarcopenic patients.
Gastritis and Muscle Weakness: Is There a Link?
You may want to see also
Explore related products





![]()
Sarcopenia, or loss of muscle mass, is common in cirrhosis patients
Sarcopenia, or loss of muscle mass, is a common complication in patients with cirrhosis. It is a multifactorial chronic condition that increases the risk of morbidity and mortality in those with liver disease. Sarcopenia is characterised by a reduction in muscle mass, strength, and function. The condition is often underdiagnosed and undertreated, with a prevalence of 40-70% in cirrhosis patients.
The aetiology of sarcopenia in cirrhosis patients is complex and influenced by various factors. Alcohol-related liver disease (ARLD) is the most common cause, with non-alcoholic fatty liver disease (NAFLD) also contributing significantly due to the obesity and diabetes epidemic. Other factors include metabolic changes, insufficient nutrient intake, physical inactivity, hormonal imbalances, and inflammation. The primary cause of muscle depletion is ageing, but sarcopenia can also be a secondary condition associated with many chronic diseases.
The connection between cirrhosis and sarcopenia is well-established. Cirrhosis is a catabolic state where muscle protein breakdown exceeds synthesis, leading to sarcopenia. Hepatic encephalopathy, a consequence of impaired liver function, also contributes to sarcopenia by causing physical inactivity and upregulating myostatin, which inhibits protein synthesis and muscle regeneration. Additionally, the muscle is a key site for removing excess ammonia, depleting stores of branched-chain amino acids (BCAAs) needed for protein synthesis. Insulin resistance, common in cirrhosis, further exacerbates the condition by reducing protein synthesis and increasing protein catabolism.
The diagnosis and assessment of sarcopenia in cirrhosis pose challenges. While computed tomography (CT) and magnetic resonance imaging (MRI) are considered the gold standards for research, they are limited in clinical practice due to cost and radiation exposure concerns. Other techniques such as anthropometry, bioelectrical impedance analysis (BIA), dual-energy X-ray absorptiometry (DXA), and ultrasound have been used to quantify muscle mass in cirrhosis. However, there is no agreed-upon reference standard for diagnosing sarcopenia in cirrhosis, making it difficult to compare results across studies.
The management of sarcopenia in cirrhosis aims to ameliorate complications and improve patient outcomes. Early recognition and tailored interventions, including nutritional support, exercise, and targeted therapies such as myostatin inhibitors, are recommended. High-protein diets and a combination of aerobic and resistance exercises can help manage sarcopenia. Pharmacological interventions, such as vitamin D and testosterone in males, are also potential therapeutic options, although further research is needed.
Lipomas and Muscle Spasms: Is There a Connection?
You may want to see also
Explore related products






![]()
Nutritional interventions and exercise may improve survival rates
Cirrhosis is a state of anabolic resistance and a risk factor for muscle wasting. Muscle depletion is a common feature of chronic liver disease, found in approximately 40% of cirrhosis patients. Sarcopenia, a term coined to describe the loss of skeletal muscle mass and function, is often observed in cirrhotic patients. It is considered one of the major complications of end-stage liver disease, with its incidence increasing as the disease progresses.
Several studies have shown that nutritional interventions and exercise can improve survival rates in cirrhosis patients. Nutritional management includes sufficient dietary intake and improved nutrient metabolism. For example, a randomised clinical trial found that a nutritional intervention with 1.0-1.5 g of vegetable protein per kg per day for six months improved neuropsychiatric performance in patients with minimal hepatic encephalopathy and decreased the risk of developing overt hepatic encephalopathy. Vegetable protein may be preferable to animal protein as it has fewer sulphur-containing amino acids and more arginine and ornithine. Another study found that a 14-day casein-vegetable, high-protein, high-calorie diet improved mental performance and decreased ammonia levels in patients with overt hepatic encephalopathy.
Exercise management can increase skeletal muscle volume and strength and improve insulin resistance. A recent survey of compensated LC patients recommended the following exercise regimen: walking 5,000 or more steps per day with a total caloric intake of approximately 30 kcal/ideal body weight. The authors claimed that this regimen could maintain and increase skeletal muscle volume in LC patients. Another randomised pilot study examined whether an exercise program combined with leucine supplementation (10 g/d) could improve patient outcomes. The intervention group showed improved exercise capacity, increased lower thigh circumference, and improved health-related quality of life.
In summary, nutritional interventions and exercise may improve survival rates in cirrhosis patients by reducing muscle wasting and improving muscle function. However, further research is needed to fully understand the impact of these interventions on patient outcomes.
Muscle Tightness: A Surprising Cause of Back Pain?
You may want to see also
Explore related products






![]()
CT and MRI scans are the best methods to measure muscle mass
Cirrhosis is a state of anabolic resistance, and liver cirrhosis is a risk factor for the loss of muscle mass. Muscle wasting is defined as the progressive and generalized loss of muscle mass. Muscle depletion is a common feature of chronic liver disease, found in approximately 40% of patients with cirrhosis.
Computed tomography (CT) and magnetic resonance imaging (MRI) scans are considered the gold standards for estimating muscle mass for research purposes. They can accurately distinguish between fat and other soft tissues, provide quantitative measurements of skeletal muscle size, and are not biased by fluid retention. CT scans are widely used due to their reasonable cost, high scan speed, and wide availability. MRI scans, on the other hand, are becoming more popular for abdominal scans due to their improved tissue contrast and reduced radiation exposure.
CT and MRI scans can be used to quantify muscle mass and quality, and to assess muscle properties such as size, mass, density, composition, and adipose tissue infiltration. While CT scans are faster, more accessible, and cheaper, MRI scans can provide a more detailed map of the fat fraction in the muscle. The choice between CT and MRI depends on the specific requirements of the examination.
Cross-sectional imaging with CT and MRI has been used to measure abdominal muscle mass, with total abdominal muscle area (TAMA) being a more reliable biomarker than total psoas muscle area (TPA) in terms of inter-scan and inter-reader agreement. The L3 level is commonly used for measurements as it reflects whole-body muscle mass well.
In summary, CT and MRI scans are the most accurate methods for measuring muscle mass, especially in cases of muscle wasting associated with cirrhosis. However, further research is needed to fully validate the use of these techniques and improve standardization.
Bone Cancer and Muscle Pain: Is There a Link?
You may want to see also
Explore related products






![]()
Cirrhosis is a state of anabolic resistance
Cirrhosis is a chronic liver disease that can lead to muscle wasting, which is a significant complication of end-stage liver disease. Muscle wasting, or sarcopenia, is characterised by a decrease in muscle size and an increase in fat accumulation. It is associated with increased mortality and decreased quality of life.
The liver-muscle axis is disrupted in cirrhosis, causing anabolic resistance and muscle wasting. Hyperammonemia, or increased ammonia uptake in skeletal muscle, leads to signalling perturbations, mitochondrial dysfunction, and impaired ribosomal function, all of which contribute to anabolic resistance. Additionally, cirrhosis is a state of accelerated starvation with impaired protein synthesis, further contributing to anabolic resistance and muscle loss.
The mechanisms of cirrhotic muscle wasting are complex and not fully understood. Some studies have suggested that resistance exercise may benefit people with cirrhosis, but the anabolic resistance may limit the anticipated responses. Nutritional interventions have shown modest to no benefit, and it is unclear whether anabolic resistance extends to physical activity.
Some interventions, such as a late evening snack, have shown promise in improving anabolic resistance and reversing sarcopenia in people with cirrhosis. Overall, more research is needed to understand the impact of exercise and nutritional interventions on muscle wasting in people with cirrhosis and how to optimise responses to anabolic stimuli.
Muscle Knots and MS: What's the Link?
You may want to see also
Frequently asked questions
Muscle wasting is defined as the progressive and generalized loss of muscle mass. It is considered the main criterion to diagnose sarcopenia, which is accompanied by a decline in muscle function.
Yes, muscle wasting is a common feature of chronic liver disease and is found in approximately 40% of patients with cirrhosis. Sarcopenia, or loss of skeletal muscle, occurs in the majority of patients with liver disease.
The exact causes of muscle wasting in people with cirrhosis are not yet fully understood. However, it is believed that cirrhosis leads to anabolic resistance, which contributes to muscle loss. Other factors include disordered energy metabolism, malnutrition, and physical inactivity.
Computed tomography (CT) scans and magnetic resonance imaging (MRI) are considered the gold standards for assessing muscle mass in people with cirrhosis. These techniques accurately distinguish between muscle, fat, and other soft tissues and are not biased by fluid retention.
Currently, there are no effective therapies to prevent or reverse sarcopenia in people with cirrhosis. Nutritional supplementation alone is generally ineffective. However, high doses of leucine, branched-chain amino acids, and long-term ammonia-lowering measures may be beneficial. Exercise may also help combat muscle wasting, but more research is needed.