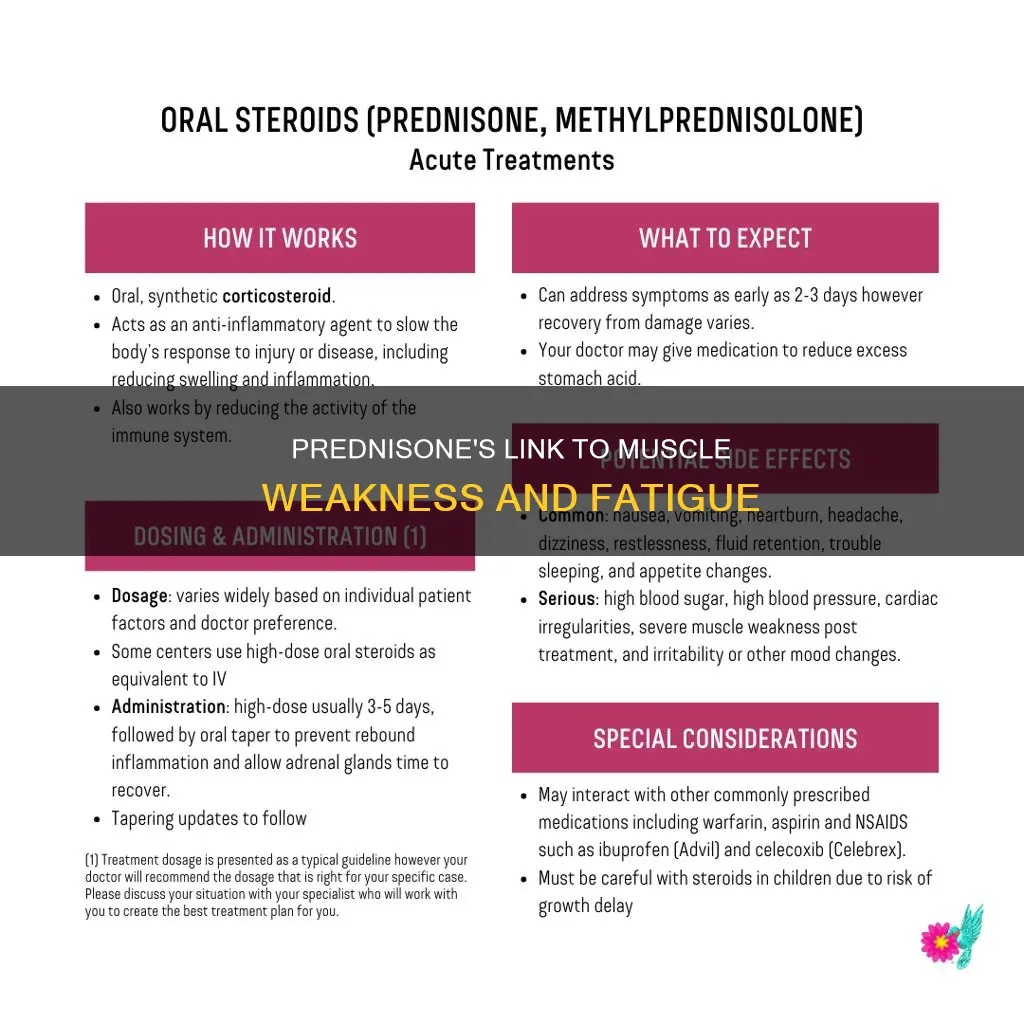
Prednisone is a corticosteroid (cortisone-like medicine or steroid) that is used to treat inflammation, severe allergies, adrenal problems, arthritis, asthma, blood or bone marrow problems, endocrine problems, eye or vision problems, stomach or bowel problems, lupus, skin conditions, kidney problems, ulcerative colitis, and flare-ups of multiple sclerosis. While prednisone is effective in providing relief for inflamed areas of the body, it can also cause muscle weakness and wasting when taken long-term. This is a significant problem for people who take steroids for many chronic conditions, and can often result in patients having to stop steroid treatments.
Explore related products






What You'll Learn
- Prolonged prednisone use can cause muscle weakness
- Prednisone doses of 30 mg/day or more increase the risk of myopathy
- Fluorinated steroids are more toxic and cause weakness more frequently
- Prednisone may cause muscle wasting when taken long-term
- Prednisone can cause acute myopathy resulting in paralysis and respiratory failure
![]()
Prolonged prednisone use can cause muscle weakness
Corticosteroid-induced myopathy typically affects the pelvic girdle muscles and is associated with muscle weakness and atrophy without pain. The onset of weakness can occur within weeks to years of starting corticosteroid administration, and it can develop with prednisone doses of 30 mg/day or more. However, the incidence of corticosteroid-induced weakness does not always correlate with the duration of treatment or dosage. Fluorinated steroids, such as dexamethasone and triamcinolone, are more likely to induce myopathy than non-fluorinated steroids like prednisone.
The muscle weakness associated with prolonged prednisone use can manifest in several ways. Patients may experience progressive proximal muscle weakness in the upper and lower limbs, making it difficult to rise from chairs, climb stairs, or perform overhead activities. In some cases, acute myopathy may occur, resulting in prolonged paralysis and respiratory failure. This is more common in patients receiving high doses of intravenous corticosteroids, especially when combined with neuromuscular blocking agents.
The treatment for corticosteroid-induced myopathy primarily involves reducing or discontinuing the use of corticosteroids. For patients unable to taper off steroids, switching from fluorinated glucocorticoids to non-fluorinated alternatives like prednisone or hydrocortisone may be considered. Physical therapy, including resistance and aerobic exercise, has also been shown to prevent and treat steroid-induced myopathy. While corticosteroid-induced myopathy is almost always reversible, recovery can take several weeks to a year.
It is important to note that prednisone is a valuable medication used to treat various conditions, including inflammation, severe allergies, adrenal problems, arthritis, asthma, and endocrine issues. When deciding to use prednisone, the potential risks must be weighed against the benefits it can provide. Additionally, weekly doses of prednisone have been found to promote muscle repair and improve muscle performance, suggesting that the frequency of administration may play a role in mitigating muscle weakness.
Constipation and Abdominal Strain: What's the Link?
You may want to see also
Explore related products

$8.88 $24.99





![]()
Prednisone doses of 30 mg/day or more increase the risk of myopathy
Corticosteroid-induced myopathy is a highly prevalent toxic non-inflammatory myopathy that occurs as an adverse effect of prolonged oral or intravenous glucocorticoid use. It was first described in 1932 by Harvey Cushing as part of a constellation of symptoms seen in Cushing syndrome. With the broader use of corticosteroids as therapeutic tools in the 1950s, corticosteroid-induced myopathy became a more well-known entity.
Prednisone doses of 30 mg/day or more have been associated with an increased risk of myopathy. However, the incidence of corticosteroid-induced weakness does not necessarily correlate with the duration of treatment or dosage. The occurrence of an associated myopathy in patients with Cushing's syndrome is approximately 50-80%. The incidence of exogenous corticosteroid myopathy is unknown, but it occurs almost twice as often in women than in men.
Fluorinated steroids seem to produce weakness and myopathy more frequently than non-fluorinated ones. Fluorinated glucocorticoids (triamcinolone, betamethasone, and dexamethasone) may be more toxic than non-fluorinated ones (prednisone, hydrocortisone). In most cases of acute corticosteroid myopathy, serum CK levels are increased and may be accompanied by myoglobinuria. Muscle biopsies show atrophy of all fiber types, as well as focal and diffuse necrosis.
Corticosteroid-induced myopathy is often overlooked as a diagnosis, as symptoms are sometimes attributed to the primary illness that the corticosteroid is treating. This prolongs the time to diagnosis and increases morbidity. Thus, a high index of suspicion is necessary when patients present with muscle weakness in any muscle group, especially the pelvic girdle, regardless of the dose, route, or duration of steroids.
Collagen and Muscle Spasms: What's the Link?
You may want to see also
Explore related products






![]()
Fluorinated steroids are more toxic and cause weakness more frequently
Prolonged administration of prednisone at a dose of 40-60 mg/day can cause muscle weakness and atrophy. Prednisone is a type of fluorinated glucocorticoid steroid. Fluorinated steroids, such as dexamethasone, triamcinolone, betamethasone, and beclomethasone, are more likely to induce myopathy than non-fluorinated steroids. They are more toxic and frequently cause weakness.
Fluorinated steroids have a greater propensity for producing weakness than non-fluorinated steroids. This is due to their ability to penetrate the skin better and their higher potency. The muscle weakness usually begins after the chronic use of high-dose steroids, although acute onset can also occur, especially after receiving intravenous fluorinated steroids.
Corticosteroid-induced myopathy is a toxic non-inflammatory myopathy caused by exogenous corticosteroid administration. It is a highly prevalent condition that occurs as an adverse effect of prolonged oral or intravenous glucocorticoid use. The condition typically affects pelvic girdle muscles and is associated with muscle weakness and atrophy without pain. Acute corticosteroid myopathy can result in prolonged paralysis and respiratory failure.
The diagnosis of corticosteroid-induced myopathy requires a high index of suspicion. It is confirmed when muscle weakness improves after 3 to 4 weeks of tapering steroids. Treatment options include steroid withdrawal, switching to non-fluorinated glucocorticoids, or alternate-day dosing. Physical therapy in the form of resistance and aerobic exercise can also help prevent and treat steroid-induced myopathy.
It is important to note that individual sensitivity plays a role in the development of corticosteroid-induced myopathy. The duration of therapy and steroid dose do not always correlate with the degree of weakness. However, high dosages and long durations of therapy increase the risk of developing this condition.
Muscle Strain and Tingling Hands: What's the Link?
You may want to see also
Explore related products






![]()
Prednisone may cause muscle wasting when taken long-term
Prednisone is a corticosteroid, or steroid, medication that provides relief for inflamed areas of the body. It is used to treat a number of conditions, including inflammation, severe allergies, adrenal problems, arthritis, asthma, endocrine problems, eye or vision problems, and skin conditions. While prednisone can be an effective treatment for these conditions, it is important to be aware of its potential side effects, particularly when taken long-term. One notable side effect is muscle weakness and wasting.
When taken in high doses (over 30 mg/day) or for prolonged periods, prednisone can cause corticosteroid-induced myopathy, a toxic non-inflammatory muscle disease. This condition typically affects the pelvic girdle muscles and is associated with muscle weakness and atrophy without pain. Patients may experience progressive proximal muscle weakness, finding it difficult to rise from chairs, climb stairs, and perform overhead activities. In some cases, acute myopathy may occur, resulting in prolonged paralysis and respiratory failure.
The risk of developing corticosteroid-induced myopathy may be influenced by the type of steroid used. Fluorinated steroids, such as dexamethasone and triamcinolone, are more likely to induce myopathy than non-fluorinated steroids like prednisone and hydrocortisone. However, it is important to note that prednisone itself can also cause muscle wasting when taken daily and long-term. This was observed in a study where mice with muscular dystrophy that received daily prednisone experienced muscle atrophy and wasting.
To mitigate the risk of muscle wasting and weakness associated with long-term prednisone use, weekly doses are recommended. Studies have shown that weekly doses of prednisone promote muscle repair and improve muscle performance. Additionally, physical therapy in the form of resistance and aerobic exercise can help prevent and treat steroid-induced myopathy. It is important for patients taking prednisone long-term to be aware of the potential side effects and to consult their doctors if they experience any muscle weakness or other concerning symptoms.
Diarrhea and Muscle Loss: What's the Connection?
You may want to see also
Explore related products


![]()
Prednisone can cause acute myopathy resulting in paralysis and respiratory failure
Prednisone is a corticosteroid or steroid medication that provides relief for inflamed areas of the body. It is used to treat inflammation, severe allergies, adrenal problems, arthritis, asthma, endocrine problems, eye or vision problems, and stomach or bowel problems, among other conditions. It is available only with a doctor's prescription.
While prednisone can be an effective treatment for many conditions, it is associated with certain side effects, one of which is muscle weakness. Prolonged administration of prednisone at a dose of 40-60 mg/day can lead to corticosteroid-induced myopathy, a toxic non-inflammatory myopathy. This condition is characterised by muscle weakness and atrophy without associated pain, typically affecting the pelvic girdle muscles. The onset of weakness can occur within weeks to years of starting corticosteroid therapy.
In addition to causing chronic steroid myopathy, prednisone can also induce acute myopathy. Acute corticosteroid myopathy typically occurs within 5-7 days of starting treatment with high doses of corticosteroids. It can lead to prolonged paralysis and respiratory failure, particularly when high doses of intravenous corticosteroids are administered concomitantly with neuromuscular blocking agents. This form of acute quadriplegic myopathy can result in severe proximal muscle weakness and respiratory failure.
The risk of developing steroid-induced myopathy may be higher in patients with severe asthma who use oral steroids. Additionally, fluorinated steroids, such as dexamethasone and triamcinolone, are more likely to induce myopathy than non-fluorinated steroids like prednisone. However, it is important to note that prednisone doses of 30 mg/day or more have been associated with an increased risk of myopathy.
If you are experiencing muscle weakness or other side effects while taking prednisone, it is important to consult your doctor or healthcare provider. They can advise on adjusting the dosage or explore alternative treatment options to alleviate the side effects.
Antibiotics and Muscle Tears: A Surprising Connection
You may want to see also
Frequently asked questions
Yes, prednisone can cause muscle weakness, especially when taken long-term.
Prednisone is a corticosteroid, a class of steroids that can cause a toxic non-inflammatory myopathy, resulting in muscle weakness and atrophy without pain.
Prednisone doses of 30 mg/day or more have been associated with an increased risk of myopathy. However, the incidence of corticosteroid-induced weakness does not always correlate with the duration of treatment or dosage.
Non-fluorinated glucocorticoids, such as prednisone or hydrocortisone, are less likely to induce myopathy than fluorinated glucocorticoids like dexamethasone, triamcinolone, and betamethasone.
Reducing or discontinuing the use of prednisone is the primary treatment for corticosteroid-induced myopathy. Physical therapy, including resistance and aerobic exercise, has also been shown to help prevent and treat this condition.