Sickle cell disease (SCD) is a genetic blood disorder characterized by abnormally shaped red blood cells that can lead to a variety of complications, including pain crises, organ damage, and infections. While muscle spasms are not typically considered a primary symptom of SCD, they can occur as a secondary effect of the disease. Muscle spasms in individuals with SCD may arise from factors such as dehydration, reduced blood flow to muscles due to sickle cell crises, or as a side effect of medications used to manage the condition. Additionally, chronic pain and physical inactivity associated with SCD can contribute to muscle stiffness and spasms. Understanding the relationship between sickle cell disease and muscle spasms is important for comprehensive patient care and management of associated symptoms.
Explore related products





What You'll Learn
- Neurological Complications: Sickle cell disease can lead to nerve damage, potentially causing muscle spasms
- Vasculopathy and Pain: Reduced blood flow from sickle cells may trigger muscle cramps and spasms
- Electrolyte Imbalance: Dehydration and anemia in sickle cell patients can disrupt electrolyte levels, causing spasms
- Musculoskeletal Stress: Chronic pain and reduced mobility in sickle cell disease may contribute to muscle spasms
- Medication Side Effects: Drugs used to manage sickle cell symptoms can sometimes induce muscle spasms as a side effect
![]()
Neurological Complications: Sickle cell disease can lead to nerve damage, potentially causing muscle spasms
Sickle cell disease (SCD) is a genetic disorder characterized by abnormal hemoglobin in red blood cells, leading to their rigid, sickle-like shape. These misshapen cells can cause blockages in blood vessels, impairing blood flow and oxygen delivery to tissues. One of the less-discussed but significant complications of SCD is its impact on the nervous system. Neurological complications arise due to repeated episodes of ischemia (reduced blood flow) and inflammation, which can damage nerves over time. This nerve damage, or neuropathy, is a critical aspect of understanding how SCD can contribute to muscle spasms.
The relationship between SCD and muscle spasms stems from the disease's ability to cause both central and peripheral nerve damage. Central nervous system complications, such as strokes or silent cerebral infarcts, can disrupt the brain's ability to regulate muscle function. Peripheral neuropathy, on the other hand, directly affects the nerves that control muscle movement. When these nerves are damaged, they may send erratic signals to muscles, leading to involuntary contractions or spasms. This is particularly evident in areas where blood flow is chronically compromised due to vaso-occlusive episodes, a hallmark of SCD.
Vaso-occlusive crises, a common feature of SCD, play a pivotal role in the development of neurological complications. During these episodes, sickle cells block blood vessels, depriving tissues of oxygen and nutrients. Prolonged or repeated ischemia can lead to nerve degeneration, making nerves more susceptible to dysfunction. Additionally, the inflammatory response triggered by these crises can exacerbate nerve damage, further increasing the likelihood of muscle spasms. Patients often report spasms in limbs or other muscle groups, which can be both painful and debilitating, impacting their quality of life.
Another mechanism linking SCD to muscle spasms involves the release of pro-inflammatory cytokines and oxidative stress. Chronic inflammation in SCD contributes to nerve damage by creating a toxic environment for nerve cells. Oxidative stress, resulting from the imbalance between free radicals and antioxidants, further compromises nerve integrity. These processes can alter the electrical conductivity of nerves, leading to abnormal muscle activity. Spasms may occur as a result of this dysregulated nerve signaling, highlighting the intricate connection between SCD, nerve damage, and muscular symptoms.
Managing neurological complications, including muscle spasms, in SCD requires a multifaceted approach. Pain management strategies, such as medications and physical therapy, can help alleviate symptoms. However, addressing the root cause involves preventing vaso-occlusive crises through hydration, infection prevention, and disease-modifying therapies like hydroxyurea or newer treatments such as voxelotor. Regular neurological monitoring is essential to detect early signs of nerve damage and intervene promptly. By understanding the neurological impact of SCD, healthcare providers can better support patients in managing complications like muscle spasms and improving overall outcomes.
Neurotransmitter Imbalance: The Root Cause of Tight Muscles?
You may want to see also
Explore related products





![]()
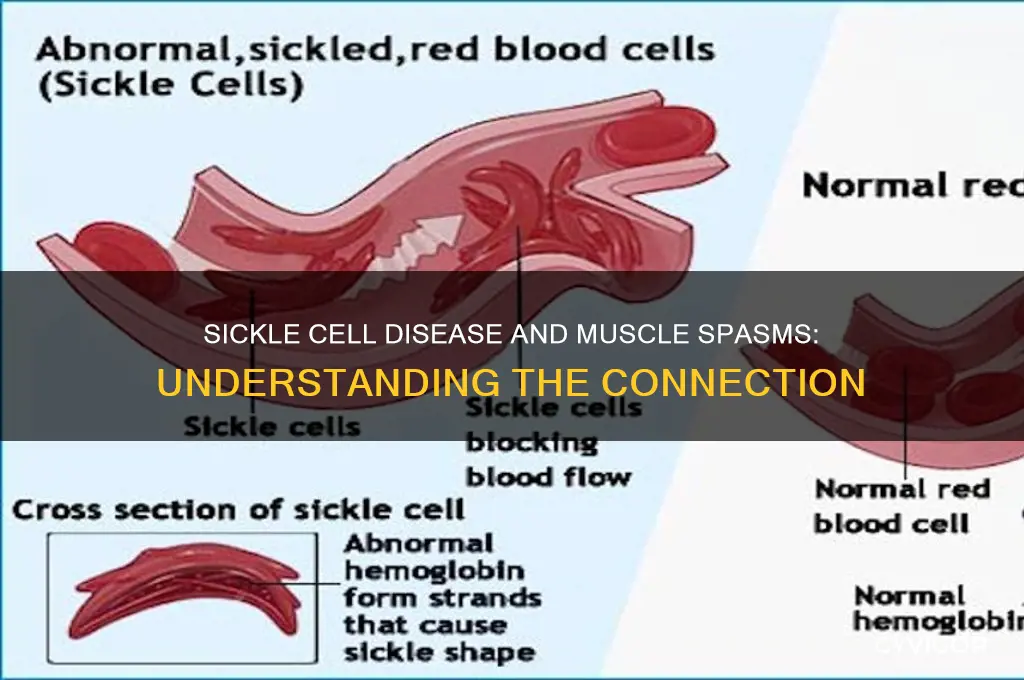
Vasculopathy and Pain: Reduced blood flow from sickle cells may trigger muscle cramps and spasms
Sickle cell disease (SCD) is a genetic disorder characterized by the production of abnormal hemoglobin, leading to the deformation of red blood cells into a sickle shape. These misshapen cells are less flexible and can obstruct blood flow, particularly in smaller vessels. This obstruction, known as vasculopathy, is a hallmark of SCD and plays a significant role in the development of various symptoms, including pain. Vasculopathy in SCD occurs when the sickle cells adhere to the walls of blood vessels, causing inflammation and further narrowing the vascular lumen. This reduced blood flow can have profound effects on tissues and organs, leading to ischemia (inadequate blood supply) and subsequent pain.
One of the direct consequences of vasculopathy in SCD is the triggering of muscle cramps and spasms. When blood flow to muscles is compromised, the tissues receive less oxygen and nutrients, leading to metabolic stress. This ischemic state can irritate muscle fibers and nerve endings, causing them to contract involuntarily. Muscle cramps, characterized by sudden, painful contractions, and spasms, which are prolonged and often more intense, are common manifestations of this process. The legs, arms, and back are frequently affected areas, as the muscles in these regions are more susceptible to ischemia due to their higher demand for oxygen during physical activity or even at rest.
The relationship between reduced blood flow and muscle cramps or spasms is further exacerbated by the release of inflammatory mediators and vasoactive substances during sickle cell crises. When sickle cells block blood vessels, they trigger an inflammatory response, leading to the release of cytokines and other chemicals that can sensitize pain receptors. This heightened sensitivity, combined with the ischemic environment, lowers the threshold for muscle contractions, making cramps and spasms more likely to occur. Additionally, the chronic nature of SCD means that repeated episodes of vasculopathy can lead to cumulative damage to muscles and nerves, further predisposing individuals to these painful symptoms.
Managing vasculopathy-induced muscle cramps and spasms in SCD requires a multifaceted approach. Hydration is critical, as adequate fluid intake helps maintain blood volume and reduces the viscosity of blood, thereby improving flow. Pain management strategies, including the use of nonsteroidal anti-inflammatory drugs (NSAIDs) or opioids in severe cases, can provide symptomatic relief. Physical therapy and gentle stretching exercises may also help alleviate muscle tension and improve circulation. In some cases, medications that modify sickle cell pathology, such as hydroxyurea or endothelin receptor antagonists, can be prescribed to reduce the frequency and severity of vaso-occlusive episodes, indirectly minimizing muscle cramps and spasms.
In conclusion, vasculopathy in sickle cell disease is a key mechanism linking reduced blood flow to muscle cramps and spasms. The ischemic conditions created by sickle cell-induced vascular obstruction, coupled with inflammation and nerve sensitization, contribute to the involuntary and painful muscle contractions experienced by patients. Understanding this relationship is essential for developing effective management strategies that address both the underlying vasculopathy and its symptomatic manifestations. By targeting blood flow improvement and pain relief, healthcare providers can significantly enhance the quality of life for individuals living with SCD.
Parkinson's Disease and Muscle Stiffness: Understanding the Connection
You may want to see also
Explore related products






![]()
Electrolyte Imbalance: Dehydration and anemia in sickle cell patients can disrupt electrolyte levels, causing spasms
Sickle cell disease (SCD) is a complex genetic disorder that affects the red blood cells, leading to a cascade of complications, including muscle spasms. One significant factor contributing to these spasms is electrolyte imbalance, which is often exacerbated by dehydration and anemia—common issues in SCD patients. Electrolytes such as sodium, potassium, calcium, and magnesium are crucial for proper muscle function and nerve signaling. When these levels are disrupted, it can result in involuntary muscle contractions or spasms. Understanding this relationship is essential for managing symptoms and improving the quality of life for individuals with SCD.
Dehydration is a frequent concern in sickle cell patients due to increased fluid loss, particularly during vaso-occlusive crises or episodes of pain. When the body is dehydrated, the concentration of electrolytes in the blood rises, disrupting the delicate balance required for optimal muscle and nerve function. For instance, low levels of potassium or magnesium can lead to hyperexcitability of muscles, causing spasms or cramps. Patients with SCD must prioritize hydration to maintain electrolyte equilibrium and reduce the risk of muscle-related complications. Simple measures like drinking adequate water, especially during crises, can help mitigate this issue.
Anemia, another hallmark of sickle cell disease, further complicates electrolyte balance. Hemoglobin, the protein in red blood cells responsible for oxygen transport, also plays a role in maintaining electrolyte stability. In SCD, the abnormal sickle-shaped cells break down prematurely, leading to chronic anemia. This reduces the body’s ability to deliver oxygen and nutrients efficiently, including those necessary for electrolyte regulation. Additionally, anemia can cause fatigue and reduced kidney function, which may impair the body’s ability to excrete excess electrolytes or retain essential ones, leading to imbalances that trigger muscle spasms.
The interplay between dehydration, anemia, and electrolyte imbalance in SCD patients highlights the need for a comprehensive approach to symptom management. Monitoring electrolyte levels through regular blood tests can help identify imbalances early. Treatment may involve oral or intravenous electrolyte supplements, depending on the severity of the imbalance. Dietary adjustments, such as consuming foods rich in potassium (e.g., bananas, oranges) and magnesium (e.g., leafy greens, nuts), can also support electrolyte stability. Addressing the root causes of dehydration and anemia, such as managing pain crises and ensuring adequate fluid intake, is equally critical.
In conclusion, electrolyte imbalance is a significant yet often overlooked contributor to muscle spasms in sickle cell disease patients. Dehydration and anemia, both common in SCD, disrupt the body’s electrolyte levels, leading to involuntary muscle contractions. By focusing on hydration, anemia management, and electrolyte monitoring, healthcare providers and patients can work together to alleviate this distressing symptom. Proactive measures, including dietary modifications and regular medical check-ups, are key to maintaining electrolyte balance and improving overall well-being in individuals with sickle cell disease.
Pulled Muscle and Diffuse Pain: What's the Link?
You may want to see also
Explore related products





![]()
Musculoskeletal Stress: Chronic pain and reduced mobility in sickle cell disease may contribute to muscle spasms
Sickle cell disease (SCD) is a genetic disorder characterized by abnormal hemoglobin in red blood cells, leading to their rigid, sickle-like shape. This deformation causes these cells to become stuck in small blood vessels, resulting in reduced blood flow and oxygen delivery to tissues. One of the most debilitating symptoms of SCD is chronic pain, often described as acute or chronic vaso-occlusive crises. These episodes occur when sickled cells block blood vessels, leading to ischemia (lack of blood supply) and subsequent tissue damage. Chronic pain in SCD is not only a direct result of these crises but also contributes to musculoskeletal stress, which can exacerbate muscle spasms.
The relationship between chronic pain and muscle spasms in SCD is multifaceted. Prolonged pain causes patients to adopt protective postures or limit movement to avoid discomfort. Over time, this reduced mobility leads to muscle stiffness, weakness, and imbalances. Muscles that are not regularly engaged or stretched become more susceptible to spasms, which are involuntary contractions that can be painful and further restrict movement. Additionally, chronic pain triggers a heightened state of muscle tension as the body’s natural response to protect the affected area, increasing the likelihood of spasms.
Reduced mobility in SCD patients also contributes to musculoskeletal stress through disuse atrophy and deconditioning. When muscles are underused due to pain or fear of triggering a crisis, they lose mass and strength. This atrophy weakens the muscles, making them less resilient to stress and more prone to spasms. Deconditioning, or the loss of physical fitness, further compounds the issue by reducing overall muscle endurance and flexibility. As a result, even minor movements or activities can strain the muscles, leading to spasms.
Another factor linking SCD to muscle spasms is the inflammatory response associated with the disease. Sickle cell crises trigger inflammation, which can affect muscles and surrounding tissues. Inflammation irritates muscle fibers and nerves, making them more excitable and likely to spasm. Moreover, chronic inflammation contributes to muscle fatigue and reduced threshold for contraction, exacerbating the risk of spasms. This inflammatory process, combined with the mechanical stress of reduced mobility, creates a cycle of musculoskeletal dysfunction in SCD patients.
Managing musculoskeletal stress in SCD requires a comprehensive approach to address both chronic pain and reduced mobility. Physical therapy plays a crucial role in maintaining muscle strength, flexibility, and range of motion. Gentle exercises, stretching, and low-impact activities can help prevent muscle atrophy and reduce the frequency of spasms. Pain management strategies, including medications, hydrotherapy, and heat or cold therapy, are essential to alleviate discomfort and encourage movement. Additionally, patient education on proper body mechanics and pacing activities can minimize muscle strain and prevent spasms. By targeting the root causes of musculoskeletal stress, individuals with SCD can improve their quality of life and reduce the burden of muscle spasms.
Muscle Fatigue: The Mystery of Lactate Buildup
You may want to see also
Explore related products






![]()
Medication Side Effects: Drugs used to manage sickle cell symptoms can sometimes induce muscle spasms as a side effect
Sickle cell disease (SCD) is a genetic disorder characterized by abnormally shaped red blood cells, leading to various complications such as pain crises, organ damage, and infections. To manage these symptoms, patients often rely on medications that, while beneficial, can introduce their own set of challenges. One such challenge is the potential for muscle spasms as a side effect of these medications. Muscle spasms, or involuntary contractions of muscles, can be distressing and impact a patient’s quality of life. Understanding the connection between SCD medications and muscle spasms is crucial for both patients and healthcare providers to manage symptoms effectively.
Several drugs commonly prescribed for SCD patients have been associated with muscle spasms. For instance, opioids, frequently used to manage acute pain during vaso-occlusive crises, can cause muscle rigidity and spasms as a side effect. This occurs due to opioids’ impact on the central nervous system, which can alter muscle tone and lead to involuntary contractions. Patients on long-term opioid therapy may be particularly susceptible to this side effect, requiring careful monitoring and dosage adjustments to minimize discomfort.
Another class of medications linked to muscle spasms is antidepressants, specifically those used to manage chronic pain in SCD patients. Tricyclic antidepressants (TCAs) and selective serotonin reuptake inhibitors (SSRIs) can affect neurotransmitter levels, potentially leading to muscle spasms or twitching. While these medications are effective in reducing neuropathic pain, their side effects must be weighed against their benefits, especially in patients already experiencing muscle-related symptoms.
Hydroxyurea, a disease-modifying medication for SCD, is generally well-tolerated but has been reported to cause muscle spasms in some patients. Although rare, this side effect may be related to the drug’s impact on red blood cell production and overall metabolic changes. Patients experiencing muscle spasms while on hydroxyurea should consult their healthcare provider to explore alternative treatments or adjunct therapies to alleviate this issue.
Finally, nonsteroidal anti-inflammatory drugs (NSAIDs), often used for mild to moderate pain in SCD, can contribute to muscle spasms, particularly when used in high doses or over extended periods. NSAIDs can cause electrolyte imbalances, such as low potassium levels, which are known to trigger muscle cramps and spasms. Patients using NSAIDs should maintain proper hydration and monitor their electrolyte levels to reduce the risk of this side effect.
In conclusion, while medications play a vital role in managing sickle cell disease symptoms, their potential to induce muscle spasms cannot be overlooked. Patients and healthcare providers must work collaboratively to identify and address these side effects, ensuring a balanced approach to treatment. Regular follow-ups, medication reviews, and lifestyle modifications, such as hydration and stretching exercises, can help mitigate muscle spasms and improve overall well-being in SCD patients.
Muscle Knots: A Surprising Cause of Headaches?
You may want to see also
Frequently asked questions
Yes, sickle cell disease can lead to muscle spasms due to reduced blood flow and oxygen delivery to muscles, causing pain and involuntary contractions.
Muscle spasms in sickle cell disease are often caused by vaso-occlusive crises, where sickle cells block blood vessels, reducing oxygen supply to muscles and triggering spasms.
While not the most common symptom, muscle spasms can occur during sickle cell crises, especially in areas with reduced blood flow, such as the legs and back.
Management includes pain relief medications, hydration, heat therapy, and muscle relaxants, as well as addressing the underlying sickle cell crisis with proper medical care.
Chronic muscle issues, including spasms, can develop in sickle cell patients due to repeated vaso-occlusive episodes and muscle damage over time. Early intervention is key to minimizing long-term effects.