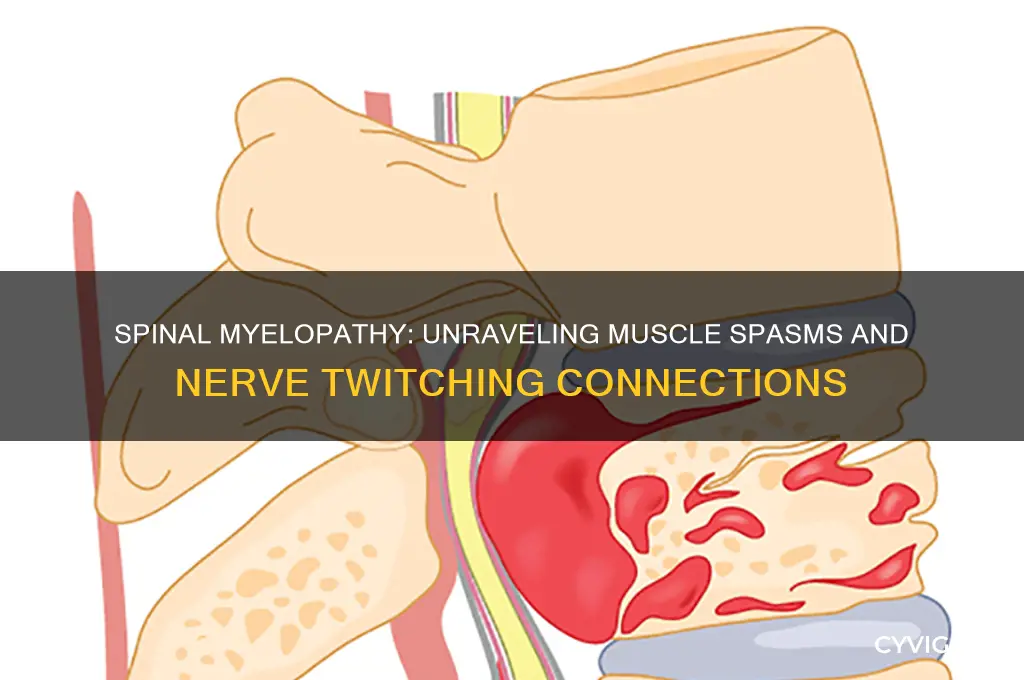
Spinal myelopathy, a condition characterized by the compression or damage to the spinal cord, can indeed lead to a range of neurological symptoms, including muscle spasms and nerve twitching. This occurs because the spinal cord plays a crucial role in transmitting signals between the brain and the rest of the body, and any disruption can result in abnormal nerve activity. Muscle spasms, or involuntary contractions, may arise due to the misfiring of motor neurons, while nerve twitching, known as fasciculations, can be a sign of lower motor neuron involvement. These symptoms often reflect the underlying irritation or dysfunction within the spinal cord, highlighting the importance of early diagnosis and treatment to prevent further neurological deterioration.
| Characteristics | Values |
|---|---|
| Definition | Spinal myelopathy refers to dysfunction of the spinal cord due to compression, injury, or disease, often caused by conditions like cervical spondylosis, tumors, or trauma. |
| Muscle Spasms | Yes, spinal myelopathy can cause muscle spasms due to irritation or compression of the spinal cord, leading to abnormal nerve signaling and involuntary muscle contractions. |
| Nerve Twitching | Yes, nerve twitching (fasciculations) can occur as a result of disrupted nerve signals from the spinal cord to muscles, often due to upper motor neuron involvement. |
| Underlying Mechanisms | - Compression of the spinal cord disrupts normal nerve transmission. - Upper motor neuron lesions lead to hyperreflexia and spasticity. - Lower motor neuron involvement causes fasciculations. |
| Associated Symptoms | Pain, weakness, numbness, tingling, difficulty walking, bowel/bladder dysfunction, and balance issues. |
| Common Causes | Cervical spondylosis, herniated discs, spinal stenosis, tumors, infections, or traumatic injuries. |
| Diagnosis | MRI, CT scan, electromyography (EMG), and neurological exams to assess spinal cord function and identify compression. |
| Treatment Options | Decompression surgery, physical therapy, medications (e.g., muscle relaxants, anti-inflammatory drugs), and management of underlying conditions. |
| Prognosis | Varies based on cause, severity, and timing of treatment. Early intervention improves outcomes; delayed treatment may lead to permanent neurological deficits. |
| Prevention | Maintaining spinal health through proper posture, regular exercise, and avoiding repetitive strain or injury. |
Explore related products






What You'll Learn
![]()
Myelopathy-induced muscle spasticity mechanisms
Spinal myelopathy, a condition characterized by the impairment of the spinal cord, can indeed lead to muscle spasms and nerve twitching, primarily through the development of muscle spasticity. This phenomenon is rooted in the disruption of normal neural signaling pathways due to spinal cord damage. In a healthy nervous system, the spinal cord acts as a critical relay center for motor commands from the brain to the muscles and sensory feedback from the body to the brain. When myelopathy occurs, this communication is compromised, often resulting in hyperexcitability of the motor neurons. This hyperexcitability arises because the inhibitory signals from the brain, which normally modulate muscle tone, are diminished or lost, leading to uncontrolled muscle contractions.
One of the key mechanisms underlying myelopathy-induced muscle spasticity is the loss of descending inhibitory pathways, particularly those involving the corticospinal and reticulospinal tracts. These pathways play a crucial role in regulating muscle tone and preventing excessive muscle activity. When the spinal cord is damaged, these inhibitory signals are reduced, allowing the excitatory pathways to dominate. This imbalance leads to increased muscle stiffness, spasms, and involuntary twitching. Additionally, the damage to the spinal cord can cause demyelination and gliosis, further disrupting the normal conduction of nerve impulses and exacerbating spasticity.
Another contributing factor is the alteration of spinal cord circuitry at the segmental level. The spinal cord contains interneurons that modulate motor neuron activity, ensuring smooth and coordinated muscle movements. In myelopathy, these interneurons may become dysfunctional or die, leading to a loss of local inhibitory control. This dysfunction results in heightened motor neuron activity, manifesting as muscle spasms and twitching. Furthermore, the accumulation of neurotransmitters like glutamate, which is excitatory, can occur due to impaired reuptake mechanisms, further amplifying the hyperexcitability of motor neurons.
Peripheral nerve involvement also plays a role in myelopathy-induced spasticity. As the spinal cord damage progresses, the peripheral nerves that innervate muscles may become sensitized or damaged, contributing to abnormal muscle activity. This peripheral sensitization can lead to increased reflex responses, such as clonus (rapid, alternating muscle contractions and relaxations), which are commonly observed in individuals with spasticity. The combination of central and peripheral mechanisms creates a complex interplay that sustains and worsens muscle spasms and nerve twitching.
Finally, neuroplastic changes in the spinal cord and brain contribute to the chronicity of spasticity in myelopathy. Over time, the nervous system attempts to compensate for the damage by reorganizing its circuitry, but these adaptations often lead to maladaptive changes. For example, the sprouting of new nerve fibers or the upregulation of excitatory receptors can further enhance motor neuron activity, perpetuating spasticity. Understanding these mechanisms is crucial for developing targeted therapies, such as antispasticity medications, physical therapy, or surgical interventions, to manage the symptoms and improve the quality of life for individuals with myelopathy-induced muscle spasticity.
Essential Tremor: Understanding Muscle Spasms
You may want to see also
Explore related products






![]()
Nerve twitching linked to spinal cord compression
Spinal myelopathy, a condition resulting from spinal cord compression, is often associated with a range of neurological symptoms, including muscle spasms and nerve twitching. Nerve twitching, also known as fasciculations, occurs when muscle fibers contract involuntarily due to abnormal nerve signaling. When the spinal cord is compressed, whether from conditions like herniated discs, spinal stenosis, or degenerative diseases, the normal transmission of nerve impulses is disrupted. This disruption can lead to overactivity in the motor neurons, causing muscles to twitch uncontrollably. Understanding this link is crucial for identifying the underlying cause of such symptoms and pursuing appropriate treatment.
The mechanism behind nerve twitching in spinal cord compression involves the irritation or damage to nerve roots and pathways within the spinal cord. As the spinal cord becomes compressed, the affected nerves may send erratic signals to muscles, resulting in twitching. This is particularly common in areas innervated by the compressed spinal segments. For instance, cervical spinal myelopathy might cause twitching in the arms or hands, while lumbar compression could lead to twitching in the legs. Recognizing the anatomical correlation between the site of compression and the location of twitching can aid in diagnosing the specific level of spinal involvement.
Muscle spasms often accompany nerve twitching in cases of spinal myelopathy, further complicating the patient’s condition. Spasms occur when muscles contract forcefully and involuntarily, sometimes causing pain or stiffness. The combination of spasms and twitching can significantly impair mobility and quality of life. These symptoms arise because the compressed spinal cord affects both the sensory and motor pathways, leading to heightened muscle activity and abnormal reflexes. Early intervention, such as physical therapy, medications, or surgical decompression, is essential to prevent long-term nerve damage and alleviate these distressing symptoms.
Diagnosing nerve twitching linked to spinal cord compression requires a thorough evaluation, including a detailed medical history, neurological examination, and imaging studies like MRI or CT scans. These tools help identify the source and extent of spinal compression. Once diagnosed, treatment focuses on relieving pressure on the spinal cord and managing symptoms. Non-surgical options may include anti-inflammatory medications, muscle relaxants, or epidural steroid injections to reduce inflammation and pain. In severe cases, surgical decompression may be necessary to create more space for the spinal cord and prevent further nerve damage.
Patients experiencing nerve twitching and muscle spasms should not ignore these symptoms, as they may indicate progressive spinal myelopathy. Early detection and treatment can prevent irreversible neurological deficits and improve outcomes. Lifestyle modifications, such as maintaining a healthy weight, practicing good posture, and avoiding activities that strain the spine, can also help manage symptoms. By addressing spinal cord compression promptly, individuals can reduce the frequency and severity of nerve twitching and related complications, ultimately enhancing their overall well-being.
Cholesterol and Muscle Pain: Is There a Link?
You may want to see also
Explore related products




![]()
Cervical myelopathy and lower limb spasms
Cervical myelopathy, a condition resulting from spinal cord compression in the neck region, can indeed lead to a variety of symptoms, including lower limb spasms. This occurs due to the disruption of neural signals between the brain and the spinal cord, affecting the motor pathways that control muscle movements. When the cervical spine is compromised, often by conditions like degenerative disc disease, herniated discs, or spinal stenosis, it can exert pressure on the spinal cord, leading to myelopathy. This compression interferes with the normal transmission of nerve impulses, causing muscles in the lower limbs to contract involuntarily, resulting in spasms.
Lower limb spasms in cervical myelopathy are characterized by sudden, uncontrollable muscle contractions that can range from mild twitches to severe, painful spasms. These spasms often occur in the legs, calves, or feet and may be triggered by movement, changes in position, or even at rest. The spasms can significantly impact mobility and quality of life, making walking or standing for extended periods challenging. Additionally, nerve twitching, or fasciculations, may accompany these spasms, further indicating the involvement of the nervous system. These symptoms arise because the damaged spinal cord fails to properly regulate muscle activity, leading to hyperactive reflexes and abnormal muscle responses.
The relationship between cervical myelopathy and lower limb spasms highlights the importance of early diagnosis and intervention. Persistent or worsening spasms should prompt a thorough neurological evaluation, including imaging studies like MRI to assess the cervical spine. Treatment options vary depending on the severity of the condition but often include physical therapy, medications to manage spasticity, and, in some cases, surgical decompression to relieve spinal cord pressure. Early management can help prevent further neurological deterioration and improve symptoms, including reducing the frequency and intensity of lower limb spasms.
Patients with cervical myelopathy experiencing lower limb spasms may also benefit from multidisciplinary care. Neurologists, physiatrists, and physical therapists can collaborate to develop a tailored treatment plan. Techniques such as stretching exercises, bracing, and the use of antispasticity medications like baclofen or tizanidine can provide symptomatic relief. For those with progressive myelopathy, surgical options like anterior cervical discectomy and fusion (ACDF) or laminoplasty may be necessary to decompress the spinal cord and halt disease progression, thereby addressing the root cause of the spasms.
In summary, cervical myelopathy can directly cause lower limb spasms and nerve twitching due to spinal cord compression and subsequent disruption of motor pathways. Recognizing these symptoms as potential indicators of myelopathy is crucial for timely intervention. Effective management requires a combination of medical, therapeutic, and, if necessary, surgical approaches to alleviate spasms and improve overall function. Patients experiencing these symptoms should seek prompt medical attention to prevent long-term complications and enhance their quality of life.
Statins and Muscle Atrophy: What's the Link?
You may want to see also
Explore related products






![]()
Thoracic myelopathy effects on muscle control
Thoracic myelopathy, a condition resulting from spinal cord compression or injury in the thoracic region, significantly impacts muscle control due to disruption of neural pathways. The thoracic spine (T1-T12) houses critical nerve fibers that transmit signals between the brain and the body, governing movement, sensation, and reflexes. When myelopathy occurs in this region, it can lead to impaired communication between the central nervous system and peripheral muscles. This disruption often manifests as muscle spasms, characterized by involuntary contractions of one or more muscle groups. These spasms arise because damaged nerve pathways may send erratic signals, causing muscles to activate unpredictably.
Nerve twitching, or fasciculations, is another common symptom of thoracic myelopathy. Fasciculations occur when individual muscle fibers or groups of fibers contract spontaneously due to abnormal nerve firing. This twitching is typically visible or palpable under the skin and can be a direct result of nerve irritation or degeneration caused by spinal cord compression. The thoracic region's involvement means that muscles in the chest, abdomen, and upper back are particularly susceptible to these involuntary movements. Over time, persistent nerve twitching can contribute to muscle fatigue and weakness, further compromising motor function.
The effects of thoracic myelopathy on muscle control extend beyond spasms and twitching to include generalized weakness and coordination difficulties. As the condition progresses, patients may experience reduced muscle strength in the lower and upper extremities, depending on the specific level and severity of spinal cord involvement. This weakness often leads to difficulties with fine motor tasks, balance, and gait. For instance, patients may struggle with activities like buttoning shirts or maintaining stability while walking. The loss of precise muscle control is a direct consequence of impaired nerve signal transmission through the damaged thoracic spinal cord.
Sensory disturbances associated with thoracic myelopathy can also indirectly affect muscle control. Altered sensation in the limbs, such as numbness or tingling, can disrupt proprioception—the body's ability to sense its position in space. Without accurate sensory feedback, muscles may not respond appropriately to movements, leading to clumsiness or uncoordinated actions. Additionally, pain resulting from nerve compression can cause protective muscle guarding, where muscles tense up to avoid further discomfort, exacerbating spasms and stiffness.
Management of thoracic myelopathy-induced muscle control issues often involves a multidisciplinary approach. Physical therapy plays a crucial role in strengthening muscles, improving flexibility, and enhancing coordination. Medications, such as muscle relaxants or antispasmodics, may be prescribed to alleviate spasms and twitching. In severe cases, surgical intervention to decompress the spinal cord can help restore neural function and improve muscle control. Early diagnosis and treatment are essential to prevent irreversible damage and optimize outcomes for individuals with thoracic myelopathy.
Sore Muscles and Fever: Understanding the Connection and Symptoms
You may want to see also
Explore related products





![]()
Lumbar myelopathy and upper extremity twitching
Lumbar myelopathy, a condition affecting the spinal cord in the lower back region, is often associated with a range of neurological symptoms. While it primarily impacts the lower extremities, its effects can extend beyond, leading to questions about its relationship with upper extremity twitching. The spinal cord's role in transmitting signals between the brain and the rest of the body means that any compression or damage in the lumbar region can potentially disrupt nerve function, causing muscle spasms and nerve twitching in various parts of the body, including the arms.
The connection between lumbar myelopathy and upper extremity twitching lies in the complex network of nerve fibers within the spinal cord. Myelopathy can result from conditions such as spinal stenosis, herniated discs, or degenerative diseases, which compress or irritate the spinal cord. This compression may lead to abnormal nerve signaling, manifesting as involuntary muscle contractions or twitching. Although the lumbar region is distant from the upper extremities, the spinal cord's intricate circuitry allows for referred symptoms, where issues in one area can affect seemingly unrelated body parts.
Upper extremity twitching in the context of lumbar myelopathy can be understood through the concept of radiculopathy and central nervous system involvement. When the spinal cord is compromised, nerve roots extending from it can become irritated or damaged. These nerve roots form part of the brachial plexus, which supplies the arms. As a result, individuals with lumbar myelopathy might experience not only leg-related symptoms but also arm twitching, tingling, or weakness. This phenomenon highlights the interconnectedness of the spinal cord and the potential for widespread neurological manifestations.
It is essential to differentiate between muscle spasms and nerve twitching, as they may have distinct implications in lumbar myelopathy. Muscle spasms are typically more sustained, painful contractions, often related to muscle strain or spinal instability. In contrast, nerve twitching, or fasciculations, are brief, involuntary muscle fiber movements caused by spontaneous nerve discharges. In the case of upper extremity twitching, fasciculations may be more indicative of nerve irritation or damage originating from the lumbar spine, especially when accompanied by other myelopathic signs such as gait changes or bowel/bladder dysfunction.
Diagnosing and managing lumbar myelopathy-related upper extremity twitching requires a comprehensive approach. Imaging studies like MRI can identify spinal cord compression or abnormalities, while electromyography (EMG) and nerve conduction studies can assess nerve function and localization. Treatment strategies may include conservative measures such as physical therapy, bracing, or medications to manage pain and inflammation. In severe cases, surgical intervention might be necessary to decompress the spinal cord and prevent further neurological deterioration. Early recognition of these symptoms is crucial, as timely intervention can significantly impact the prognosis and quality of life for individuals with lumbar myelopathy.
Ezetimibe Side Effects: Muscle and Joint Pain Explained
You may want to see also
Frequently asked questions
Yes, spinal myelopathy can cause muscle spasms due to compression or damage to the spinal cord, which disrupts nerve signals and leads to involuntary muscle contractions.
Yes, spinal myelopathy can cause nerve twitching (fasciculations) as a result of irritated or damaged nerve fibers in the spinal cord sending abnormal signals to muscles.
Muscle spasms and nerve twitching can be early signs of spinal myelopathy, but they often appear alongside other symptoms like weakness, numbness, or coordination issues. Early diagnosis is crucial for effective management.