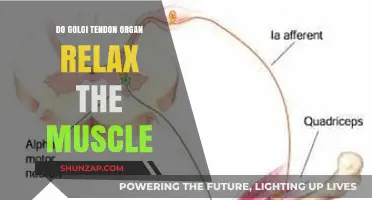
Muscle relaxants are commonly prescribed to alleviate muscle spasms, pain, and stiffness, but their potential side effects have raised questions about their impact on sleep behaviors. One intriguing concern is whether these medications can cause individuals to talk in their sleep, a phenomenon known as somniloquy. While muscle relaxants primarily target skeletal muscles, their influence on the central nervous system may inadvertently affect sleep stages and disrupt normal sleep patterns. This has led to anecdotal reports and curiosity about whether these drugs might induce sleep talking, prompting further investigation into the relationship between muscle relaxants and altered sleep behaviors.
| Characteristics | Values |
|---|---|
| Effect on Sleep Talking | Muscle relaxants may indirectly contribute to sleep talking due to their impact on sleep stages, particularly REM sleep. However, there is no direct evidence that muscle relaxants specifically cause sleep talking. |
| Mechanism of Action | Muscle relaxants work by reducing muscle tension and spasms, which can affect overall relaxation but do not target speech mechanisms directly. |
| Common Muscle Relaxants | Cyclobenzaprine, Tizanidine, Baclofen, and others. |
| Side Effects Related to Sleep | May cause drowsiness, dizziness, or altered sleep patterns, which could indirectly influence sleep behaviors like talking. |
| Scientific Studies | Limited research specifically links muscle relaxants to sleep talking. Most studies focus on their effects on sleep quality and muscle relaxation. |
| Individual Variability | Effects on sleep talking may vary based on the individual, dosage, and specific medication used. |
| Conclusion | While muscle relaxants can alter sleep patterns, there is no conclusive evidence that they directly cause sleep talking. |
Explore related products






What You'll Learn
![]()
Types of Muscle Relaxants and Sleep Talking
Muscle relaxants, broadly categorized into antispasmodics and antispastics, target different physiological mechanisms to alleviate muscle tension. Antispasmodics, such as cyclobenzaprine (Flexeril) and tizanidine (Zanaflex), act on the central nervous system to reduce muscle spasms. Antispastics, like baclofen, modulate spinal reflexes to decrease muscle stiffness. While these medications are primarily prescribed for conditions like back pain or multiple sclerosis, their impact on sleep behaviors, including sleep talking, varies based on their pharmacological profile. For instance, cyclobenzaprine’s sedative effects may alter sleep stages, potentially increasing the likelihood of parasomnia, whereas tizanidine’s shorter duration of action might minimize such disruptions.
The relationship between muscle relaxants and sleep talking hinges on how these drugs influence sleep architecture. Sleep talking, or somniloquy, often occurs during non-rapid eye movement (NREM) sleep, particularly in lighter stages. Muscle relaxants that prolong NREM sleep or disrupt the transition to deeper stages could theoretically increase sleep talking episodes. For example, a 10 mg dose of cyclobenzaprine before bedtime may induce drowsiness but also fragment sleep, creating conditions conducive to parasomnias. Patients should monitor their sleep patterns after initiating such medications, especially if they share a bed or room, as sleep talking can be disruptive to others.
Not all muscle relaxants carry the same risk for sleep talking. Direct-acting agents like dantrolene, which works on muscle fibers rather than the nervous system, are less likely to interfere with sleep stages. Conversely, medications with a strong sedative component, such as methocarbamol (Robaxin), may increase the risk by altering sleep depth and stability. Dosage plays a critical role here—a 500 mg dose of methocarbamol might be more likely to induce sleep disturbances than a 250 mg dose. Patients should discuss the lowest effective dose with their healthcare provider to minimize side effects.
Practical strategies can mitigate the risk of sleep talking while using muscle relaxants. Avoiding evening doses, especially for medications with long half-lives like baclofen, can reduce nighttime disruptions. Combining muscle relaxants with sleep hygiene practices, such as maintaining a consistent sleep schedule and creating a quiet sleep environment, may also help. For older adults, who are more susceptible to both parasomnias and medication side effects, starting with the lowest possible dose and gradually titrating upward is advisable. If sleep talking persists or worsens, consulting a sleep specialist to explore underlying sleep disorders or alternative treatments is recommended.
In conclusion, while muscle relaxants do not universally cause sleep talking, certain types and dosages may increase the risk by altering sleep architecture. Patients and clinicians should weigh the benefits of muscle relaxation against potential sleep disturbances, tailoring treatment plans to individual needs. Awareness of these dynamics empowers users to manage their symptoms effectively while minimizing unwanted side effects.
Does Anesthesia Relax Muscles? Exploring Its Effects on Muscle Tension
You may want to see also
Explore related products






![]()
Mechanism: How Relaxants Affect Sleep Stages
Muscle relaxants, often prescribed for conditions like muscle spasms or chronic pain, can significantly alter sleep architecture by disrupting the delicate balance of sleep stages. These medications primarily target the central nervous system or act peripherally on muscle fibers, but their systemic effects can inadvertently influence sleep-wake cycles. For instance, cyclobenzaprine, a commonly prescribed muscle relaxant, has been shown to reduce rapid eye movement (REM) sleep, the stage associated with vivid dreaming and muscle atonia. This reduction in REM sleep may paradoxically increase sleep talking, as the brain’s inhibitory mechanisms on motor activity during dreaming are less effective.
To understand this mechanism, consider the role of gamma-aminobutyric acid (GABA), a neurotransmitter that muscle relaxants often modulate. GABA inhibits neuronal activity, promoting relaxation and reducing muscle tension. However, excessive GABAergic activity can suppress REM sleep, leading to fragmented sleep patterns. For example, a study published in *Sleep Medicine Reviews* found that patients taking tizanidine, another muscle relaxant, experienced a 20% decrease in REM sleep duration compared to placebo. This disruption can cause individuals to transition abruptly between sleep stages, potentially triggering vocalizations during sleep as the brain struggles to maintain atonia.
Dosage plays a critical role in these effects. Lower doses of muscle relaxants (e.g., 5–10 mg of cyclobenzaprine) may have milder impacts on sleep architecture, while higher doses (15–30 mg) can exacerbate REM suppression. Age is another factor; older adults, who metabolize medications more slowly, are more susceptible to sleep disturbances from muscle relaxants. For instance, a 70-year-old taking 10 mg of cyclobenzaprine may experience more pronounced sleep talking than a 30-year-old on the same dose. To mitigate these effects, clinicians often recommend taking muscle relaxants earlier in the evening, allowing the medication to wear off by the time REM sleep predominates in the early morning hours.
Comparatively, muscle relaxants that act peripherally, such as dantrolene, have a lower likelihood of affecting sleep stages since they target muscle fibers directly rather than the central nervous system. However, even these medications can indirectly influence sleep by alleviating pain, which may improve sleep quality but does not address the potential for sleep talking. For patients concerned about sleep disturbances, combining muscle relaxants with sleep hygiene practices—such as maintaining a consistent sleep schedule and avoiding stimulants before bed—can help stabilize sleep architecture.
In conclusion, muscle relaxants can alter sleep stages by modulating neurotransmitter activity and reducing REM sleep, which may paradoxically increase sleep talking. Understanding the specific mechanisms and factors like dosage and age allows for more tailored treatment strategies. Patients and clinicians should weigh the benefits of muscle relaxation against potential sleep disruptions, exploring alternatives or adjunctive therapies when necessary. Practical steps, such as timing medication intake and improving sleep hygiene, can minimize unwanted effects and promote restorative sleep.
Botulism's Impact: Does It Cause Muscle Contraction or Relaxation?
You may want to see also
Explore related products





![]()
Common Side Effects Linked to Sleep Talking
Sleep talking, or somniloquy, is a phenomenon that can be influenced by various factors, including medication. Muscle relaxants, commonly prescribed for conditions like muscle spasms or chronic pain, have been anecdotally linked to sleep talking episodes. While not everyone experiences this side effect, understanding the potential connection is crucial for those taking these medications.
The Mechanism Behind the Chatter
Muscle relaxants work by depressing the central nervous system, leading to reduced muscle tension and pain relief. However, this depression can also impact the brain's regulation of sleep stages. During sleep, our bodies typically cycle through periods of REM (rapid eye movement) and non-REM sleep. Muscle relaxants may disrupt this cycle, causing more frequent awakenings or transitions between stages. It is during these transitions that sleep talking is most likely to occur. The brain's attempt to process information or respond to stimuli can result in verbalizations, often without the sleeper's awareness.
Unraveling the Evidence
Research specifically linking muscle relaxants to sleep talking is limited, but user reports and medical case studies provide valuable insights. For instance, a study on the effects of cyclobenzaprine, a commonly prescribed muscle relaxant, noted that 5% of participants experienced vivid dreams and sleep disturbances, which could potentially include sleep talking. Another study on tizanidine, another muscle relaxant, reported that 12% of patients experienced abnormal dreams, further suggesting a connection between these medications and altered sleep behaviors. These findings, though not conclusive, indicate a possible relationship between muscle relaxant use and sleep talking.
Practical Considerations and Management
If you suspect your muscle relaxant is causing sleep talking, consider the following steps:
- Dosage Review: Discuss with your healthcare provider if a lower dose might alleviate side effects while maintaining therapeutic benefits. For example, reducing a 10mg dose of cyclobenzaprine to 5mg before bedtime could minimize disruptions.
- Timing Adjustment: Taking the medication earlier in the evening might allow its peak effects to coincide with deeper sleep stages, potentially reducing sleep talking incidents.
- Alternative Therapies: Explore non-pharmacological options like physical therapy, acupuncture, or yoga to manage muscle pain, thereby reducing reliance on relaxants.
- Sleep Hygiene: Implement a consistent sleep routine, limit caffeine intake, and create a restful environment to improve overall sleep quality and minimize talking episodes.
A Balanced Perspective
While muscle relaxants may contribute to sleep talking, it's essential to weigh this against their therapeutic benefits. For many, these medications provide significant relief from pain and improved quality of life. Sleep talking, though potentially embarrassing or disruptive, is generally harmless. By understanding the connection and taking proactive measures, individuals can manage this side effect effectively, ensuring both physical comfort and restful sleep.
Optimal Muscle Relaxer Timing: How Many Hours Apart Should You Take Them?
You may want to see also
Explore related products




$21.95 $27.95


![]()
Individual Differences in Sleep Talking Reactions
Sleep talking, or somniloquy, is a phenomenon that varies widely among individuals, and the introduction of muscle relaxants into the equation adds another layer of complexity. While muscle relaxants are primarily prescribed to alleviate muscle spasms, pain, and stiffness, their impact on sleep talking is not uniform across users. Some individuals report an increase in sleep talking episodes, while others experience no change or even a reduction. This variability underscores the importance of understanding individual differences in reactions to these medications.
Consider the case of a 45-year-old woman prescribed cyclobenzaprine (10 mg daily) for chronic back pain. Within a week, her partner noticed a significant increase in her sleep talking, often accompanied by vivid, nonsensical narratives. In contrast, a 30-year-old man taking tizanidine (4 mg twice daily) for muscle spasms reported no change in his sleep behavior. These examples highlight how age, dosage, and individual physiology can influence the likelihood of sleep talking while on muscle relaxants. For instance, older adults may metabolize medications more slowly, potentially prolonging their effects and increasing the risk of side effects like sleep talking.
To minimize the risk of sleep talking while on muscle relaxants, patients should adhere to specific guidelines. First, start with the lowest effective dose, as higher doses (e.g., 20 mg of cyclobenzaprine) are more likely to disrupt sleep patterns. Second, take the medication earlier in the evening to allow its peak effects to subside before bedtime. For example, taking tizanidine 2–3 hours before sleep can reduce its impact on REM sleep, the stage most associated with sleep talking. Third, maintain a consistent sleep schedule to stabilize circadian rhythms, which can mitigate medication-induced disturbances.
Comparatively, benzodiazepines like diazepam, sometimes used as muscle relaxants, may have a more pronounced effect on sleep talking due to their sedative properties. A study found that 20% of patients on diazepam (5–10 mg daily) reported increased sleep talking, compared to 10% on non-benzodiazepine muscle relaxants. This suggests that the mechanism of action—benzodiazepines enhance GABA activity, potentially altering sleep architecture—plays a role in individual reactions. Patients concerned about sleep talking should discuss alternative medications with their healthcare provider, such as non-pharmacological options like physical therapy or over-the-counter pain relievers.
Finally, tracking sleep patterns can provide valuable insights into individual reactions. Keeping a sleep diary to record episodes of sleep talking, medication timing, and dosage can help identify correlations. For instance, a 50-year-old man noted that his sleep talking increased only when he took methocarbamol (750 mg) within an hour of bedtime. Adjusting his dosage timing reduced the frequency of these episodes. This proactive approach empowers individuals to manage their symptoms effectively, ensuring that muscle relaxants provide relief without disrupting their sleep or that of their bed partner.
Do Drug Panels Detect Muscle Relaxers? A Comprehensive Testing Guide
You may want to see also
Explore related products





![]()
Preventing Sleep Talking While on Relaxants
Muscle relaxants, while effective for alleviating pain and tension, can disrupt sleep patterns and trigger sleep talking in some individuals. This phenomenon often stems from the medication’s impact on the central nervous system, which can alter REM sleep and induce vocalizations. To mitigate this side effect, consider adjusting the timing of your dosage. Taking muscle relaxants earlier in the evening, at least 2–3 hours before bedtime, allows the sedative effects to peak during the initial sleep stages, reducing the likelihood of sleep talking during REM cycles. For example, if your medication is prescribed for nighttime use, consult your doctor about shifting the dose to early evening, ensuring it aligns with your sleep schedule without compromising its therapeutic benefits.
Another practical strategy involves creating a sleep environment that minimizes triggers for sleep talking. Keep the bedroom cool, dark, and quiet, as external disturbances can exacerbate vocalizations. Incorporate white noise or earplugs to mask sudden sounds that might prompt unconscious responses. Additionally, avoid consuming caffeine, alcohol, or heavy meals close to bedtime, as these can interfere with sleep quality and amplify the effects of muscle relaxants. For instance, limiting caffeine intake after 2 PM and avoiding alcohol within 3 hours of sleep can significantly reduce nocturnal disruptions, particularly in individuals aged 40–60 who are more susceptible to sleep disturbances.
If dosage adjustments and environmental changes prove insufficient, explore complementary therapies to stabilize sleep patterns. Cognitive-behavioral therapy for insomnia (CBT-I) has shown promise in reducing sleep talking by addressing underlying sleep hygiene issues. Techniques such as progressive muscle relaxation or guided meditation can also counteract the stimulating effects of muscle relaxants, promoting deeper, more restful sleep. For those on long-term relaxant regimens, combining medication with these therapies under professional guidance can yield better outcomes. A study published in *Sleep Medicine Reviews* highlights that patients who integrated CBT-I with their treatment plan experienced a 40% reduction in sleep talking episodes within 8 weeks.
Lastly, open communication with your healthcare provider is crucial. If sleep talking persists despite these measures, discuss alternative medications or dosage reductions. Some muscle relaxants, like cyclobenzaprine, are more likely to cause sleep disturbances than others, such as methocarbamol. Your doctor may recommend a trial of a different relaxant or adjunctive treatments like melatonin (1–3 mg) to regulate sleep cycles without exacerbating side effects. Always adhere to prescribed dosages and avoid self-adjusting medication, as abrupt changes can lead to withdrawal symptoms or reduced efficacy. By combining medical oversight with targeted lifestyle adjustments, you can effectively manage sleep talking while benefiting from muscle relaxants.
Can Muscle Relaxers Effectively Heal Chronic Back Pain?
You may want to see also
Frequently asked questions
Muscle relaxants can potentially increase the likelihood of sleep talking as they affect the central nervous system and may alter sleep patterns, leading to parasomnia behaviors like talking during sleep.
Muscle relaxants can disrupt normal sleep stages, particularly REM sleep, which is associated with dreaming and vocalizations. This disruption may trigger sleep talking in some individuals.
Sleep talking is not a widely reported side effect of muscle relaxants, but it can occur in individuals predisposed to parasomnias or those experiencing altered sleep patterns due to the medication.
Yes, muscle relaxants may exacerbate sleep talking in individuals who already experience it, as they can further disrupt sleep architecture and increase the likelihood of parasomnia episodes.
To minimize sleep talking, maintain a consistent sleep schedule, create a relaxing bedtime routine, and discuss alternative medications or dosages with your healthcare provider if sleep disturbances persist.