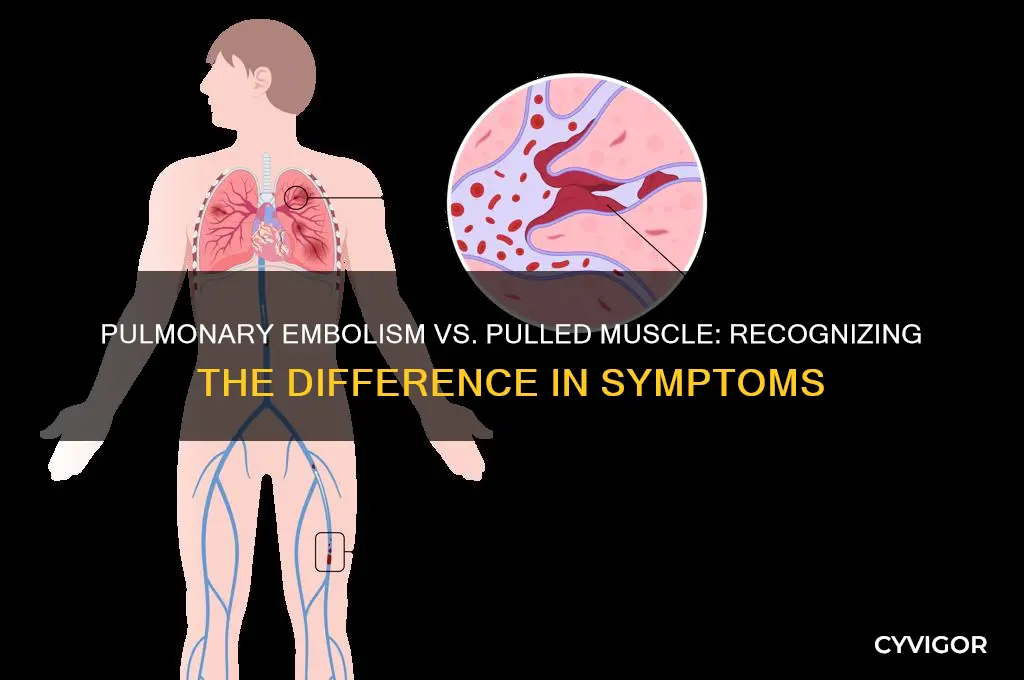
A pulmonary embolism (PE) is a serious and potentially life-threatening condition that occurs when a blood clot lodges in the pulmonary arteries, blocking blood flow to the lungs. While symptoms can vary widely, many people wonder if a pulmonary embolism might feel similar to a pulled muscle, particularly in the chest or back. This question arises because both conditions can cause discomfort or pain in the chest area, leading to confusion or delay in seeking medical attention. However, it’s crucial to understand that a pulmonary embolism typically presents with distinct symptoms, such as sudden shortness of breath, rapid heartbeat, coughing (sometimes with blood), and sharp, stabbing chest pain that worsens with deep breaths. In contrast, a pulled muscle usually causes localized, aching pain that improves with rest and worsens with movement. Recognizing these differences is essential, as prompt diagnosis and treatment of a pulmonary embolism are critical to prevent severe complications or fatality.
Explore related products






What You'll Learn
- Chest Pain Comparison: Sharp vs. dull pain, location, and intensity differences between PE and muscle strain
- Shortness of Breath: Sudden breathing difficulty in PE vs. gradual discomfort in muscle pulls
- Leg Swelling: Deep vein thrombosis (DVT) link to PE, absent in muscle injuries
- Onset Timing: Immediate PE symptoms vs. gradual muscle pain after activity
- Associated Symptoms: Fever, cough, or rapid heart rate in PE, not in muscle pulls
![]()
Chest Pain Comparison: Sharp vs. dull pain, location, and intensity differences between PE and muscle strain
Chest pain can be a symptom of both a pulmonary embolism (PE) and a muscle strain, but the characteristics of the pain differ significantly. Understanding these differences is crucial for timely and accurate diagnosis. Sharp pain is often associated with a pulmonary embolism, typically felt as a sudden, stabbing sensation in the chest. This pain may worsen with deep breaths or coughing, a hallmark of PE due to the blockage in the pulmonary artery. In contrast, a muscle strain usually presents as a dull, aching pain that intensifies with movement or palpation of the affected area. The sharpness of PE-related pain is a key differentiator, often described as acute and unrelenting, whereas muscle strain pain is more localized and improves with rest.
Location of the pain is another critical factor. Pulmonary embolism pain is generally centralized in the chest, often radiating to the shoulder, back, or neck. It is not confined to a specific muscle group but rather reflects the systemic impact of the embolism. Muscle strain, however, is typically localized to the area of injury, such as the intercostal muscles or chest wall. For instance, a strained pectoral muscle will cause pain in the front of the chest, while a strained back muscle will cause discomfort in the thoracic region. Recognizing the pain’s location can help distinguish between these conditions, though overlap can occur, especially if the strain involves muscles near the rib cage.
Intensity and duration of pain also vary. Pulmonary embolism pain is often severe and persistent, with patients frequently describing it as the worst pain they’ve ever experienced. It does not subside with over-the-counter pain relievers and may be accompanied by symptoms like shortness of breath, rapid heartbeat, and coughing up blood. Muscle strain pain, while potentially intense, is usually manageable with rest, ice, compression, and elevation (RICE) and may respond to nonsteroidal anti-inflammatory drugs (NSAIDs) like ibuprofen (200–400 mg every 4–6 hours, as needed). If chest pain is sudden, severe, and accompanied by systemic symptoms, seek emergency medical attention immediately, as it could indicate a life-threatening condition like PE.
Practical tips for differentiation include monitoring associated symptoms and assessing pain triggers. For example, if chest pain worsens with deep breathing or is accompanied by leg swelling or unexplained shortness of breath, a pulmonary embolism is more likely. Conversely, if pain is exacerbated by specific movements, such as lifting or twisting, and improves with rest, a muscle strain is more probable. Always err on the side of caution; chest pain should never be ignored, especially in individuals over 40, smokers, or those with a history of blood clots or recent surgery, as these are risk factors for PE. Early diagnosis and treatment can be life-saving.
Pulled Muscle Pain: Symptoms, Sensations, and What to Expect
You may want to see also
Explore related products






![]()
Shortness of Breath: Sudden breathing difficulty in PE vs. gradual discomfort in muscle pulls
Shortness of breath is a symptom that can arise from both a pulmonary embolism (PE) and a pulled muscle, but the onset and nature of this discomfort differ dramatically between the two conditions. In a PE, shortness of breath often manifests suddenly and intensely, as if someone has clamped down on your chest, restricting your ability to take a full breath. This occurs because a blood clot blocks blood flow to the lungs, impairing oxygen exchange. Patients frequently describe feeling like they’re drowning or suffocating, even at rest. In contrast, a pulled muscle typically causes a gradual, localized discomfort that worsens with movement or deep breaths. The shortness of breath here, if present, is mild and tied directly to the strained area, such as the intercostal muscles between the ribs, which may ache when expanding the chest.
To differentiate these experiences, consider the context and progression. A PE’s breathing difficulty is immediate and severe, often accompanied by symptoms like chest pain, rapid heartbeat, and coughing (sometimes with blood). It’s a medical emergency requiring immediate attention—delaying treatment can be fatal. For a pulled muscle, the discomfort evolves slowly, often after overexertion or an awkward movement. Rest and gentle stretching usually alleviate symptoms within days, and over-the-counter pain relievers like ibuprofen (200–400 mg every 6–8 hours) can help manage pain. If shortness of breath persists or worsens despite rest, or if you suspect a PE, seek urgent medical care.
Analyzing the mechanics behind these symptoms highlights why they feel so distinct. A PE disrupts the cardiovascular system, causing hypoxia (low oxygen levels) and triggering a fight-or-flight response, including rapid breathing and panic. A pulled muscle, however, is a musculoskeletal issue, where inflammation and microtears irritate nerve endings, creating a dull, throbbing pain that intensifies with activity. For muscle strains, applying ice for 20 minutes every hour during the first 48 hours reduces inflammation, followed by heat to promote healing. For PE, treatment involves anticoagulants (e.g., heparin or warfarin) to dissolve the clot and restore blood flow, emphasizing the critical need for prompt diagnosis.
Practically speaking, understanding these differences can save lives. If you experience sudden, unexplained shortness of breath, especially with risk factors like recent surgery, prolonged immobility, or a history of blood clots, assume the worst and call emergency services. For muscle pulls, monitor symptoms and use the RICE protocol (Rest, Ice, Compression, Elevation) to aid recovery. While both conditions involve breathing discomfort, the abrupt, systemic nature of PE’s shortness of breath sets it apart from the localized, activity-dependent pain of a strained muscle. Recognizing this distinction is key to responding appropriately and avoiding catastrophic outcomes.
Pulled Chest Muscle Symptoms: Pain, Tenderness, and Recovery Insights
You may want to see also
Explore related products





![]()
Leg Swelling: Deep vein thrombosis (DVT) link to PE, absent in muscle injuries
Leg swelling, particularly when unilateral and accompanied by pain or tenderness, is a red flag that demands attention. Unlike the diffuse, achy discomfort of a pulled muscle, which typically resolves with rest and ice, swelling in one leg can signal a far more serious condition: deep vein thrombosis (DVT). This occurs when a blood clot forms in a deep vein, often in the calf or thigh, and can lead to life-threatening complications if left untreated. The link between DVT and pulmonary embolism (PE) is critical—a clot can break free, travel through the bloodstream, and lodge in the lungs, causing sudden shortness of breath, chest pain, and even death. Recognizing this distinction is vital, as mistaking DVT-related swelling for a muscle injury could delay intervention and worsen outcomes.
To differentiate between leg swelling due to DVT and a pulled muscle, consider the context and symptoms. A pulled muscle usually follows overexertion or trauma, with pain localized to the strained area and improving within days. In contrast, DVT-related swelling often appears without clear cause, is confined to one leg, and may be accompanied by warmth, redness, or a heavy sensation. If you suspect DVT, immediate medical evaluation is essential. Diagnostic tools like ultrasound can confirm the presence of a clot, and treatment—typically with anticoagulants like heparin or warfarin—can prevent progression to PE. For adults over 60 or those with risk factors like obesity, smoking, or prolonged immobility, vigilance is especially crucial.
Persuasively, it’s worth emphasizing that ignoring leg swelling as a mere muscle injury can have dire consequences. While a pulled muscle rarely requires medical attention beyond rest and over-the-counter pain relievers (e.g., ibuprofen 600 mg every 6 hours), DVT demands urgent care. Anticoagulants, though effective, carry risks like bleeding, so monitoring and adherence to treatment plans are non-negotiable. Practical tips include elevating the affected leg, wearing compression stockings, and staying hydrated to reduce clot risk. If swelling persists or is paired with shortness of breath, seek emergency care immediately—it could be the difference between recovery and a fatal PE.
Comparatively, while both conditions involve leg discomfort, the absence of swelling in muscle injuries is a key differentiator. Pulled muscles may cause bruising or stiffness but rarely result in localized, unilateral swelling. DVT, however, almost always presents with swelling due to impaired blood flow. This distinction underscores the importance of assessing symptoms holistically. For instance, a 45-year-old who develops sudden leg swelling after a long flight is far more likely to have DVT than a muscle strain, given the association between prolonged sitting and clot formation. Understanding these nuances can empower individuals to act swiftly and appropriately.
Descriptively, imagine the scenario: one leg feels heavier than the other, with swelling that pits when pressed and a tightness reminiscent of a charley horse. Unlike the sharp, localized pain of a pulled muscle, this discomfort is deeper, more persistent, and often worsens with bending the foot upward. If you notice these signs, especially in the context of recent surgery, pregnancy, or a sedentary lifestyle, DVT should be your primary concern. Early intervention not only prevents PE but also reduces the risk of post-thrombotic syndrome, a chronic condition causing leg pain and swelling. In contrast, a pulled muscle’s recovery is straightforward—rest, ice, compression, and elevation (RICE) typically suffice, with no need for medical intervention unless symptoms persist beyond two weeks.
Stronger Muscles, Greater Pull: Unraveling the Science Behind Muscle Strength
You may want to see also
Explore related products





![]()
Onset Timing: Immediate PE symptoms vs. gradual muscle pain after activity
The onset of symptoms is a critical differentiator between a pulmonary embolism (PE) and a pulled muscle. While both conditions can cause chest pain, the timing and progression of discomfort are distinct. A PE often presents with immediate, intense symptoms that escalate rapidly, sometimes within minutes or hours. This sudden onset is due to the blockage of a pulmonary artery, which can cause severe hypoxia and cardiovascular stress. In contrast, a pulled muscle typically manifests as a gradual ache or stiffness that becomes noticeable after physical activity, intensifying over hours or even days as inflammation sets in.
Consider the scenario of a 45-year-old marathon runner who experiences sharp chest pain during a race. If the pain is immediate, accompanied by shortness of breath, rapid heartbeat, and dizziness, a PE should be suspected, especially if there are risk factors like prolonged immobility or recent surgery. Immediate medical attention is crucial, as untreated PEs can be life-threatening. On the other hand, if the runner notices soreness in the chest or back muscles that develops gradually after the race, worsening with movement or deep breaths, a pulled muscle is more likely. Rest, ice, and over-the-counter anti-inflammatories (e.g., ibuprofen 600 mg every 6 hours for adults) can aid recovery.
Analyzing the mechanism behind these differences highlights the importance of understanding pathophysiology. A PE occurs when a blood clot lodges in the lungs, causing an abrupt disruption in blood flow and oxygen exchange. This triggers an immediate systemic response, including pain, hypoxia, and potential cardiac strain. Conversely, a pulled muscle involves microtears in muscle fibers, leading to localized inflammation and pain that builds as the body responds to tissue damage. This gradual process explains why muscle pain often peaks 24–48 hours after injury, whereas PE symptoms are instantaneous and severe.
For practical differentiation, monitor the context and progression of symptoms. If chest pain appears suddenly, particularly at rest or with no clear trigger, seek emergency care. A PE diagnosis often involves imaging tests like a CT pulmonary angiogram. For suspected muscle strains, apply the RICE protocol (rest, ice, compression, elevation) and observe for improvement within days. Persistent or worsening symptoms in either case warrant professional evaluation, as misdiagnosis can have serious consequences. Understanding these onset patterns empowers individuals to respond appropriately, balancing vigilance with informed self-care.
Healing a Pulled Muscle Under Rib Cage: Effective Recovery Tips
You may want to see also
Explore related products





![]()
Associated Symptoms: Fever, cough, or rapid heart rate in PE, not in muscle pulls
A pulled muscle typically presents with localized pain, swelling, and tenderness, often exacerbated by movement. In contrast, a pulmonary embolism (PE) can mimic muscle strain in the chest or back but comes with distinct systemic symptoms. One key differentiator is the presence of fever, cough, or rapid heart rate, which are rare in muscle pulls but common in PE. These symptoms arise from the body’s response to a blocked lung artery, triggering inflammation and cardiovascular stress. Recognizing these associated signs is critical, as mistaking a PE for a muscle injury can delay life-saving treatment.
Fever, for instance, is virtually absent in muscle pulls but can occur in PE due to the body’s inflammatory reaction to the clot. While a low-grade fever (100–101°F) might seem benign, it should raise suspicion when paired with chest pain or shortness of breath. Similarly, a cough—especially if it produces blood-streaked mucus (hemoptysis)—is a red flag. This symptom is unheard of in muscle strains but occurs in up to 20% of PE cases, signaling lung tissue damage. Monitoring these signs, particularly in individuals over 40 or those with risk factors like recent surgery or prolonged immobility, is essential.
Rapid heart rate (tachycardia) is another telltale sign of PE, often exceeding 100 beats per minute at rest. This occurs as the heart struggles to compensate for reduced blood flow to the lungs. In contrast, a pulled muscle might cause mild tachycardia during movement but not at rest. Practical tips include using a smartwatch or pulse oximeter to track heart rate and oxygen levels, especially if chest discomfort persists. If tachycardia is accompanied by dizziness or fainting, seek emergency care immediately, as this could indicate severe hypoxia or cardiac strain.
Comparatively, muscle pulls lack these systemic markers. They are confined to the affected area, with symptoms improving within days to weeks. PE, however, demands urgent attention. A missed diagnosis can lead to complications like heart damage or death within hours. For example, a 45-year-old office worker with a "pulled chest muscle" who develops a fever, persistent cough, and heart palpitations likely has a PE, not a strain. This scenario underscores the importance of not dismissing atypical symptoms, especially in high-risk populations.
In summary, while a pulmonary embolism might initially feel like a pulled muscle, the presence of fever, cough, or rapid heart rate should prompt immediate medical evaluation. These symptoms are absent in muscle pulls but are hallmark signs of PE, reflecting the body’s distress from a blocked lung artery. Practical steps include monitoring vital signs, noting any respiratory changes, and seeking emergency care if symptoms escalate. Early recognition of these associated signs can be the difference between a misdiagnosis and timely, potentially life-saving intervention.
Immediate Effects of a Pulled Muscle: Pain, Swelling, and Recovery Steps
You may want to see also
Frequently asked questions
Yes, a pulmonary embolism can sometimes mimic the pain of a pulled muscle, especially if the clot is small or located in a specific area of the lung. However, it often comes with other symptoms like shortness of breath, chest pain, or coughing.
Pulled muscle pain typically worsens with movement or deep breaths, while pulmonary embolism pain may be sudden, sharp, and accompanied by difficulty breathing, rapid heartbeat, or coughing up blood. If in doubt, seek immediate medical attention.
Yes, it is possible for a pulmonary embolism to be initially misdiagnosed as a muscle strain, especially if the pain is mild or localized. However, the presence of other symptoms like sudden shortness of breath or chest pain should raise concern.
Yes, a pulmonary embolism can cause back pain, particularly if the clot affects the back of the lung. However, this pain is often accompanied by other symptoms like chest discomfort, rapid breathing, or lightheadedness.
Yes, if your muscle pain persists, worsens, or is accompanied by symptoms like sudden shortness of breath, chest pain, or coughing, seek immediate medical attention. A pulmonary embolism is a serious condition that requires prompt treatment.