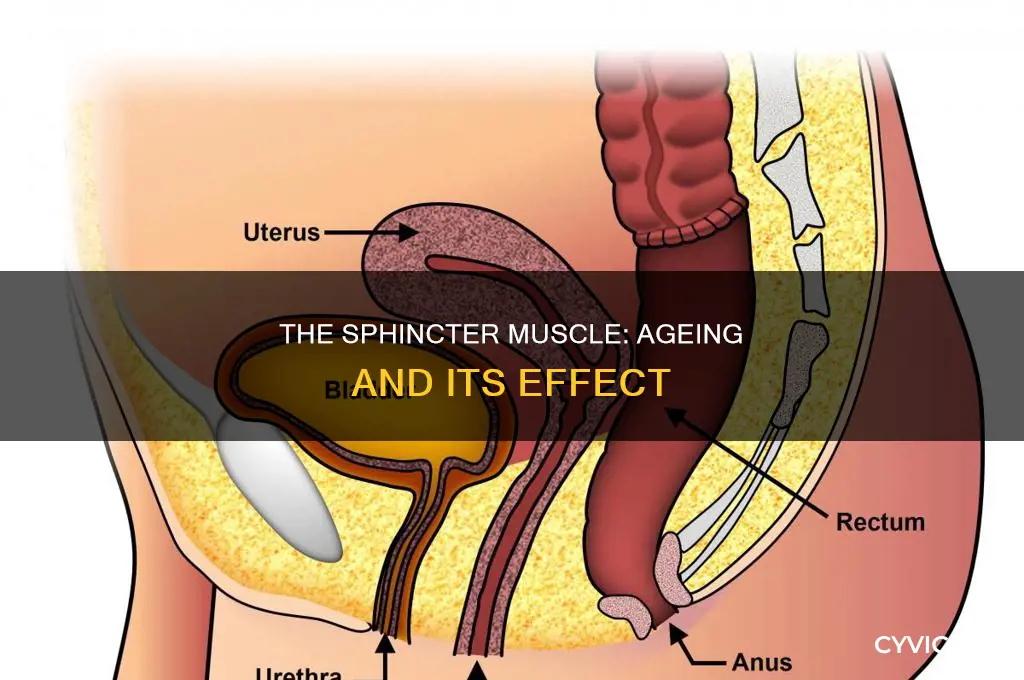
Ageing can cause the weakening of the anal sphincter muscle, leading to faecal incontinence. This condition affects between 2 and 15% of the adult population, with the prevalence increasing with age. Studies have shown that ageing alters the structure and function of the external anal sphincter muscle, leading to atrophy and fibrosis. In addition, childbirth-related injuries to the anal sphincter can also contribute to age-related sphincter dysfunction, particularly in women. The weakening of the anal sphincter muscle can result in the accidental release of liquid or solid stool, causing embarrassment and negatively impacting quality of life. Treatment options include pelvic floor exercises, muscle-strengthening techniques, and in some cases, surgery.
Explore related products






What You'll Learn
![]()
Fecal incontinence
Age is a contributing factor to fecal incontinence as it tends to weaken muscles, including the anal sphincter, which is responsible for retaining feces until an individual is ready for a bowel movement. The thickness of the internal anal sphincter (IAS) increases with age, altering the delicate balance between the tension in the wall of the sphincters, their diameter, and the closure pressure. This distortion in the anal sphincter complex can lead to fecal incontinence. Additionally, the muscles in the rectum and anus naturally weaken over time, and other nearby structures in the pelvis region loosen, resulting in impaired stool control.
Several factors influence an individual's ability to regulate bowel movements. The proper functioning of the muscles in the pelvic floor, rectum, and anus is essential for retaining and releasing stool. Nerves play a crucial role in coordinating these muscles, allowing the body to recognize when it is time to defecate. Damage to these nerves or muscles can lead to fecal incontinence. Conditions such as rectal surgery, inflammatory bowel disease, multiple sclerosis, stroke, childbirth, and diabetes can contribute to nerve or muscle damage and subsequent fecal incontinence.
Anxiety's Physical Impact: Leg Muscle Weakness Explained
You may want to see also
Explore related products





![]()
Pelvic floor exercises
As we age, the muscles in the pelvic floor, rectum, and anus naturally weaken, which can lead to fecal incontinence. Fecal incontinence can also be caused by damage to the rectum, surrounding nerves, or muscles, which may occur during childbirth or due to rectal surgery, inflammatory bowel disease, multiple sclerosis, stroke, diabetes, or constipation.
Kegel Exercises
Kegel exercises involve tightening and then releasing the muscles in your pelvic floor. To locate these muscles, try stopping the flow of urine while sitting on the toilet. You can also insert a finger into your vagina and squeeze the muscles around it. The muscles you feel lifting are the ones you want to engage during Kegel exercises. Start with a few Kegels at a time and gradually increase the number of repetitions and the length of time you hold each contraction. Consistency is key—aim to perform these exercises 2-3 times a week.
Pelvic Tilts
Pelvic tilts help strengthen the lower back and abdominal muscles, contributing to pelvic floor stability. Lie on your back with your knees bent and feet flat on the floor. Tighten your abdominal muscles and press your lower back into the floor. Hold this position for a few seconds and then release. Repeat this movement 10-15 times, gradually increasing the repetitions as your muscles strengthen.
Bridge Pose
The bridge pose targets the pelvic floor and engages the core and glute muscles. Lie on your back with your knees bent and feet hip-width apart. Place your arms at your sides, palms facing down. Inhale and lift your hips towards the ceiling, engaging your pelvic floor muscles. Hold this pose for 10-15 seconds while maintaining steady breathing. Slowly lower your hips back down and repeat for 10-15 repetitions.
Squats
Squats are excellent for working the lower body, including the pelvic floor muscles. Stand with your feet shoulder-width apart and lower your body as if sitting back into a chair, keeping your chest and back straight. Engage your pelvic floor muscles as you lower and rise. Aim for three sets of 10-15 squats, gradually increasing the intensity as you get stronger.
Bird-Dog Exercise
The bird-dog exercise activates multiple muscle groups, including the pelvic floor. Start on your hands and knees, aligning your wrists under your shoulders and your knees under your hips. Keep your back straight and engage your core muscles. Simultaneously extend and raise your left leg and right arm, maintaining a neutral body position. Hold this position for a few seconds before switching sides.
It is important to consult a healthcare professional before starting any new exercise regimen, especially if you have pre-existing health conditions. Additionally, pelvic floor physical therapy may be beneficial in some cases.
Citalopram Side Effects: Muscle Pain Explained
You may want to see also
Explore related products






![]()
Anal sphincter thickness
The anal sphincter is comprised of three muscular structures: the smooth muscle of the internal anal sphincter (IAS), the striated muscle of the external anal sphincter, and the striated puborectal muscle. The IAS is a specialised thickened terminal portion of the inner circular layer of smooth muscle of the large intestine. The thickness of the IAS is known to increase with age.
The anal sphincter is responsible for maintaining anal canal closure. The IAS plays a key role in this process, providing 55-75% of the maximum resting pressure. The striated external anal sphincter can be voluntarily used to generate additional closure pressure during large increases in abdominal pressure, such as coughing or sneezing. The internal anal sphincter has a cylindrical structure, and the tension in its circularly oriented smooth muscle produces a high-pressure zone in the anal canal.
As people age, the prevalence of fecal incontinence increases. This is due to the weakening of the anal sphincter muscles, as well as the weakening of other nearby structures in the pelvis area. Fecal incontinence can also be caused by damage to the rectum, rectal walls, or surrounding nerves, as well as by various diseases that impact bowel function, such as diabetes mellitus.
Several methods can be used to measure the thickness of the anal sphincter, including endoanal probes, vaginal ultrasound, and magnetic resonance imaging (MRI). However, measurements performed with an endoanal probe can be invasive as they alter the diameter and thickness of the sphincter. MRI has been shown to be a useful tool in measuring sphincter thickness and predicting surgical outcomes.
Muscle Spasms: A Surprising Fever Cause
You may want to see also
Explore related products






![]()
Bowel control
Ageing can cause the anal sphincter muscle to weaken and lose its tone, leading to a condition known as fecal incontinence (FI). FI is the involuntary passage of fecal matter through the anus or the inability to control bowel movements. It can cause extreme embarrassment and have a devastating impact on one's quality of life. The prevalence of FI increases with age, affecting up to 8% of adults over 65 years old and 15.3% of people over 70 years old.
The anal sphincter is composed of two muscles: the internal anal sphincter and the external anal sphincter. The internal anal sphincter is a thin white muscle wrapped around the anal canal, maintaining a resting tightness that prevents the unexpected escape of liquid or gas during rest or sleep. The external anal sphincter is composed of skeletal muscle, similar to the muscles in the arms and legs.
Age-related changes in the structure and function of the anal sphincter muscles include alterations in thickness, wall tension, and squeeze pressure. Studies have shown an increase in the thickness of the internal anal sphincter with age, which can lead to altered closure pressure. At the same time, the external anal sphincter may undergo atrophy and fibrosis, resulting in muscle dysfunction. These changes can disrupt the delicate balance of the anal canal closure mechanism, which is governed by Laplace's law.
To improve bowel control, various treatments are available, ranging from conservative to surgical approaches. Conservative treatments include:
- Pelvic floor exercises (Kegel exercises): These involve contracting and squeezing the anal sphincter muscles several times a day or when one feels fullness in the rectum. While these exercises can help, they may not always solve the problem, and consistent daily practice is necessary.
- Pelvic muscle retraining: This approach aims to strengthen the muscles, improve their resting tone, increase the ability to contract, enhance awareness of rectal fullness, and reduce accidental bowel movements.
- Dietary modifications: Increasing dietary fibre intake can bulk up the stool, making it easier to control. Legumes such as beans and lentils are excellent sources of fibre.
- Medications: Nonprescription antidiarrheal medications like loperamide (Imodium) can help with incontinence associated with diarrhea.
If conservative measures are ineffective, surgery may be considered. Surgical options include:
- Sacral nerve stimulation: This involves implanting wires into the sacral nerve in the spine to stimulate the sphincter muscle to contract. However, this method is only effective for incontinence involving solid stool and requires the patient to operate an external device and actively participate in their care.
- Sphincter repair surgery: This surgery aims to repair and tighten the sphincter muscles. It is important to assess the pudendal nerve, which supplies the external anal sphincter, before recommending this procedure.
- Colostomy: This involves bringing the end of the large intestine out through an opening in the abdomen to drain into an attached bag. While this option is rarely chosen, it can provide freedom for those who opt for it, especially those who use wheelchairs and have difficulty accessing bathrooms frequently.
Muscle Cell Dysfunction: Unraveling the Mystery of Muscular Dystrophy
You may want to see also
Explore related products






![]()
Age-related muscle atrophy
Muscle atrophy is the thinning or loss of muscle mass, which can be caused by a lack of muscle use, malnourishment, genetic disorders, consistent sitting, being bedridden, or natural ageing. Age-related muscle atrophy, also known as sarcopenia, is a common condition among people over 65 years old. It is connected to weakness, slower movement, and loss of balance, which can lead to a greater risk of falls and fractures.
The loss of muscle mass due to age-related atrophy occurs from middle age, with an average loss of 1% per year, and can lead to a total loss of up to 50% by the 8th or 9th decade of life. This loss of muscle mass and function is associated with physical frailty and an increased risk of chronic diseases and mortality. The mechanisms of muscle fibre atrophy in humans are related to imbalances in muscle protein synthesis (MPS) and breakdown (MPB). Age-related muscle atrophy occurs when muscles become resistant to anabolic stimuli, leading to impaired MPS and suppressed inhibition of MPB, resulting in the onset of atrophy.
Research has identified the prostaglandin-degrading enzyme 15-PGDH as a driver of muscle atrophy. Blocking this protein can restore the hormone prostaglandin E2, which stimulates muscle stem cells to repair tissue loss and improve mitochondrial function in mature muscle fibres, countering weakness caused by sarcopenia. While there are currently no approved treatments for sarcopenia, regular exercise and a high-protein diet can help slow or even reverse the effects of age-related muscle atrophy.
Iron Deficiency: Understanding the Link to Muscle Aches
You may want to see also
Frequently asked questions
Yes, age tends to weaken muscles, including the anal sphincter. This can lead to faecal incontinence, which is the involuntary passage of faecal matter through the anus.
Faecal incontinence can be caused by damage to the rectum, rectal walls, or surrounding nerves, as well as childbirth, surgery, inflammatory bowel disease, multiple sclerosis, stroke, diabetes, and constipation.
Faecal incontinence affects approximately 2-15% of the adult population, with up to 8% of adults over 65 years old experiencing it. It is more common in women, especially after childbirth.
Faecal incontinence can be treated with pelvic floor exercises, dietary changes, medication, or surgery. Pelvic floor exercises, also known as Kegel exercises, involve contracting and squeezing the anal sphincter muscles to strengthen them and improve resting tone. Dietary changes, such as increasing fibre intake, can help bulk up stool and make it easier to control. Medications such as antidiarrhoeals can also be used to treat diarrhoea-related incontinence. In more severe cases, surgery may be required to repair and tighten the sphincter muscles.










![Thigh Master [2026 Upgraded], 12-80LB Thigh Master Thigh Exerciser, LED Pelvic Floor Exercise Devices, 360° Inner Thigh Exerciser, Thigh Hip Trainer Kegel Excerciser with 50LB Resistance Band](https://m.media-amazon.com/images/I/61Us8eRrBEL._AC_UL320_.jpg)