Cardiac muscle, also known as the myocardium, is one of three major categories of muscles in the human body, along with smooth and skeletal muscles. Cardiac muscle is unique to the heart and is responsible for its contractility and pumping action. The heart consists of three types of muscle tissue: atrial, ventricular, and specialized muscle tissue that coordinates electrical signals through the heart. Cardiac muscle fibres conduct electrical signals and contain receptors that regulate cardiac function. These include mechanically and chemically sensitive receptors located in the atria and ventricles, as well as β-adrenergic receptors that respond to stress hormones like adrenaline and noradrenaline. The location and dynamics of these receptors play a crucial role in their function and have implications for the development of treatments for cardiac conditions.
Explore related products






What You'll Learn
![]()
Beta-adrenergic receptors in cardiac muscle
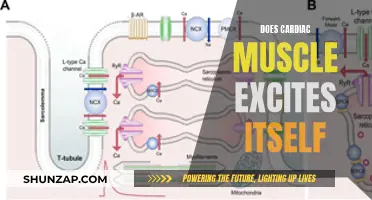
Beta-adrenergic receptors (β-ARs) are found in cardiac muscle, and they play a crucial role in regulating cardiac function and heart failure. These receptors are primarily of the β1-type (75-80%) and β2-type (20-25%) in cardiomyocytes.
The β-adrenergic receptors are G-protein coupled receptors located on the cell membrane. When activated by catecholamines such as epinephrine and norepinephrine, they initiate intracellular signalling pathways that regulate cardiac function. These signalling pathways involve positive and negative feedback loops and exhibit substantial cross-talk, allowing for a diverse range of cellular and subcellular responses.
One important function of β-adrenergic receptors in cardiac muscle is their role in excitation-contraction coupling. Compartmentalized β1-adrenergic signalling has been shown to synchronize excitation-contraction coupling without modulating individual Ca2+ sparks in healthy and hypertrophied cardiomyocytes. This signalling process helps maintain appropriate cardiac output by fine-tuning the activity of the autonomic nervous system, particularly the sympathetic system.
Additionally, β-adrenergic receptors are implicated in the pathogenesis of certain cardiovascular diseases. For example, sustained elevated activation of β-adrenergic receptors due to increased catecholamine outflow from the sympathetic nervous system can lead to abnormalities in the β-AR signalling system, contributing to conditions such as congestive heart failure (CHF). In such cases, treatment with β-blockers can improve left ventricular contractile function and reverse cardiac remodelling.
Furthermore, β-adrenergic receptor subtype signalling has been a focus of research. Studies have shown that both β1 and β2-adrenergic receptor subpopulations are involved in coupling receptor subtypes to muscle contraction. Alterations in β-adrenergic receptor subtype signalling can impact the progression of cardiomyopathy and heart failure.
Muscle Hydraulics: The Fluid Mechanics of Human Strength
You may want to see also
Explore related products






![]()
Beta1 and beta2 receptors
Beta-1 and beta-2 receptors are adrenergic receptors that are primarily responsible for signalling in the sympathetic nervous system. Beta-agonists bind to these receptors on various tissues throughout the body. Beta-1 receptors are predominantly found in the heart, kidney, and fat cells. Beta-2 receptors are found in the lungs.
Beta-1 receptors are an integral part of the normal function of the sympathetic nervous system, or the "fight or flight" system. When a person experiences fear or extreme excitement, the body quickly releases catecholamines (epinephrine and norepinephrine) that target the beta-1 receptor, along with other receptors. This increases heart rate and contractility, allowing a person to perform physical tasks that are not typically within their physiological capacity for a short duration.
Beta-2 receptors are targeted by beta-2 agonists, which are commonly used to treat chronic obstructive pulmonary disease (COPD) and asthma. These agonists bind to receptors in the lungs, relaxing the muscles in the airways and allowing them to open up. This helps individuals breathe better and get more oxygen to their body.
In the heart, targeted activation of the beta-1 receptor increases sinoatrial (SA) nodal, atrioventricular (AV) nodal, and ventricular muscular firing, thus increasing heart rate and contractility. This, in turn, increases stroke volume and cardiac output. Beta-1 receptors also have functions in the kidney and fat cells. In the kidney, they cause the release of renin from the juxtaglomerular apparatus, leading to an increase in blood volume. In fat cells, they are targeted to upregulate lipolysis.
Facial Muscles: Understanding Their Hypaxial Nature Better
You may want to see also
Explore related products






![]()
Atrial and ventricular receptors
Cardiac muscles are unique tissues located only in the heart. The heart consists of three types of muscle tissue: atrial muscle, ventricular muscle, and specialized muscle tissue that coordinates electrical signals through the heart. Cardiac muscle fibres conduct electrical signals, but they coordinate contraction locally rather than coordinating the activity of the entire heart.
Atrial receptors are innervated by myelinated vagal afferent fibres that reflexly regulate heart rate and intravascular volume. They are also known as veno-atrial stretch receptors and are low-pressure baroreceptors found in the atria of the heart. When these receptors detect an increase in blood volume in the atria, the atrial stretch triggers the release of Atrial Natriuretic Peptide (ANP), and a signal is transmitted from the receptors to the hypothalamus in the brain. The ANP causes increased natriuresis, while the hypothalamus decreases the production of vasopressin (also known as ADH, AVP, or arginine vasopressin). These receptors also cause renal vasodilation, resulting in increased diuresis, which helps to decrease blood volume and, consequently, lower blood pressure.
Stimulation of ventricular receptors can cause either reflex bradycardia and hypotension or, alternatively, excitation of the cardiovascular system. The former response is mediated by vagal afferents, whereas the latter is mediated by sympathetic (spinal) afferents. Under normal circumstances, ventricular receptors sense changes in wall motion or diastolic pressure and fine-tune the cardiovascular system. However, under pathological conditions such as coronary ischemia, which causes the release of substances like bradykinin and prostaglandins, there is an exaggerated response of the ventricular receptors.
In the context of heart failure, both atrial and ventricular receptors are reset, leading to an exaggerated neurohumoral discharge. Additionally, excessive stimulation of left ventricular receptors during exercise in patients with aortic stenosis can result in paradoxical vasodilation and syncope.
Unraveling Neurons' Power Over Muscles
You may want to see also
Explore related products






![]()
Mechanically and chemically sensitive receptors
Cardiac receptors include both mechanically and chemically sensitive receptors located in atria and ventricles. Atrial receptors are innervated by myelinated vagal afferent fibres, which reflexly regulate heart rate and intravascular volume. On the other hand, ventricular receptors can cause either reflex bradycardia and hypotension or excitation of the cardiovascular system.
Under normal circumstances, cardiac receptors sense changes in wall motion or diastolic pressure, providing fine-tuning of the cardiovascular system. Mechanically and chemically sensitive receptors in the ventricle have been described histologically and electrophysiologically.
Stimulation of ventricular receptors can also lead to an exaggerated response under certain pathological conditions, such as coronary ischemia, which causes the release of substances like bradykinin and prostaglandins. These receptors play a protective role by inducing renal vasodilation, reducing myocardial oxygen requirements, and increasing renal blood flow.
In patients with aortic stenosis, excessive stimulation of left ventricular receptors during exercise can result in paradoxical vasodilation and syncope. Additionally, in heart failure, both atrial and ventricular receptors are reset, leading to an exaggerated neurohumoral discharge.
Prevent Muscle Ache: Simple Strategies for Quick Recovery
You may want to see also
Explore related products






![]()
Ryanodine and calcium receptors
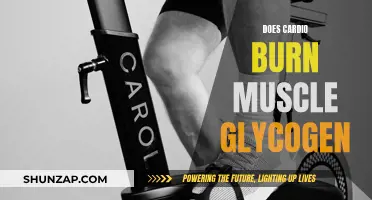
Ryanodine receptors (RyRs) are huge ion channels that release Ca2+ from the sarco/endoplasmic reticulum. They are named after the plant alkaloid ryanodine, which binds to RyRs with high affinity and specificity. The South American plant Ryania speciosa has long been recognized for its insecticidal properties, and its active compound is ryanodine. RyRs are expressed in many cell types, but their roles have only been extensively characterized in tissues where they are abundant. RyR1 is essential for excitation-contraction coupling in skeletal muscle, while RyR2 is required for the analogous signal transduction pathway in the heart.
RyR channels release calcium from internal stores during excitation-contraction coupling in muscle. Intracellular Ca2+ is an important secondary messenger for signal transduction and is essential for cellular processes such as excitation-contraction coupling (E-C coupling). The major source of intracellular Ca2+ is the sarcoplasmic reticulum (SR) in striated muscle and the endoplasmic reticulum (ER) in other cell types. There are two major Ca2+ release channels localized in the SR/ER: the ryanodine receptors (RyRs) and inositol 1,4,5-triphosphate receptors (IP3Rs).
RyR2 is involved in fatal cardiac arrhythmias and heart failure. During the prolonged plateau phase of an action potential in the cardiac muscle cell, a slow influx of Ca2+ into the cell balances the efflux of K+, thereby maintaining a stable membrane potential for about 175 ms. The incoming Ca2+ activates ryanodine receptors to trigger the release of more Ca2+.
Calcium release via ryanodine receptors can be modulated by FK-506, and Ca2+/calmodulin-dependent protein kinase modulates cardiac ryanodine receptor phosphorylation and sarcoplasmic reticulum Ca2+ leak in heart failure. Hypernitrosylated ryanodine receptor calcium release channels are leaky in dystrophic muscle.
Muscle Tears: Causes, Prevention, and Treatment Options
You may want to see also
Frequently asked questions
Cardiac receptors include both mechanically and chemically sensitive receptors located in atria and ventricles. They regulate heart rate and intravascular volume and may protect the heart and kidney by lessening myocardial oxygen requirements.
There are two different subtypes of beta adrenergic receptors in the heart: beta1 and beta2. Both are activated by the stress hormones adrenaline and noradrenaline and trigger the strongest stimulation of the strength and frequency of the heart rate.
Beta1 receptors are found on the entire surface of heart muscle cells, while beta2 receptors are found exclusively in specific structures in these cells called T-tubules. Beta1 receptors can elicit a number of persistent changes and are endowed with the ability to initiate the often-detrimental growth of the heart muscle cell. Beta2 receptors have a much narrower range of functionality and are limited to direct and short-term stimulation of the heart.