Nicotine is a highly addictive substance found in cigarettes and vaping products. While nicotine does not directly affect muscle contractions, it has been shown to alter sensitivity to muscle tension and impair muscle recovery from injury. The effects of nicotine on muscle tension have been studied in both human and animal models, with conflicting results. Some studies suggest that nicotine may not be the main culprit in acute vascular dysfunction, but its long-term effects on muscle function and recovery are still not fully understood.
| Characteristics | Values |
|---|---|
| Does nicotine cause muscle tension? | Nicotine does not directly cause muscle tension, but it does alter sensitivity to muscle tension. |
| Smoking and muscle tension | Smoking can alter the sensitivity to muscle activity, particularly in female smokers. |
| Nicotine replacement and muscle tension | A study found a significant difference in sensitivity to muscle tension in subjects given nicotine gum compared to those given no nicotine replacement during withdrawal. |
| Nicotine and microvascular responses | Studies on mice suggest that nicotine-containing e-cigarette aerosol impairs skeletal muscle force development and prevents recovery from injury. |
| Nicotine and vascular dysfunction | Evidence indicates that e-cigarettes are not safer than traditional cigarettes in terms of the user's risk of developing vascular dysfunction or disease. |
| Nicotine and cardiovascular disease | E-cigarettes have been shown to produce similar significant and adverse changes to vascular structure and function as traditional cigarettes, indicating a potential risk for cardiovascular disease. |
Explore related products






What You'll Learn
![]()
Nicotine chewing gum and muscle tension
Nicotine is a chemical compound found naturally in tobacco and certain plants. When ingested, nicotine enters the bloodstream and releases dopamine in the brain, creating a short-lived "feel good" effect.
Nicotine does not directly affect the muscles, as muscle proteins are not very sensitive to nicotine. However, nicotine affects brain proteins that are nearly identical to receptor proteins on muscle cells that signal them to contract.
Smoking has been shown to alter the sensitivity to muscle activity in female smokers. A study examined the effects of smoking cessation and nicotine replacement on sensitivity to muscle tension. Twenty-five women were randomly divided into two groups: one group received nicotine chewing gum during the withdrawal period, while the other group received no nicotine replacement. The results showed a significant difference in sensitivity between the two groups, supporting the hypothesis that nicotine alters sensitivity to muscle tension.
Nicotine gum is used as a smoking cessation aid, providing a low dose of nicotine without the harmful smoke and toxins found in cigarettes. However, it can cause side effects such as mouth or throat irritation, bad aftertaste, nausea, hiccups, jaw pain, racing heartbeat, stomach upset, and dizziness. To use nicotine gum effectively, it should be chewed a few times and then tucked between the cheek and gums, allowing the nicotine to absorb directly into the bloodstream rather than the stomach.
Amitriptyline and Muscle Stiffness: What's the Link?
You may want to see also
Explore related products






![]()
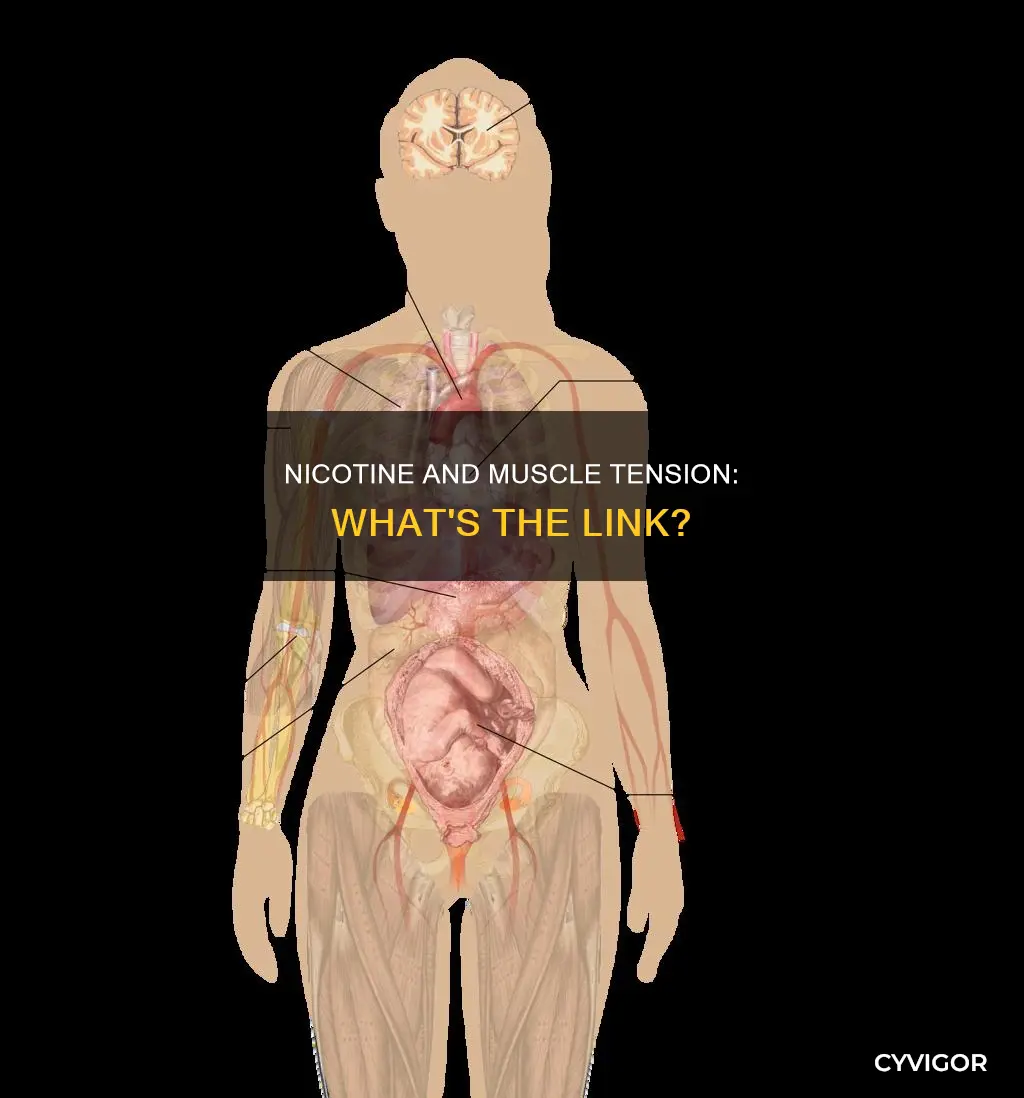
Nicotine's impact on microvascular responses in skeletal muscle
While nicotine does not directly impact muscle cells, it has been shown to alter sensitivity to muscle tension. A study on female smokers found that nicotine chewing gum during withdrawal altered sensitivity to muscle tension compared to those who did not receive nicotine replacement.
Novel tobacco products, such as heated tobacco and electronic cigarettes (e-cigarettes or e-cigs), have become increasingly popular over the last 15 years. The e-cigarette market is driven by claims that e-cigarettes are a safer alternative to traditional smoking. However, the health effects of e-cigarettes are not yet fully understood, especially regarding their impact on microvascular health.
Despite claims of harm reduction, emerging evidence suggests that e-cigarettes are not necessarily safer than traditional cigarettes in terms of vascular dysfunction and disease. E-cigarettes differ from regular cigarettes in that users can customize the e-liquid composition, including the base solution, flavors, and nicotine level. The effects of e-cigarettes on microvascular responses in skeletal muscle are not well understood, and acute exposure studies are needed to evaluate the individual components of e-liquid on vascular tone and endothelial function.
Studies have found that arteriole responses in a peripheral vascular bed respond rapidly (within 15 minutes) to the inhalation of cigarette smoke and e-cigarette aerosol. The vascular responses are similar between cigarettes and e-cigarettes, indicating that e-cigarettes can lead to similar risks for cardiovascular disease as seen with smoking. However, the peripheral skeletal muscle vasoconstriction response triggered by e-cigarettes is not mediated by nicotine. Instead, other compounds or chemicals in the delivery vehicle are likely responsible for triggering peripheral vasoconstriction in skeletal muscle.
Thyroid Disorders: Muscle Pain and Stiffness Explained
You may want to see also
Explore related products






![]()
Nicotine's effect on muscle repair and recovery
Nicotine does not directly affect muscles as they are not very sensitive to it. However, nicotine affects the brain proteins that are nearly identical to a receptor protein on muscle cells that tells them to contract.
A study on the effects of nicotine chewing gum on muscle tension showed that nicotine alters sensitivity to muscle tension. Another study on the microvascular responses in skeletal muscle from acute exposure to cigarettes and vaping showed that nicotine-containing aerosol reduced the maximal force produced by the extensor digitorum longus (EDL) by 30-40% and the speed achieved in treadmill running by 8%.
Chronic exposure to nicotine-containing e-cigarette aerosol decreased catecholamines, both epinephrine and norepinephrine, in the adrenal gland and increased circulating plasma catecholamines. This may alter whole-body catecholamine homeostasis by increasing norepinephrine and epinephrine release into the plasma from the adrenal glands or decreasing catecholamine clearance due to lower muscle and liver catecholamine action.
Nicotine-containing aerosol also decreased running speed by 11% and prevented full recovery from a lengthening contraction protocol (LCP) injury. In nicotine aerosol-exposed mice, muscle regenerating from overuse injury only recovered force to 80% of non-injured levels. These data suggest that nicotine may prevent full muscle recovery and repair.
Gatorade and Muscle Cramps: What's the Connection?
You may want to see also
Explore related products






![]()
Nicotine's influence on muscle sensitivity
Nicotine is a highly addictive substance found in cigarettes and vaping products. While nicotine does not directly affect muscle proteins, it has been shown to alter sensitivity to muscle tension.
A study on female smokers found that nicotine chewing gum during the withdrawal period significantly impacted muscle tension sensitivity. This suggests that nicotine does play a role in altering muscle sensitivity, even if it does not directly cause contractions.
The mechanism behind nicotine's influence on muscle sensitivity is not fully understood, but it may be related to its interaction with acetylcholine, a neurotransmitter. Acetylcholine is involved in transmitting signals between nerve cells and muscle cells, and nicotine interferes with these signals by binding to acetylcholine receptors. This interference may contribute to the altered sensitivity to muscle activity observed in smokers.
Furthermore, nicotine-containing aerosols in e-cigarettes have been shown to impair skeletal muscle force development and prevent recovery from injury in male mice. The nicotine aerosol exposure decreased catecholamines in the adrenal gland while increasing circulating plasma catecholamines. This alteration in catecholamine homeostasis may be a factor in nicotine's influence on muscle sensitivity and recovery.
While nicotine does not directly cause muscle tension, the available research indicates that it does modify muscle sensitivity and recovery capabilities. The exact mechanisms behind these effects require further investigation, particularly regarding the role of neurotransmitters and the body's catecholamine balance.
Exercise and Muscle Twitching: What's the Connection?
You may want to see also
Explore related products






![]()
Nicotine and vascular dysfunction
Nicotine, the addictive component of tobacco products, has been shown to alter vasoreactivity through endothelium-dependent and/or independent mechanisms, leading to vascular dysfunction. This alteration in vasoreactivity can cause a reduction in blood flow in microvascular beds, potentially impairing wound healing, macular degeneration, progressive renal disease, and placental dysfunction during pregnancy.
Nicotine affects the proliferation, migration, and matrix production of vascular endothelial and vascular smooth muscle cells, inducing vascular remodeling. It also reduces the bioavailability of nitric oxide (NO) by decreasing endothelial NO synthase (eNOS) expression and phosphorylation levels. This reduction in NO bioavailability can lead to endothelial dysfunction and the generation of superoxide.
Additionally, nicotine has been found to induce neurogenic vascular relaxation in multiple vascular beds. Stimulation of nicotinic acetylcholine receptors (nAChR) on perivascular sympathetic nerves causes the release of norepinephrine (NE), which induces NO production in neighboring chronic nerves, resulting in nitrergic dilation of cerebral arteries. However, chronic exposure to nicotine can lead to oxidative stress, endothelial dysfunction, and hypoperfusion of the cerebral arteries.
While nicotine alone may not be the primary cause of vascular dysfunction, its role in the development of cardiovascular disease (CVD) is still a concern, especially for individuals with existing cardiovascular issues. The use of electronic cigarettes (e-cigs) and vaping has increased due to the perception of reduced harm compared to traditional cigarettes. However, evidence suggests that these alternatives are not necessarily safer and can lead to similar vascular dysfunction and adverse vascular outcomes.
Furthermore, nicotine has been shown to promote the growth of new blood vessels, or angiogenesis, which may stimulate tumor growth and contribute to cardiovascular disease. While nicotine replacement therapy is used to help smokers quit, caution is advised due to the potential risks associated with nicotine's impact on vascular function and overall cardiovascular health.
Mold Infection and Muscle Fatigue: Is There a Link?
You may want to see also
Frequently asked questions
Nicotine does not directly cause muscle tension. However, it has been shown to alter sensitivity to muscle activity in female smokers.
Nicotine affects the brain proteins that are nearly identical to a receptor protein on muscle cells that tells them to contract. However, nicotine does not directly affect muscles as they are not very sensitive to nicotine.
Yes, nicotine can affect microvascular responses in skeletal muscle. Studies have shown that nicotine-containing aerosol impairs locomotor muscle function, limits exercise tolerance, and interferes with muscle repair.
Nicotine vaping can cause muscle tension indirectly. While nicotine is not the culprit, vaping devices use polyethylene glycol and vegetable glycerin to dissolve nicotine, which decreases running speed and prevents full recovery from muscle injuries.